


124 Vasodilators
Organic Nitrates
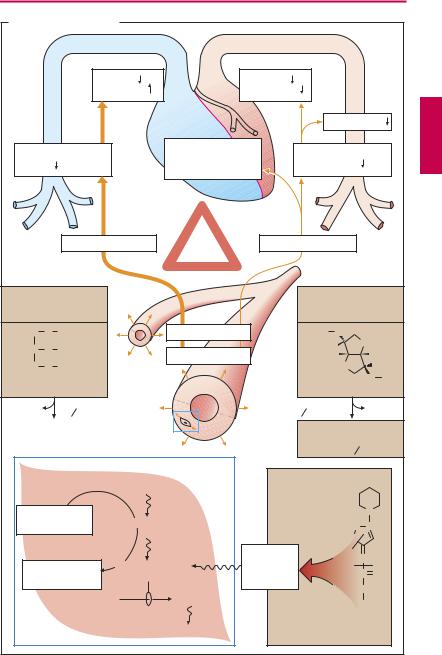
Various esters of nitric acid (HNO3) and polyvalent alcohols relax vascular smooth muscle, e.g., nitroglycerin (glyceryl trinitrate) and isosorbide dinitrate. The effect is more pronounced in venous than in arterial beds.
These vasodilator effects produce hemodynamic consequences that can be put to therapeutic use. Owing to a decrease in both venous return (preload) and arterial afterload, cardiac work is decreased (p.318). As a result, the cardiac oxygen balance improves. Spasmodic constriction of larger coronary vessels (coronary spasm) is prevented.
Uses. Organic nitrates are used chiefly in angina pectoris (p.316), less frequently in severe forms of chronic and acute congestive heart failure. Continuous intake of higher doses with maintenance of steady plasma levels leads to loss of ef cacy, inasmuch as the organism becomes refractory (tachyphylactic). This “nitrate tolerance” can be avoided if a daily “nitrate-free interval” is maintained, e.g., overnight.
At the start of therapy, unwanted reactions occur frequentlyin the formofathrobbing headache, probably caused by dilation of cephalic vessels. This effect also exhibits tolerance, even when daily “nitrate pauses” are observed. Excessive dosages give rise to hypotension, reflex tachycardia, and circulatory collapse.
Mechanism of action. The reduction in vascular smooth muscle tone is due to activation of guanylate cyclase and elevation of cyclic GMP levels. The causative agent is nitric oxide (NO) generated from the organic nitrate. NO is a physiological messenger molecule that endothelial cells release onto subjacent smooth muscle cells (“endothe- lium-derived relaxant factor,” EDRF). Organic nitrates thus utilize a physiological pathway; hence their high ef cacy. The enzymatically mediated generation of NO from
organic nitrates (via a mitochondrial aldehyde dehydrogenase) within the smooth muscle cell depends on a supply of free sulfhydryl (–SH) groups; “nitrate-tolerance” is attributed to a cellular exhaustion of SH donors.
Nitroglycerin (NTG) is distinguished by a high membrane penetrability and very low stability. It is the drug of choice in the treatment of angina pectoris attacks. For this purpose, it is administered as a spray, or in sublingual or buccal tablets for transmucosal delivery. The onset of action is between 1 and 3 minutes. Due to a nearly complete presystemic elimination, it is poorly suited for oral administration. Transdermal delivery (nitroglycerin patch) also avoids presystemic elimination.
Isosorbide dinitrate (ISDN) penetrates wellthroughmembranes,ismorestablethan NTG, and is partly degraded into the weaker, but much longer acting, 5-isosorbide mononitrate (ISMN). ISDN can also be applied sublingually; however, it is mainly administered orally in order to achieve a prolonged effect. ISMN is not suitable for sublingual use because of its higher polarityandslower rate of absorption. Taken orally, it isabsorbed and is not subject to first-pass elimination.
Molsidomine itself is inactive. After oral intake, it is slowly converted into an active metabolite, linsidomine. The differential effectiveness in arterial vs. venous beds is less evident compared to the drugs mentioned above. Moreover, development of “nitrate tolerance” is of less concern. These differencesinactivityprofileappeartoreflectadifferent mechanism of NO release. The same applies to the following sodium nitroprusside.
Sodium nitroprusside contains a nitroso (–NO) group, but is not an ester. It dilates venousand arterial beds equally. It is administered by infusion to achieve controlled hypotension under continuous close monitoring. Cyanide ions liberated from nitroprusside can be inactivated with sodium thiosulfate (p.310).
|
|
|
|
|
|
|
Organic Nitrates |
|
|
|
125 |
||
A. Vasodilators: Nitrates |
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
Preload |
|
Afterload |
|
|
|
|
|
|
|
|
|
|
|
O2-supply |
|
O2-demand |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Blood pressure |
||||
Venous blood return |
|
Prevention of |
|
|
Peripheral |
|
|
||||||
|
coronary artery |
|
|
|
|
||||||||
to heart |
|
|
|
|
|
|
resistance |
|
|
||||
|
|
|
|
spasm |
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Venous bed |
“Nitrate |
Arterial bed |
|
|
|
|
|||
|
|
|
|
|
|
tolerance” |
|
|
|
|
|
|
|
Route: |
|
|
|
|
|
|
|
Route: |
|
|
|
|
|
e.g., sublingual, |
|
|
|
|
e.g., sublingual, |
||||||||
transdermal |
|
|
|
|
|
oral, transdermal |
|||||||
H2C |
O |
NO2 |
|
|
|
Vasodilation |
|
|
O2N O |
|
|
O |
|
HC |
O |
NO2 |
|
|
|
|
|
|
H |
5 |
|
||
|
|
|
“Nitrates” |
|
|
|
|
|
H |
||||
|
|
|
|
|
|
|
|
H |
4 |
3 |
|
||
H2C O NO2 |
|
|
|
|
|
|
O 1 |
2 |
H |
||||
Glyceryl trinitrate |
|
|
|
|
|
|
|
|
O NO2 |
||||
Nitroglycerin |
|
|
|
|
|
Isosorbide dinitrate |
|||||||
NO |
|
t 1 |
2 |
~ 2 min |
|
|
t 1 |
2 |
~ 30 min |
|
|
|
NO |
|
|
|
|
|
|
|
|
|
|
|
|
||
Inactivation |
|
|
|
5-Isosorbide mono- |
|||||||||
|
|
|
|
|
|
|
nitrate, an active meta- |
||||||
|
|
|
|
|
|
|
bolite |
t 1 2 ~ 240 min |
|||||
|
|
|
|
|
R – O – NO2 |
|
|
|
|
|
|
|
|
SH-donators |
|
|
Release of NO |
|
|
|
|
|
|
N |
|||
e.g., glutathione |
|
|
|
–N |
|
N+ |
|||||||
|
|
|
|
|
|
|
|
|
|
O |
|
|
|
|
|
|
|
|
|
|
Active |
|
|
2 |
|
N |
|
Consumption |
Activation of |
|
|
|
1 |
|
|
||||||
|
metabolite |
|
|
|
C |
O |
|||||||
guanylate cyclase |
|
|
|
|
|||||||||
of SH donors |
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
O |
|
|
|
|
|
GTP |
|
cGMP |
|
|
|
|
|
C2H5 |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Smooth mucle cell |
|
Relaxation |
|
|
Molsidomine |
|
||||||
|
|
|
|
(precursor) |
|
|
|
||||||

126 Vasodilators
Calcium Antagonists
During electrical excitation of the cell membrane of heart or smooth muscle, different ionic currents are activated, including an inward Ca2+ current. The term Ca2+ antagonist is applied to drugs that inhibit the influx of Ca2+ ions without affecting inward Na+ or outward K+ currents to a significant degree. Other labels are calcium entry blocker or
Ca2+-channel blocker. Ca2+ antagonists used therapeutically can be divided into three groups according to their effects on heart and vasculature.
I. Dihydropyridine Derivatives
The dihydropyridines, e.g., nifedipine, are uncharged hydrophobic substances. They particularly induce a relaxation of vascular smooth muscle in arterial beds. An effect on cardiac function is practically absent at therapeutic dosage. (In pharmacological experiments on isolated cardiac muscle preparations, a clear negative inotropic effect is, however, demonstrable at high concentrations.) They are thus regarded as vasoselective Ca2+ antagonists. Because of the dilation of resistance vessels, blood pressure falls. Cardiac afterload is diminished (p.318) and, therefore, also oxygen demand. Spasms of coronary arteries are prevented.
Indications. An indication for nifedipine is angina pectoris (p.318). In angina pectoris, it is effective when given either prophylactically or during acute attacks. Adverse effects are palpitation (reflex tachycardia due to hypotension), headache, and pretibial edema.
The successor substances principally exert the same effects, but have different kinetic properties (slow elimination and, hence, steady plasma levels).
Nitrendipine, isradipine, and felodipine are used in the treatment of hypertension. Nicardipine and nisoldipine are also used in angina pectoris. Nimodipine is given prophylactically after subarachnoidal hemorrhage to prevent vasospasms. On its dihydropyri-
dine ring, amlodipine possesses a side chain with a protonatable nitrogen and can therefore exist in a positively charged state. This influences its pharmacokinetics, as evidenced by the very long half-life of elimination (~ 40 hours).
II. Verapamil and Other Catamphiphilic Ca2+ Antagonists
Verapamil contains a nitrogen atom bearing a positive charge at physiological pH and thus represents a cationic amphiphilic molecule. It exerts inhibitory effects not only on arterial smooth muscle, but also on heart muscle. In the heart, Ca2+ inward currents are important in generating depolarization of sinoatrial node cells (impulse generation), in impulse propagation through the AVjunction (atrioventricular conduction), and in electromechanical coupling in the ventricular cardiomyocytes. Verapamil thus produces negative chronotropic, dromotropic, and inotropic effects.
Indications. Verapamil is used as an antiarrhythmic drug in supraventricular tachyarrhythmias. In atrial flutter or fibrillation, it is effective in reducing ventricular rate by virtue of inhibiting AV conduction. Verapamil is also employed in the prophylaxis of angina pectoris attacks (p.318) and the treatment of hypertension (p.314).
Adverse effects. Because of verapamil’s effects on the sinus node, a drop in blood pressure fails to evoke a reflex tachycardia. Heart rate hardly changes; bradycardia may even develop. AV-block and myocardial insuf ciency can occur. Patients frequently complain of constipation, because verapamil also inhibits intestinal musculature.
Gallopamil (= methoxyverapamil) is closely related to verapamil in terms of both structure and biological activity.
Diltiazem is a catamphiphilic benzothiazepine derivative with an activity profile resembling that of verapamil.
|
|
|
|
|
|
Calcium Antagonists |
127 |
||
A. Vasodilators: calcium antagonists |
|
|
|
|
|
||||
Smooth muscle cell |
|
|
|
|
|
|
|
||
|
|
|
|
|
|
Afterload |
|
|
|
|
|
|
|
|
|
O2-demand |
|
|
|
|
|
|
|
|
|
|
Blood pressure |
||
Contraction |
|
|
|
|
|
|
|
||
|
|
|
|
Inhibition of |
|
Peripheral |
|
||
|
|
|
|
|
resistance |
|
|||
|
|
|
|
coronary spasm |
|
||||
|
|
|
|
|
|
|
|||
Ca2+ |
|
|
|
|
|
|
|
|
|
|
|
|
|
Arterial |
|
|
|
|
|
|
|
|
|
blood vessel |
|
|
|
|
|
|
|
|
Vasodilation in arterial bed |
|
|
|
|||
|
|
|
|
Na+ Ca2+10-3M |
|
|
|
|
|
|
|
|
depolarization |
|
|
O |
CH3 |
|
|
|
|
|
|
|
H3CO |
O |
CH3 |
|
|
|
|
NO2 |
|
|
H3C |
|
O |
CH3 |
|
H3C O C H |
|
|
|
|
|
O CH3 |
|||
|
C O CH3 |
Ca2+10-7M |
K+ |
HC C C N |
|
||||
O |
|
O |
H3C H2C |
|
|
|
|||
H3C |
N |
CH3 |
Membrane |
|
|
H2C |
|
CH2 |
|
|
H |
|
Selective |
|
H2C + |
C |
|
||
|
|
|
inhibition of |
|
|
N |
H2 |
|
|
|
|
|
|
|
H3C |
H |
|
||
|
|
|
calcium influx |
|
|
||||
|
|
|
|
|
|
|
|||
Nifedipine |
|
|
|
|
|
Verapamil |
|
|
|
(dihydropyridine derivative) |
|
|
|
(cationic-amphiphilic) |
|||||
|
|
|
Inhibition of cardiac functions |
|
|
|
|||
|
|
|
|
|
|
Impulse |
Heart rate |
|
|
|
|
|
Sinus node |
|
generation |
Reflex tachycardia |
|||
|
|
|
|
|
|
|
with nifedipine |
||
Ca2+ |
|
|
|
|
|
|
|
|
|
|
|
Ca2+ |
|
|
|
Impulse |
AV- |
|
|
|
|
AV-node |
|
|
conduction |
conduction |
|
||
|
|
|
|
|
|
||||
|
|
Ca2+ |
|
|
|
|
|
|
|
Ca2+ |
|
|
|
|
|
|
|
|
|
|
|
|
|
Ventricular |
Electro- |
Contractility |
|||
|
|
|
|
mechanical |
|||||
|
|
|
|
muscle |
|
||||
|
|
|
|
|
coupling |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Heart muscle cell |
|
|
|
|
|
|
|
||