




|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
LARYNGEAL PROSTHETIC DEVICES |
233 |
|
|
The tracheostoma breathing valve contains an elastic |
|
|
|
|||||||||||||||||||
diaphragm installed in a peristomal housing, which permits |
|
|
|
||||||||||||||||||||
normal respiration during silent periods. Expiratory air for |
|
|
|
||||||||||||||||||||
speech shuts off the pressure-sensitive diaphragm, and is thus |
|
|
|
||||||||||||||||||||
diverted through the valve into the esophagus. This device |
|
|
|
||||||||||||||||||||
eliminates the need for manual stoma occlusion during speech. |
|
|
|
||||||||||||||||||||
|
In both cases, air from the lung reaches the esophagus |
Figure 13. Examples of fixed commercial prosthesis. (Staffieri, |
|||||||||||||||||||||
and causes the mucosal tissue tovibrate. The resulting |
|||||||||||||||||||||||
Groningen standard, Groningen low pressure, Panje, Provox). |
|||||||||||||||||||||||
sound can be modulated by the mouth, teeth, oral cavity, |
|||||||||||||||||||||||
|
|
|
|||||||||||||||||||||
and so on, to produce the new voice. |
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
Most speakers that have prosthesis do not have difficul- |
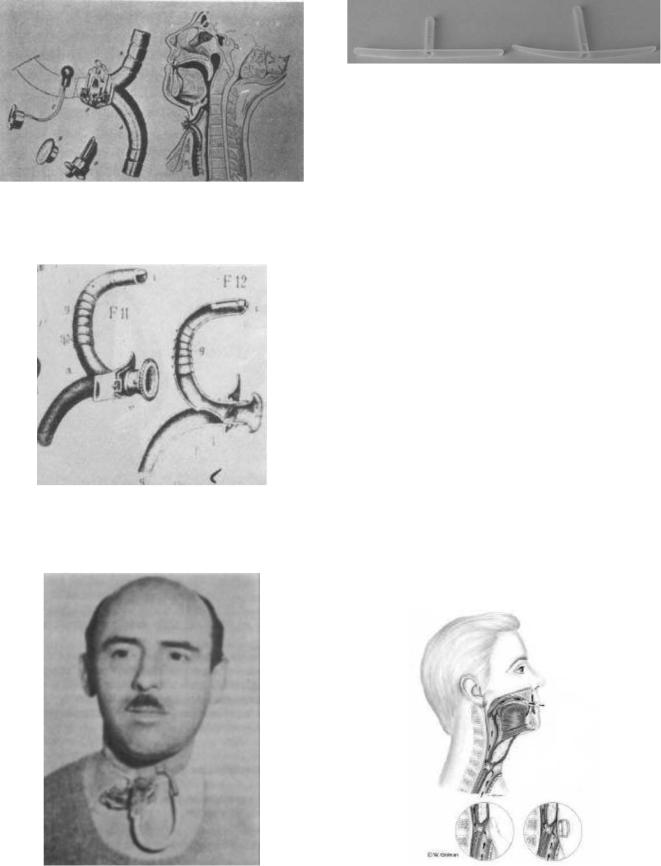
tracheal retention collar is connected to the mucosa (or |
|||||||||||||||||||||
ties with articulation, rate of speech, or phonatory duration. |
tracheal flange), a hollow cylindrical tube (whose length |
||||||||||||||||||||||
|
If esophageal speech depends on gulping or trapping air |
depends on the patient’s physical characteristics) connect- |
|||||||||||||||||||||
using the phonatory valve, the resulting speech depends on |
ing the trachea to the esophagus, an endoesophageal |
||||||||||||||||||||||
expiratory capacity. Voice quality is very good, and may |
flange, and a dome (or hat) that closes the proximal endoe- |
||||||||||||||||||||||
resemble the ‘‘original’’ voice. |
|
|
|
|
|
|
|
|
sophageal end of the tube. Via the razor-thin slit (or |
||||||||||||||
|
Poor digital occlusion of the tracheostoma as well as |
esophagus exit), the hat enables airflow to pass from the |
|||||||||||||||||||||
poor tracheostoma valve adherence allows pulmonary air |
trachea to the esophagus when there is a positive differ- |
||||||||||||||||||||||
to escape from the stoma prior to its diversion through the |
ential pressure, and prevents the reverse flow of liquid (or |
||||||||||||||||||||||
prosthesis into the oesophagus for voice production. In fact, |
food) when the differential pressure becomes negative. The |
||||||||||||||||||||||
the bleeding off of pulmonary air limits phonatory duration |
arrows represent the airflow paths. |
|
|||||||||||||||||||||
and, therefore, the number of words that can be spoken. |
|
Hat shape and the extension of the razor-thin slit can |
|||||||||||||||||||||
|
The one-way valve design of the prosthesis prevents |
differ according to valve type. The razor-thin slit may be |
|||||||||||||||||||||
aspiration (of food and liquid) from the esophagus to the |
located at the base of the hat (Staffieri, Groningen low |
||||||||||||||||||||||
trachea. An example of a phonatory valve is shown in |
pressure), at the center of the hat (Panje, Groningen |
||||||||||||||||||||||
Fig. 12 (11,12). The prosthesis illustrated in this sketch |
standard), or inside the hollow tube (Provox, Blom-Singer). |
||||||||||||||||||||||
consists of an air-flow tracheal entry, whereby an endo- |
|
Though valve geometry and shape may vary, the oper- |
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ating principle remains the same. |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Several commercial prostheses are shown in Fig. 13: |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
from left to right, they include the Staffieri, Groningen |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
standard, Groningen low pressure, Panje, and Provox types. |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Fixed and removable prostheses are available in differ- |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ent lengths, which usually range from 6 to 12 mm to enable |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
the surgeon to select the dimensions that are best suited to |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
the patient’s physical characteristics, for example, poster- |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ior tracheoesophageal wall thickness. |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
To compare valve performance in the laboratory, most |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
authors use valve airflow resistance (7,11), which is defined |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
as the ratio of pressure to flow-rate. Figure 14 show an |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
example of resistance versus flow-rate characteristics |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
obtained with experimental tests on commercial valves (11). |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Low resistance allows air to pass freely though the |
||
|
Figure 12. Sketch of phonatory valve or prostheses. |
prosthesis with little effort on the part of the patient, and |
|||||||||||||||||||||
|
80 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Staffieri |
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
/s)] |
70 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Provox |
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
60 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
3 |
40 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
pressure |
|
|
|
|||
[kPa/(dm |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
50 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Groningen |
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
standard |
|
|
|
||||
Resistance |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Groningen low |
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
30 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Panje |
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
20 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
10 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
0 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
0 |
0,05 |
0,1 |
0,15 |
0,2 |
0,25 |
0,3 |
0,35 |
|
||||||||||||||
|
|
|
|
|
|
|
|
|
Flow-rate [dm3/s (ANR)] |
|
|
|
|
|
|
Figure 14. Resistance of commercial valves. |
|
||||||