47.Sleisenger MH, Fordtran JS, editors. Gastrointestinal Disease. Philadelphia: Saunders; 1983. p 1599–1616.
48.Sleisenger MH, Fordtran JS, editors. Gastrointestinal Disease. Philadelphia: Saunders; 1983. p 1617–1626.
49.Silvis SE, editor. Therapeutic Gastrointestinal Endoscopy. New York: Igaku-Shoin; 1985. p 241–268.
50.Huizinga E. On esophagoscopy and sword swallowing. Ann Otol Rhinol Laryngol 1969;78:32–34.
51.Shaheen N, Ransohoff DF. Gastroesophageal reflux, Barrett esophagus, and esophageal cancer: scientific review. JAMA 2002;287:1972–1981.
52.Spechler SJ. Clinical practice. Barrett’s Esophagus. N Engl J Med 2002;346:836–842.
53.Sampliner RE. Updated guidelines for the diagnosis, surveillance, and therapy of Barrett’s esophagus. Am J Gastroenterol 2002;97:1888–1895.
54.Wolfsen HC, Hemminger LL, DeVault KR. Recurrent Barrett’s esophagus and adenocarcinoma after esophagectomy. BMC Gastroenterology 2004;4:18.
55.Jean M, Dua K. Barrett’s Esophagus: Best of Digestive Disease Week 2003. Curr Gastroenterol Rep 2004;6:202– 205.
56.Hunt RH, Waye JD, editors. Colonoscopy. London: Chapman & Hall; 1981. p 11–18.
57.Ohligisser M, Sorokin Y, Hiefetz M. Gynecologic laparoscopy, a review article. Obstet Gynecol Surv 1985;40:385–396.
58.Robinson HB, Smith GW. Application for laparoscopy in general surgery. Surg Gynecol Obstet 1976;143:829–834.
59.Devaux BC, Joly L, Page P, Nataf F, Turak B, Beuvon F, Trystram D, Roux F. Laser-assisted endoscopic third ventriculostomy for obstructive hydrocephalus: Technique and results in a series of 40 consecutive cases. Lasers Surg Med 2004;34:368–378.
60.Cram GP, Copeland ML. Nucl Instrum Methods Phys Rev B 1998;144:256.
61.Edwards G et al. Free-electron-laser-based biophysical and biomedical instrumentation. Rev Sci Instrum 2003;74:3207– 3245.
62.Paparella MM, Shumrick DA, editors. Otolaryngology Philadelphia: W.B. Saunders; 1980. p 2410–2430.
63.Ballenger JJ, editor. Diseases of the Nose, Throat, Ear, Head, and Neck. Philadelphia: Lea & Febiger; 1985. p 1293–1330.
64.Steiner W. Techniques of diagnostic and operative endoscopy of the head and neck. Endoscopy 1979;1:51–59.
65.Vaughan CW. Use of the carbon dioxide laser in the endoscopic management of organic laryngeal disease. Otolaryngol Clin North Am 1983;16:849–864.
66.Pfalz R, Hibst R, Bald N. Suitability of different lasers for operations ranging from the tympanic membrane to the base of the stapes. Adv in Oto-Rhino-Laryngol 1995;49:87–94.
67.Schade G, Leuwer R, Kraas M, Rassow B, Hess M. Laryngeal morphometry with a new laser ‘clip on’ device. Lasers Surg Med 2004;34:363–367.
68.Future Trends in Medical Device Technology: Results of an Expert Survey. Available at http://www.fda.gov/cdrh/ost/ trends/TOC.html.
Further Reading
Ponsky JL. Atlas of Surgical Endoscopy. St. Louis (MO): MosbyYear Book; 1992.
Barkin J, O’Phelan C, editors. Advanced Therapeutic Endoscopy. New York: Raven Press; 1990.
Ovassapian A. Fiberoptic Airway Endoscopy in Anesthesia and Critical Care. New York: Raven Press; 1990.
Niemz M. Laser-Tissue Interactions: Fundamentals and Applications. 2nd ed. Berlin Heidelberg: Springer-Verlag; 2002.
ENGINEERED TISSUE |
189 |
Infrared Fiber Systems. Available at http://www.infraredfibersy stems.com.
Polymicro Technologies, LLC. Available at http://www.polymicro. com.
Omniguide Communications, Inc. Available at http://www.omniguide.com.
LightLab Imaging, Inc. Available at http://www.lightlabimaging. com.
Given Imaging. Available at www.givenimaging.com.
Intuitive Surgical, Inc. Available at www.intuitivesurgical.com.
See also ESOPHAGEAL MANOMETRY; FIBER OPTICS IN MEDICINE; MINIMALLY INVASIVE SURGERY.
ENGINEERED TISSUE
GREGORY E. RUTKOWSKI
University of Minnesota-Duluth
Duluth, Minnesota
INTRODUCTION
History of Tissue Engineering
In 1988, researchers gathered at the Granlibakken Resort in Lake Tahoe, CA under the sponsor ship of the National Science Foundation (NSF) to develop the fundamental principles of tissue engineering as an emerging technology. Based on an earlier proposal by Dr. Y.C. Fung to develop an Engineering Research Center focused on the engineering of living tissues, NSF held several meetings that led to the decision to designate tissue engineering as a new emerging field. A formal definition was finally agreed upon at the Granlibakken workshop. Based on this meeting, tissue engineering is defined as ‘‘the application of the principles and methods of engineering and the life sciences toward the fundamental understanding of structure–function relationships in normal and pathological mammalian tissues and the development of biological substitutes to restore, maintain, and improve function’’ (1). This was further refined in 1992 by Eugene Bell who developed a list of more specific goals:
1. Providing cellular prostheses or replacement parts for the human body.
2. Providing formed acellular replacement parts capable of inducing regeneration.
3. Providing tissue or organ-like model systems populated with cells for basic research and for many applied uses such as the study of disease states using aberrant cells.
4. Providing vehicles for delivering engineered cells to the organism.
5. Surfacing nonbiological devices (2).
These discussions eventually culminated in the pioneering review article by Langer and Vacanti in 1993 (3). The general strategies to create engineered tissue would include the isolation of cells or cell substitutes, the use of tissue-inducing substances, and development of threedimensional (3D) matrices on which to grow tissue.
190 ENGINEERED TISSUE
Much of tissue engineering owes its beginnings to reconstructive surgery and internal medicine. In the sixteenth century, Gaspare Tagliacozzi developed a method for nasal reconstruction using flaps of skin taken from the arm and grafted onto the injury site (4). With the scientific development of the germ theory of disease and the sterile techniques that were introduced, modern surgery became established as a means to treat patients with internal injuries. In the late nineteenth century, surgeons used veins and arteries as conduits to enhance the nerve regeneration (5). World War I saw improvements in reconstructive surgery as doctors were able to hone their skills due to the number of soldiers injured in battle. Reconstructive surgery had it limitations in terms of the availability of biological material. By the 1940s, much progress had been made in understanding the function of the immune system is accepting tissue from a donor. This eventually led to the first successful organ transplant (kidney) in 1954. The next 50 years, would see tremendous advances in organ transplants as well as in immunosuppressive drug therapy.
An alternative to organ transplant has been the development of artificial devices to mimic biological function. The mid-nineteenth century also saw the rise in the use of prosthetic limbs that would initiate the use of artificial devices to replace biological functions. Artificial limbs were used as far back as the Dark Ages to assist knights heading off to battle. The intervening centuries saw improvements over such devices through the use of stronger, lighter materials, and a better understanding of biomechanics
(6). Besides limbs, artificial devices have also been invented to replace the function of certain internal organs. The dialysis machine was created in the 1940s to assist patients with acute renal failure. In 2001, an implantable artificial heart was first used in a human. While many advances have been made in artificial devices, some of the drawbacks include the breakdown of the artificial materials, a lack of interaction with the human body, and the inability to self-renew.
The modern era of tissue engineers seeks to overcome the limitations of reconstructive surgery, organ transplantations, and prosthetic devices by creating functional, completely biocompatible tissues and organs. Since the late 1980s, the field of tissue engineering has grown exponentially and continues to draw scientists from diverse fields, from the biological and medical sciences to engineering and materials science.
THEORY
Tissue engineering adds to the modern health care system by providing the tools to assist in the repair of tissue and organs damaged by injury and disease. An exact replica of the tissue could potentially be grown in the lab and later inserted into the patient. Alternatively, precursors may be placed in the body with the expectation that it will develop into fully formed functional tissue. Also, devices may be implanted into the body to encourage the regeneration of already existing tissue in the body.
Engineered tissue is created by combining relevant cells and chemical factors within a 3D matrix that serves as a
. .. .. ......... .
.. . . . .. . .. .
Engineered
Tissue
Cells |
Scaffold |
. .. .. ......... .
.. . . . .. . .. .
Chemical
Factors
Figure 1. Basic components of engineered tissue.
scaffold (Fig. 1). Sterile cell culture techniques allows for the expansion of cells in vitro to obtain sufficient quantities for use in engineered tissue. Cells can originate from the patient, another donor, or even animal tissue. As our understanding of biochemical cues during development expands, tissue formation can be better controlled through the delivery of pertinent growth factors or through the interaction of complex multiple cell cultures. Scaffold materials may be biological (collagen, extra cellular matrix) or synthetic. Synthetic materials can be designed to mimic the extra cellular matrix and may be infused with chemical factors to support tissue regeneration. Since the discovery and availability of synthetic polymers in the 1940s, scientific advances have made these materials biodegradable and biocompatible.
Cellular Processes
During the formation of tissue, either during development or in the lab, cells undertake many different processes. In order to maintain the integrity of the tissue, the cells tissue must adhere to others as well as to the surrounding matrix material. Certain cells must migrate through the 3D space in order to properly position themselves within the tissue. Once in position, they must also continue to multiply to provide adequate tissue growth. Vascularization and innervation of the tissue is required to complete integration of the engineered tissue with its surroundings. Tissue derived from donor material also has immune concerns.
Development. Engineered tissue is best created by mimicking the processes that occur during development
(7). Following fertilization, the zygote divides until the blastocyst is formed. The early embryonic tissue is comprised of two cell phenotypes: epithelial cells and migratory mesanchymal cells. The transformation between these cells is regulated by growth factors, the extra cellular matrix, and intracellular signaling. As the embryo develops, these cells will become diversified as they commit to various tissue forms. These cells will eventually differentiate into the various cell types found in the body.
Morphogenesis describes the cascade of events that leads to the spatial pattern formation of the developing
embryo. Regeneration of tissue mimics this process. Specific chemical factors, called morphogens, provide information on the pattern via diffusion. The combination of various morphogens due to diffusion leads to complex pattern formation. One well-studied example is the development of bone. Several bone morphogenic factors have been isolated and observed to affect the bone and cartilage morphogenesis and formation. Also, BMPs have been implicated in the development of tissue as diverse as skin, eye, heart, and kidney. These morphogens have the potential to assist in the engineering of bone tissue.
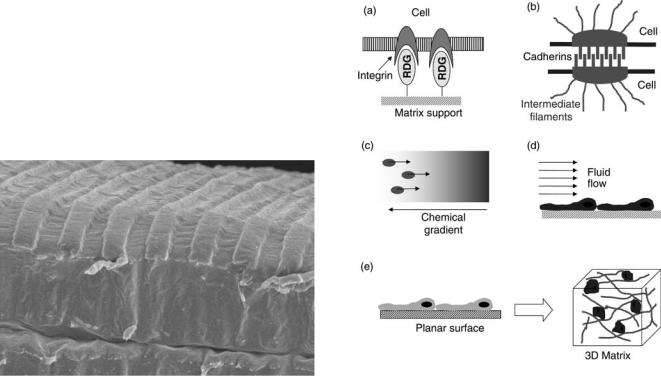
Adhesion. Tissue is held together by the adhesion processes between different cells and the cells and extracellular matrix. The cell–cell interactions consist of tight, anchoring, and communication junctions. Tight junctions are composed of transmembrane proteins that form connections between cells. More contact points will decrease the permeability between the cells so that the tissue can become essentially impermeable. This is typically found with epithelial cells, as in the intestinal, reproductive, and respiratory tract, where the barrier that is formed is essential to function.
Anchoring junctions are loosely held connections that take advantage of the cytoskeleton. With adherens junctions, actin filaments of the cytoskeleton are connected and linked to integrins on the cell exterior. These integrins form focal contacts that interact with cadherins found on the surface of other cells. The focal contacts can also interact with extracellular domains. With the involvement of the cytoskeleton, these junctions can also affect cell function by providing a mechanism to signal changes in cell growth, survival, morphology, migration, and differentiation.
Desmosomes are similar to adherens junctions, but they involve intermediate filament protein, such as vimentin, desmin, and keratin. These junctions connect with other cells via cadherins. A similar junction called the hemidesmosome behaves in the same manner, but connects with basal lamina proteins via integrin.
Communication junctions are those that provide direct communication between cells. These are large proteins that form pore structure that connects the two cells. These large pores (connexons) allow the transport of molecules between cells. These junctions are commonly found between neurons for rapid signal conduction.
In order to connect with other cells or the extracellular matrix, the junction proteins must interact with some receptor molecule. Integrins will bind with the amino acid sequence arginine-glycine-aspartic acid (RGD). This sequence is found in several proteins, such as collagen and fibronectin and these peptides can be incorporated onto other surfaces in order to improve cell adhesion. Cadherin– cadherin binding is mediated via Ca2þ. Without the presence of Ca2þ, the connection is subject to proteolysis. The Ig-like receptors contain motifs found in immunoglobulins. These receptors can interact with neural cell adhesion molecule (N-CAM) and are present during development. Finally, selectins are specific receptor types that are expressed during the inflammatory response. The lectin domain found in oligosaccharides on neutrophils allows
ENGINEERED TISSUE |
191 |
these cells to interact with endothelial cells along the surface of blood vessels.
Migration. During embryogenesis, diffusible factors and ECM composition are important factors in the pattern formation of tissue development. The migration of cells is necessary for the formation of tissue not just for development, but also during regeneration. Cell migration is also observed in other body functions. Angiogenesis, or blood vessel formation, involves the migration of endothelial cells into new tissues. For immune responses, B and T cells patrol the body ready to attack invaders. Tumor invasion and, more importantly, metastasis relies on the migration of cancer cells into other parts of the body. Controlling migration can help to control the spread of cancer.
Signals from various factors can lead to the release of cells from their contact with other cells or with the extracellular matrix. Once released, different mechanisms can affect the migration pattern of the cell depending on the cell type. Cells may move in random directions. The movement can be modeled by Brownian motion. In this case, motion is due to collisions with other particles. This motion is characterized by the time between collisions, the mean free path (average distance before hitting another particle) and the average speed. The characteristics are dependent on the density of the particles.
Of more relevance is the issue of directed migration. Direct migration depends on some sort of gradient. In response to some kind of stimulus, cells may move toward or away from the source of the stimulus. The stimulus may affect speed, direction, or both. Chemotaxis is the general term describing the response of cells to a chemical gradient. The strength of the effect is dependent on the absolute concentration as well as the steepness of the gradient.
Growth. Mitosis is a tightly controlled process to regulate cell growth and depends on signals from the cell’s environment. During mitosis, the deoxyribonucleic acid (DNA) is replicated and copies are separated as the cells divide into two exact copies. This process repeats itself depending on the extracellular signaling and the properties of the cell itself. Certain cells, such as pancreatic beta cells, are locked in the cell cycle and mitosis is arrested. In order to overcome this barrier, stem cells can be used to generate new differentiated cells. Also, cells may be converted into a precursor cell form that can undergo proliferation before switching back to the differentiated form.
Cell growth relies on the availability of essential nutrients. As the need for nutrients increases during cells proliferation, the availability becomes reduced barring some mechanism for distributing the nutrients to the growing tissue. Distribution of nutrients occurs naturally in the human body in the form of the network of blood vessels. The lack of such a vasculature for engineered tissue limits the effective size that tissue can grow.
Vascularization. For most engineered tissue to become integrated into the human body, it must become vascularized by the body’s own blood vessel network. The body provides a natural mechanism for neovascularization by the process of wound healing. When tissue has been
192 ENGINEERED TISSUE
damaged, a cascade of events is initiated to block the bleeding wound and encourage healing. Platelets, fibrin, and fibronectin first form a mesh plug. Mast cells release chemotactic agents to recruit other cells as part of the inflammatory response. Keratinocytes migrate to the site of the injury and begin to proliferate. Vascular endothelial growth factor (VEGF) and fibroblast growth factor (FGF) are released to encourage blood vessel formation. Once the new tissue has been vascularized, remodeling of the tissue occurs to complete the healing process.
For engineered tissue, two options are used to ensure vascularization and promote tissue growth and integration. The engineered tissue can be designed to contain a vascular network in vitro that would then be connected to the body’s own network when it is implanted. This presents a significant engineering challenge in trying to create several different types of engineered tissue in one construct simultaneously. An alternative method is to engineer the tissue to recruit blood vessels from the body’s existing framework. This has been accomplished though the controlled release of VEGF from the biodegradable support matrix of the engineered tissue (8).
Innervation. To become fully integrated into the body, certain tissues and organs must also reconnect with the body’s own nervous system. Several organs of the body form connections with the sympathetic nervous system. These connections are important to regulation of the organ. Skeletal muscle tissue makes sensory and motor connections via the peripheral nervous system. In any case, the cells of these engineered tissues need to make synaptic connection with the axons of the relevant neurons. Because the new tissue is being engineered to replace that which has been lost to injury or disease, the neural framework may not be available for integration. If it is present, the neurons may be encouraged to regenerate toward the tissue and form new connections. Another complex, but theoretically possible, option may be to engineer the tissue with neural connections that can be later integrated into the existing nervous system. Also, artificial devices may be integrated into the system to provide the appropriate control of the tissue function.
Immune Concerns. As with organ transplants, engineered tissue also has concerns of rejection by the immune system. The major histocompatibility complex I (MHC I) present on the cells of the engineered tissue are recognized by the T cells of the immune system as a foreign body. This would eventually lead to cell lysis. The primary means of preventing rejection, though, is the use of immune suppressant drug therapy. While this may be acceptable, for a patient receiving a life saving organ transplant, it is not for those receiving engineered tissue. Certain tissues, such as cartilage, may not interact with the immune system. Metabolic tissues that only interact chemically can be physically separated from the environment. Some engineered tissues may contain cells that are only temporary until the body’s own cells can take over. In these cases, immune suppressant drug may be a viable option. For most other tissues, methods are being developed for side stepping the immune system.
Because the cells of the immune system are formed within the bone marrow, one method is to transplant the bone marrow from the cell and tissue donor along with the organ. The donated bone marrow can form a chimera with the patient’s existing bone marrow to allow the adaptation of the immune system to the new tissue (9).
At the molecular level, the antigen of the foreign cell can be blocked or completely eliminated. In order to block the antigen, a fragment of antibody to the antigen can be added to the tissue to mask the foreign cells from the patient’s own immune system (10). This effect is temporary as the fragments will eventually separate from the antigen. Another drawback is that is may not counter all the mechanisms of immune response. The antigen can also be removed by placing an inactive form of the antigen gene into the cells (11). A gene can also be added to the cells to produce a protein that will inhibit rejection (12). Finally, oligonucleotides can be added to hybridize with either ribonucleic acid (RNA) or DNA in order to inhibit the transcription or translation of the antigen molecule (13).
Microencapsulation is a means of physically separating the cells from the environment. For this method, cells are surrounded by a porous synthetic material. As long as the membrane coating remains intact, the cells are isolated from the immune system. The pore size can be adjusted to allow chemical interaction with the environment while preventing cellular interaction. The encapsulation should allow nutrients to permeate through the membrane and reach the cells. This was first used in clinical studies for the encapsulation of xenogenic pancreatic islets (14).
Cell Types. While the response of the immune system is of great importance to the success of the engineered implant, the source of cells and their application will determine the best method for immunomodulation. Cells may come from the patients themselves (autologous), from a human donor (allogeneic), or from another species (xenogeneic). Each type has its own advantages and disadvantages.
Autologous cells are derived from the patient, expanded in culture, and then placed back into the patient. These cells are completely biocompatible with the patient and this eliminates the need for any immune modulation. Genzyme, for example, has developed a successful protocol for the repairing articular cartilage. One drawback to using autologous cells is that it requires a period of time to expand the cells. This would not be acceptable for patients needing an immediate tissue replacement. As a result, the engineered tissue does not have off-the-shelf availability. Depending on the tissue and the amount of damage, the amount of cells that may be harvested from the patient may be insufficient to form tissue.
Allogeneic cells can help to overcome some of the drawbacks to autologous cells because the cells come from donor sources that may be pooled together. This can provide off-the-shelf availability, but at the expense of immune rejection. The cells can be engineered to become immune acceptable or immunosuppressive drug therapy may be used. These cells are also well suited for tissues that do not interact with the patient’s vasculature system or may only be used until the native tissue regenerate.
Advanced Tissue Science developed a skin replacement tissue (Dermagraft) with cells derived from circumcision surgeries.
Xenogeneic cells are derived from nonhuman species. An animal source can provide an unlimited amount of cells, but they provoke an acute immune response within minutes of implantation into the body. One useful application of such cells is the encapsulation of pancreatic islets (14,15). The membrane can be adjusted to allow the islets to regulate blood sugar and insulin levels while protecting the cells from the immune system. Another drawback to xenogeneic cells is the threat of transmission of animal viruses and well as endogenous retroviruses that may interact with the patient.
Cells that have been isolated may be modified to alter their characteristics before being incorporated into engineered tissue. Primary cells that are subcultured eventually become cell lines. These cell lines may be finite or continuous. The cells may also be normal or transformed compared to the primary cell from which it is derived. Transformation is associated with genetic instabilities that may lead to a change in the phenotype. These changes may impart different growth characteristics for the cell, such as immortalization, anchorage independence, and overall growth rate. The genetic material may be altered to effect gene expression. Changes in protein expression may effect the secretion of chemical factors or even the formation of extracellular matrix. In the worst case, cells may become cancerous and prove to be detrimental to the patient. Examples of stable, well-characterized cell lines used in tissue engineering include HEK-293 for nerve growth factor secretion (16), and 3T3-L1 for adipose tissue formation (17).
Primary cells as well as cell lines can be artificially transformed by introducing new genes by the process of transfection. In this process, a new gene is carried by some vector, such as a liposome or virus, to the host cells. The gene is transferred into the cells and delivered into the nucleus where it can be transcribed. This method allows the creation of cells with desirable characteristics for engineered tissue. Such cells may secrete growth factor that will enhance tissue formation. Examples of engineered tissue utilizing transfected cells include insertion of hBMP-4 gene in bone marrow stromal cells for bone tissue engineering (18) and aquaporin gene transfection in the LLC-PK1 cell line for a bioartificial renal device (19), secretion of neuronal growth factors from fibroblasts to enhance axonal regeneration (20).
Regardless of the source, primary cells have limitations depending on their age and genetic makeup. Adult cells may only have a limited number of cell divisions before they reach senescence or even become cancerous. Transformed cell lines may allow for continuous growth, but without proper control can become a problem for the patient. These cells are typically used to enhance regeneration of existing tissue, but do not become integrated into the body. Because of these issues, a universal cell that can develop into multiple tissue types has an infinite capacity to proliferate without loss of function, and if immune acceptable would be ideal for engineered tissue. Stem cells come closest to meeting these criteria.
ENGINEERED TISSUE |
193 |
Fertilized
Egg
Totipotent
Blastocyst |
|
|
|||
|
|
|
|
|
|
Amniotic |
Inner Cell |
|
Embryonic |
|
|
Sac |
|
Mass |
|
Stem Cells |
|
|
|
|
|
All Cell |
|
|
|
|
|
|
|
|
|
|
|
|
Types |
|
|
Fetus |
|
Embryonic |
|
|
|
|
Germ Cells |
|
|
|
|
|
|
Pluripotent |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Hematopoietic |
Blood |
|
|
|
Adult |
Stem Cells |
Cells |
|
Spermatocyte |
|
Neural |
Neurons |
||
|
Stem Cells |
||||
Stem Cell |
|
|
Astrocytes |
||
|
|
|
|
||
|
|
|
|
|
Oligodendrocytes |
|
|
Mesenchymal |
|
||
Sperm |
|
Stem Cells |
Bone |
|
|
|
|
|
Cartilage |
||
Unipotent |
|
|
|
||
|
|
|
Muscle |
||
|
|
Multipotent |
Tendon |
||
|
|
|
|
Fat |
|
Figure 2. Stem cell potency. Relationship of stem cells to various stages of development. Cells and tissue derived from stem cells are shown in italics.
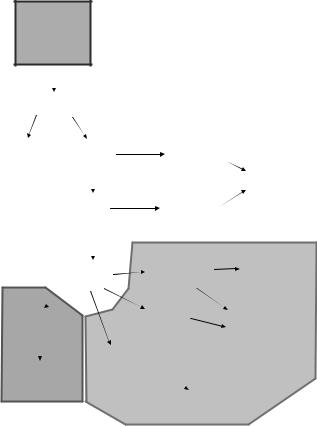
Stem Cells. The potency of stem cells is defined by their ability to differentiate into one or more cell genotypes (see Fig. 2). Unipotent stem cells give rise to only one cell type (ex. Spermatogonia). Multipotent stem cells are more functional and can differentiate into multiple cell types. Embryonic stem cells are considered pluripotent in that they can form all the cell types found in an embryo and adult. The fertilized egg develops into an embryo as well as the amniotic sac and is considered totipotent. Embryonic stem cells hold the most promise for engineering tissue, but more work must be done on the basic principles of stem and progenitor cell biology as well as on the control of differentiation.
Multipotent stem cells obtained from embryonic or adult sources are considered the optimal choice for tissue engineering applications because of their ability to form multiple tissue type. Hematopoietic stem cells (HSCs) are the most well characterized of stem cells. While isolated from bone marrow, HSCs can differentiate to form skeletal muscle, cardiac muscle, hepatocytes, endothelial cells, and epithelial cells. Multipotent stem cells can be found in several other tissues, such as brain, heart, pancreas, retina, liver, and lung, and skin.
To take full advantage of the functionality of stem cells, more work needs to be done to elucidate the mechanisms for differentiation. Once established, stem cells can be encouraged to differentiate into the required cell type.
194 ENGINEERED TISSUE
The mechanism may rely on an environmental cue as to whether they are physical contact, chemical, or chemotactic in nature. The ability of stem cell to proliferate, integrate, and differentiate also depends on the methods of identifying, isolating, and expanding. Protocols for stem cell culture need to be developed and optimized to ensure the cells achieve their full potential.
Since some stem cells are harder to obtain than others, getting stem cells to transdifferentiate from one form to another would allow for further flexibility. Evidence suggests that bone marrow stromal cells may convert to neural stem cells (21) and neural stem cells to hematopoietic stem cells (22). Recent evidence, though, points to the fusion of stem cells with other cells instead of true transdifferentiation (23).
Another source for stem cells is from embryos discarded from in vitro fertilization clinics. Human embryonic stem cells have an even greater capacity to form tissues than the multipotent stem cells. These cells have been isolated from humans and protocols for long-term cultures have successfully been developed (24). The use of embryonic stem cells has raised many ethical concerns because of the destruction of the fetus from which they are derived. This has led to legislation tightly regulating their use. To avoid these concerns, several proposals have been suggested to obtain embryonic stem cells without compromising the potential for life (25).
Stem cells have been used successfully for tissue engineering applications. Stem cells have been seeded on scaffolds to form cartilage, small intestine, and bone (26). Neural stem cells have also been used for repair of spinal cord injuries (27). Embryonic stem cells have also been seeded onto scaffolds where the native vasculature integrated into the engineered tissue (28).
Instead of preseeding cells on scaffolds, stems cells may also be injected directly to the site of injury to promote tissue regeneration. Clinical studies in nonhuman primates have shown that neural stem cells can enhance repair of spinal cord injuries (29). Stem cells have also been used to regenerate damaged cardiac muscle tissue (30). Embryonic stem cells may also be used to regenerate pancreatic beta cells in order to alleviate diabetes (31). Mesanchymal stem cells also show some promise for the repair of articular cartilage for those suffering from osteoarthritis (32).
Scaffolds
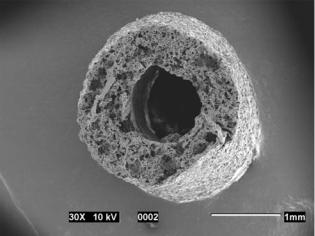
Primary cells will form monolayer cultures when dissociated from tissue. In order to encourage the cells to form engineered tissue, they must be placed in a 3D matrix that acts as a support scaffold. Ideally, these scaffolds should be compatible with the cells as well as being biodegrade. The scaffold should have a high porosity to ensure the diffusion of nutrients and other chemical factors as well as provide room for cell migration and proliferation. The material should have a higher surface area to ensure adequate room for cell attachment. The matrix should maintain its structural integrity until tissue integration has been completed. For certain applications, the final construct may need to be formed into a specific 3D shape (see Fig. 3).
Figure 3. Example of a scaffold for engineered tissue. This scaffold is designed for nerve regeneration. The cylindrical conduit was manufactured by using the solvent casting method (see below) with particle leaching. Poly(vinyl alcohol) rods were coated with a suspension of salt crystals in a poly(lactic acid) (PLA)–chloroform solution. Dissolution of the rods permitted the formation of the large central pore through which nerve tissue could regenerate. A porosity of 85% was obtained by controlling the volume fraction of salt crystals.
For tissue engineering, scaffolds may come in different forms. An acellular matrix can be used to recruit cells from the host tissue (33). With this form, the immune response is not a concern though inflammation may occur. For most applications, cells must be seeded onto the scaffold to ensure successful tissue formation. Cells can be seeded onto collagen gels that mimic the naturally occurring extracellular matrix (34,35). Cells can also be encouraged to self-assemble in culture. These systems are ideal for tissue that forms simple shapes, such as sheets and cylinders (36,37). Biodegradable polymers provide a flexible means of creating scaffolds with properties desirable for tissue formation.
Natural Polymers. Macromolecules found with the extracellular matrix provide chemical and structural support for living tissue. Because of their function in tissue formation, these natural polymers provide an excellent scaffold for engineering new tissue. These natural polymers have some limitations in their application. The mechanical properties and degradation rates cannot be controlled as well as synthetic polymers (38). Also, material derived from donors may elicit an immune response (39). Many of these limitations can be overcome by chemical modification of the materials as well as creating composite materials of natural polymers or natural–synthetic polymers.
Collagen is a large family of proteins that make up much of the extracellular matrix. At least 19 different types have been isolated. Fibrillar collagen is comprised of several collagen types that combine to form extended structures that assist is maintaining tissue integrity. The relative amounts of collagen are characteristic of the tissue type. Collagen has been used for cartilage (40), nerve regeneration (41), gallbladder engineering (42), corneal tissue (43),