

новая папка / [libribook.com] 50 Cases in Clinical Cardiology_ A Problem Solving Approach 1st Edition
.Pdf
Acknowledgments
I am extremely grateful to:
•Myteachersinschool,whohelpedmetoacquiregoodcommandoverspoken and written English language.
•My lecturers and professors in medical college, who taught me the science and art of bedside cardiology.
•My heart patients, whose findings on clinical examination and results of investigations made me wiser.
•Learned authors of textbooks on clinical cardiology to which I referred liberally, while preparing the manuscript.
•My esteemed readers of earlier books, whose generous appreciation and constructive criticism keep me going.
•M/s Jaypee Brothers Medical Publishers (P) Ltd., New Delhi, India, who repose their unflinching faith in me and provide excellent editorial support.

Contents
Section 1: Congenital Heart Diseases
Case 1 |
: |
Ventricular Septal Defect |
3 |
Case 2 |
: |
Atrial Septal Defect |
7 |
Case 3 |
: |
Fallot’s Tetralogy |
11 |
Case 4 |
: |
Ebstein’s Anomaly |
15 |
Case 5 |
: |
Patent Ductus Arteriosus |
19 |
Section 2: Mitral Valve Diseases
Case 6 |
: |
Mitral Stenosis |
25 |
Case 7 |
: |
Mitral Regurgitation |
29 |
Case 8 |
: |
Mitral Valve Prolapse |
33 |
Section 3: Aortic Valve Diseases
Case 9 |
: |
Aortic Stenosis |
39 |
Case 10 |
: |
Aortic Regurgitation |
43 |
Case 11 |
: |
Aortic Sclerosis |
48 |
Section 4: The Cardiomyopathies
Case 12 |
: |
Dilated Cardiomyopathy |
55 |
Case 13 |
: |
Restrictive Cardiomyopathy |
59 |
Case 14 |
: |
Hypertrophic Cardiomyopathy |
63 |
Case 15 |
: |
Takotsubo Cardiomyopathy |
67 |
Section 5: Aortic Diseases
Case 16 |
: |
Aneurysm of Aorta |
73 |
Case 17 |
: |
Dissection of Aorta |
77 |
Case 18 |
: |
Coarctation of Aorta |
81 |
Case 19 |
: |
Sinus of Valsalva Aneurysm |
85 |
xiv |
|
50 Cases in Clinical Cardiology: A Problem Solving Approach |
|
|
|
Section 6: Pulmonary Diseases
Case 20 |
: |
Pulmonary Stenosis |
91 |
Case 21 |
: |
Pulmonary Hypertension |
95 |
Case 22 |
: |
Pulmonary Embolism |
99 |
Case 23 |
: |
Obstructive Pulmonary Disease |
103 |
Section 7: Pericardial Infections
Case 24 |
: |
Acute Pericarditis |
109 |
Case 25 |
: |
Pericardial Effusion |
113 |
Case 26 |
: |
Constrictive Pericarditis |
117 |
Section 8: Myocardial Infections
Case 27 |
: |
Rheumatic Fever |
123 |
Case 28 |
: |
Acute Myocarditis |
127 |
Section 9: Endocardial Infections
Case 29 |
: |
Aortic Valve Endocarditis |
133 |
Case 30 |
: |
Tricuspid Valve Endocarditis |
137 |
Section 10: Intracardiac Masses
Case 31 |
: |
Atrial Myxoma |
143 |
Case 32 |
: |
Atrial Thrombus |
147 |
Case 33 |
: |
Ventricular Thrombus |
151 |
Section 11: Typical ECG Abnormalities
Case 34 |
: |
Left Ventricular Hypertrophy |
157 |
Case 35 |
: Left Bundle Branch Block |
161 |
|
Case 36 |
: |
Features of Hypokalemia |
165 |
Case 37 |
: |
Features of Hyperkalemia |
169 |
Section 12: Electrocardiac Syndromes
Case 38 |
: |
Prolonged Q-T Syndrome |
175 |
Case 39 |
: |
Sick Sinus Syndrome |
179 |
Case 40 |
: |
Early Repolarization Syndrome |
183 |
Case 41 |
: |
Brugada Syndrome |
186 |
Case 42 |
: |
WPW Syndrome |
189 |

Contents |
|
xv |
|
|
|
Section 13: Cardiac Arrhythmias
Case 43 |
: |
Supraventricular Tachycardia |
195 |
Case 44 |
: |
Atrial Fibrillation |
199 |
Case 45 |
: |
Ventricular Premature Beats |
203 |
Case 46 |
: |
Ventricular Tachycardia |
207 |
Section 14: Coronary Artery Diseases
Case 47 |
: |
Chronic Stable Angina |
213 |
Case 48 |
: |
Acute Coronary Syndrome |
217 |
Case 49 |
: |
Papillary Muscle Rupture |
222 |
Case 50 |
: |
Left Ventricular Aneurysm |
226 |
Index |
|
|
231 |
S E C T I O N
1
Congenital Heart
Diseases

|
|
C A S E |
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
||
|
|
1 |
|
Ventricular |
|
|
|
|
|
|
|
|
|
|
|
|
|
Septal Defect |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Case Presentation
A 31-year old man was referred to the cardiologist by a general physician, for evaluation of a heart murmur. This young man had been denied a life insurance policy because the physician, empanelled by the insurance company, had incidentally noticed the murmur during medical examination. The man was normally very active and denied complaints of chest pain, breathlessness, palpitations or syncope. There was no history of cyanotic spells, joint pains or repeated chest infections during childhood and he regularly played cricket and football in school. However, the patient recollected that the doctor in the school medical room had noticed the murmur and made a note of it in his medical report.
On examination, the man was of average built and height and looked healthy. The pulse was 84 beats/min. and regular with no special character. The BP was 134/76 mm Hg in the right arm while sitting. There was no anemia, cyanosis or clinical sign of congestive heart failure. The apex beat was ill-sustained, heaving in nature and slightly displaced towards the axilla. There was a pansystolic murmur over the middle of the left sternal border with a S3 sound in early diastole. The murmur did not radiate towards the axilla. There was no parasternal heave and the lower border of the liver was not palpable. The lung fields were clear.
CLINICAL DISCUSSION
From the history and physical examination, this asymptomatic young man had a parasternal pansystolic murmur. Typical causes of a pansystolic murmur are mitral regurgitation, ventricular septal defect and tricuspid regurgitation. Sometimes, tight coarctation of aorta or a patent ductus arteriosus with pulmonary hypertension can also produce a pansystolic murmur but these murmurs are usually located at the upper left sternal edge. The murmur of mitral regurgitation radiates towards the axilla while the murmur of tricuspid regurgitation is usually associated with engorged neck veins and an enlarged pulsatile liver.
ECG of the patient showed biphasic RS complexes in the mid-precordial leads. X-ray chest showed mild cardiomegaly with minimal signs of pulmonary congestion. On ECHO, the left ventricle was normal in size with normal ejection fraction. A signal drop-out was noticed in the mid-portion of the interventricular
4 |
|
Section 1 Congenital Heart Diseases |
|
|
|
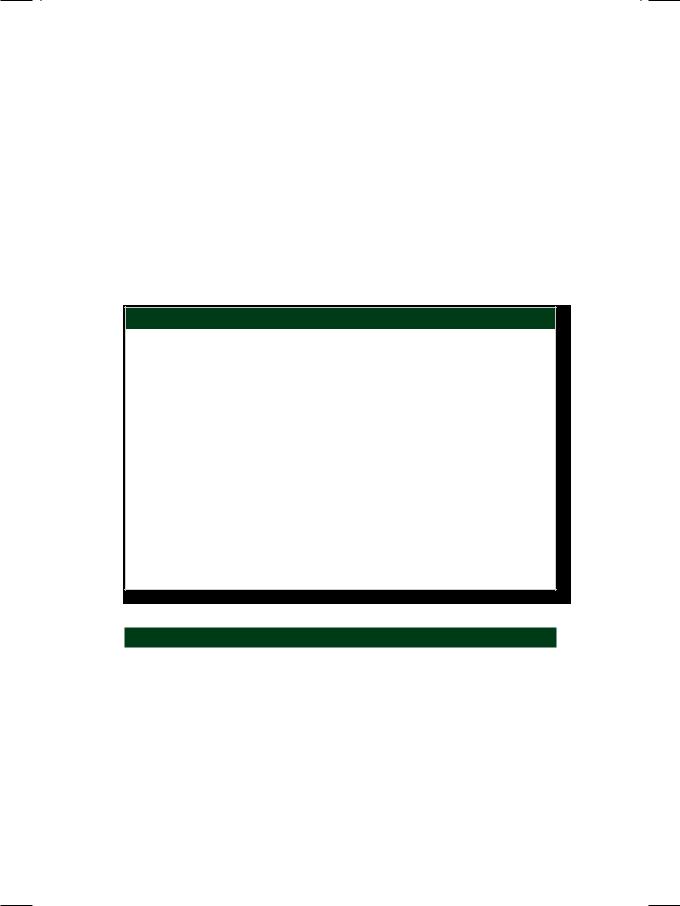
Figure 1.1: Color flow map extending from left ventricle to right ventricle
septum. There was no abnormality of the cardiac valves and the estimated pulmonary artery pressure was normal. On color Doppler, an abnormal flow map was observed extending from the left ventricle to the right ventricle (Fig. 1.1), with a high velocity jet on continuous wave Doppler. Therefore, the definite diagnosis in this case is ventricular septal defect (VSD).
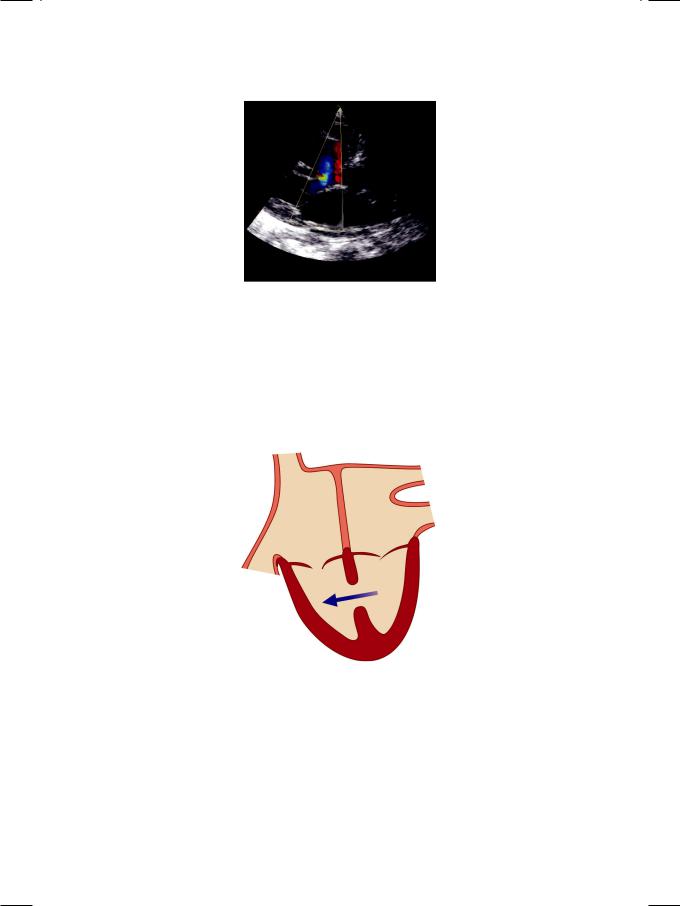
Figure 1.2: Ventricular septal defect
In VSD, a breach in the continuity of the interventricular septum creates a left-to-right shunt between the ventricles (Fig. 1.2). This congenital cardiac defect occurs due to complexity of embryological development of the septum, which has a membranous and a muscular portion. Most (80%) VSDs occur at the junction of these sections and are termed as perimembranous VSD (Fig. 1.3). Some VSDs occur in the muscular section (muscular VSD) and may be multiple (sieve-like). Rare varieties of VSD are endocardial cushion defects (supracristal VSD) and outlet septal defect (subpulmonic VSD) (Table 1.1).