

новая папка / [libribook.com] 50 Cases in Clinical Cardiology_ A Problem Solving Approach 1st Edition
.Pdf
|
|
C A S E |
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
||
|
|
36 |
Features of |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Hypokalemia |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CASE PRESENTATION
A 48-year old man sought consultation from a physician for pain and weakness in both arms, since the last 3 days. There was no history of chest pain, breathlessness, palpitation or sweating. The heaviness in the arms was aggravated by lifting a light weight, but not by movement at the neck.The patient also complained of fatigue and pain over his calf muscles while walking. He had systemic hypertension for several years for which he was presently prescribed losartan 50 mg and hydrochlorthiazide 25 mg. The patient also suffered from bronchial asthma, for which he used an inhaler containing a combination of salmeterol and fluticasone. Recently, he had a gastro-intestinal infection with profuse vomiting and diarrhea that lasted 2 days. Besides age and hypertension, other cardiovascular risk factors in the patient were prediabetes and a modestly elevated serum cholesterol.
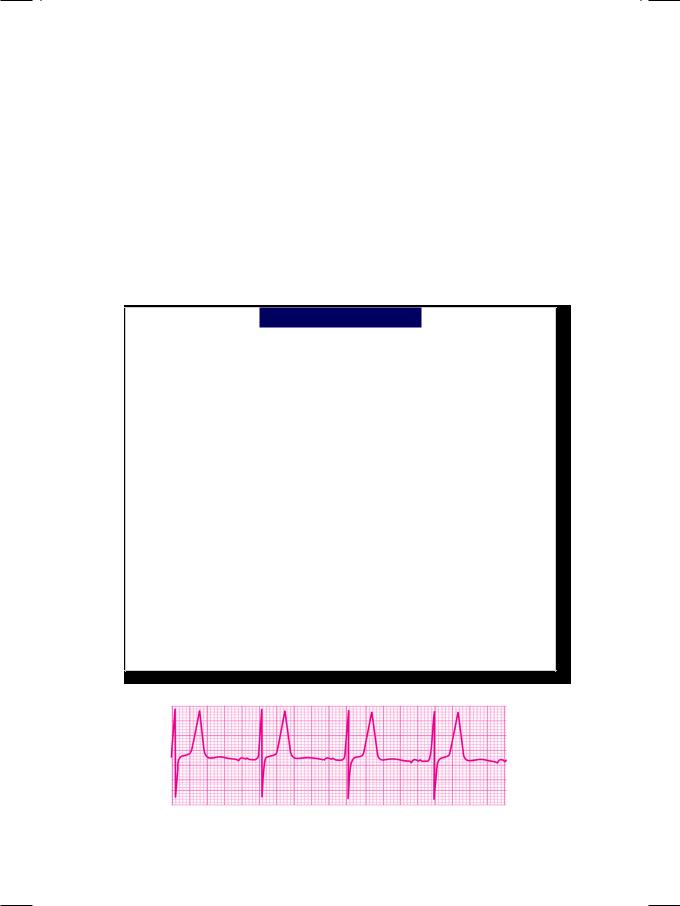
On examination, the patient was coherent, comfortable and in no distress. There was no anemia, cyanosis, icterus or ankle edema. The JVP was not raised, thyroid gland was normal and there were no palpable lymph-nodes. The pulse rate was 72 beats/min with a BP of 130/80 mm Hg. The precordium was unremarkable and the apex beat was normally located. The S1 and S2 were normal and no gallop sound was heard. No murmur or pericardial friction rub was audible. The breath sounds were normal without rhonchi or crepts. An ECG was obtained (Fig. 36.1) following which he was asked to immediately see a cardiologist. His blood biochemistry was Glucose 128 mg/dl, Urea 38 mg/dl, Creatinine 1.2 mg/dl, LDL cholesterol 147 mg/dl, Sodium 131 m Eq/L and Potassium 2.9 m Eq/L.
Figure 36.1: ECG showing flat T waves with prominent U waves
166 |
|
Section 11 Typical ECG Abnormalities |
|
|
|
ECG INTERPRETATION
The ECG showed normal sinus rhythm. The P wave and QRS complex were normal in morphology. There were no significant Q waves and the S-T segment was isoelectric. The T wave was reduced in amplitude, while the U wave was prominent. TheQ-T intervalseemedtobeprolonged.These findingsareconsistent with the diagnosis of hypokalemia. Hypokalemia is an important cause of T wave change. The T wave is either reduced in amplitude, flattened or inverted. This is associated with prominence of the U wave that follows the T wave. The low T wave followed by a prominent U wave produces a ‘camel-hump’ effect.
In hypokalemia, the T wave is flattened and the prominent U wave may be mistaken for the T wave. This may falsely suggest prolongation of the Q-T interval, whereas it is actually the Q-U interval. Hypokalemia therefore causes pseudo-prolongation of the Q-T interval, at the expense of T wave. The U wave that is exaggerated and approximates the size of the T wave is considered to be a prominent U wave. Other causes of prominent U wave are cardiovascular drugs e.g. digitalis, quinidine and psychotropic agents e.g. phenothiazines, tricyclic antidepressants.
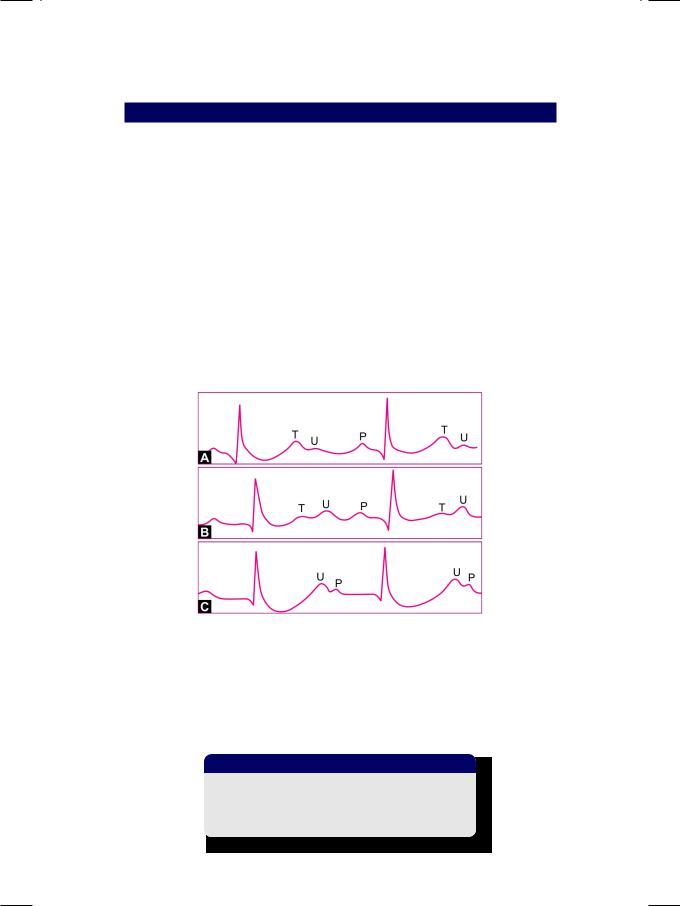
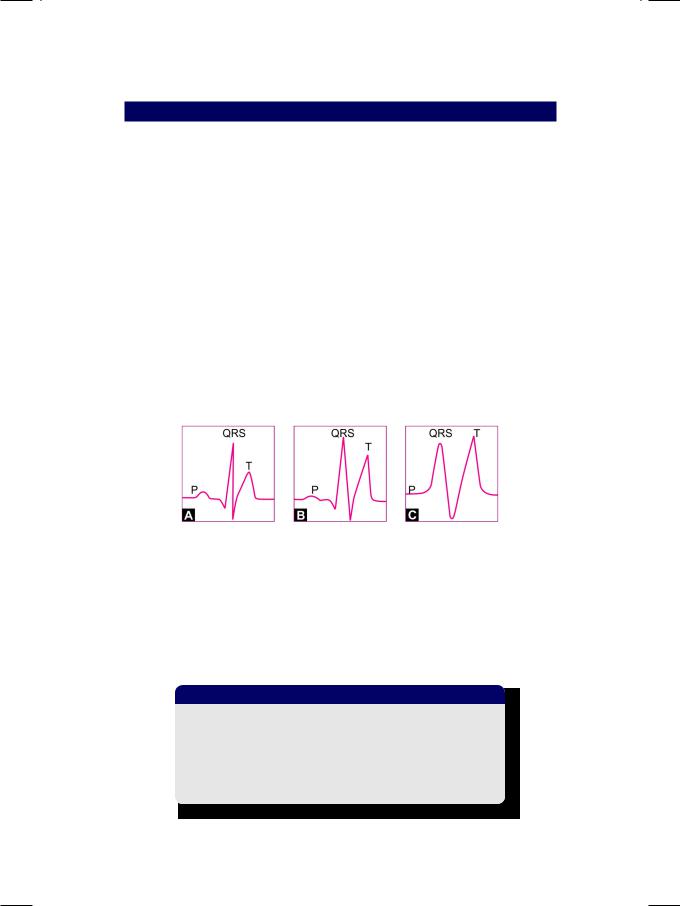
Figure 36.2: ECG features of progressively increasing hypokalemia
The ECG features of hypokalemia depend upon its severity (Fig. 36.2). In mild hypokalemia, only the T wave amplitude is reduced. In moderate hypokalemia, the U wave becomes more prominent than the T wave. In severe hypokalemia, there is sagging of the S-T segment and only the U wave is visible (Table 36.1).
Table 36.1: ECG features of progressive hypokalemia
•Reduced amplitude of the T wave
•Flat T wave with prominent U wave
•S-T segment sagging; only U wave.
Case 36 Features of Hypokalemia |
|
167 |
|
|
|
CLINICAL DISCUSSION
The ECG is sometimes helpful in the diagnosis of an electrolyte abnormality, even before the blood biochemistry results from the laboratory are available. Variation in the blood levels of potassium and calcium are mainly responsible for these ECG changes. Hypokalemia causes pseudo-prolongation of the Q-T interval, at the expense of the T wave. Hypocalcemia causes true prolongation of the Q-T interval, with true lengthening of the S-T segment.
Table 36.2: Causes of hypokalemia
• Body fluid loss
Diuresis
Vomiting
Diarrhea
• Redistribution
Metabolic alkalosis
• Drug -induced
Beta-agonist Insulin therapy
• Hyperaldosteronism
Cushing’s disease Conn’s syndrome
• Genetic causes
Hypokalemic periodic paralysis Renal tubular acidosis Type 2
There are several causes of hypokalemia which have been enlisted in Table 36.2. True loss of potassium is due to vomiting, diarrhea, naso-gastric suction and diuretic therapy (see Table 36.2). Redistribution of potassium occurs in metabolic alkalosis (intracellular shift) and with beta-agonist or insulin therapy. Hypokalemia is a feature of cortisol excess due to Cushing’s disease or steroid therapy as well as a feature of hyperaldosteronism in Conn’s syndrome. Genetic causes of hypokalemia are Type 2 renal tubular acidosis (RTA-2) and hypokalemic periodic paralysis. Typical clinical features of hypokalemia are fatigue and leg cramps. In severe cases, neuromuscular paralysis and cardiac arrhythmias may occur. In cardiac patients on diuretic treatment, hypokalemia aggravates digitalis toxicity and increases the likelihood of serious ventricular arrhythmias.
In our case, the hypokalemia was multi-factorial. Firstly, the patient was prescribed a diuretic for his hypertension. Secondly, he was using an inhaled beta-agonist for asthma, which is known to cause hypokalemia. Finally, he had a recent episode of gastro-enteritis, which might have caused substantial loss of potassium from his body.
168 |
|
Section 11 Typical ECG Abnormalities |
|
|
|
Table 36.3: Management of hypokalemia
• Potassium replacement
Dietary supplements Oral K preparations Intravenous infusion
• Treatment of the cause
Anti-emetics
Anti-diarrheals Diuretic withdrawal
MANAGEMENT ISSUES
Management of hypokalemia includes potassium replacement and correction of the underlying cause (Table 36.3). Potassium can be replaced through dietary supplementation of potassium-rich foods. Oral proprietary supplements of potassium citrate can also be prescribed. If potassium deficiency is severe or if the patient is vomiting, potassium chloride is administered as an intravenous infusion. Generally, potassium deficiency is more severe, if there is true loss of body fluids than if there is only a transcellular shift of potassium.
|
|
C A S E |
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
||
|
|
37 |
Features of |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Hyperkalemia |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
. |
CASE PRESENTATION |
A 64-year old woman was wheeled into the emergency room, with generalized weakness and shortness of breath of one week duration. She also complained of swelling around the eyes and over the feet, loss of appetite and occasional vomiting. The lady was a known case of diabetes mellitus since 25 years and systemic hypertension for the last 12 years. She sustained an anterior wall myocardial infarction four years back, for which she was thrombolysed. At that time, coronary angiography showed triple-vessel disease, but she declined a revascularization procedure. Her serum creatinine value was found to be high and therefore, she was switched over from oral antidiabetic drugs to insulin therapy. The patient also underwent laser photocoagulation for proliferative retinopathy, one year back. She was presently undergoing maintenance hemodialysis, thrice a week.
On examination, the patient was drowsy, disoriented and obviously dyspneic. The complexion was pale and sallow with dry skin that bore marks of pruritus. There was periorbital puffiness and pitting edema over the ankles and lower legs. The neck veins were engorged but there was no cyanosis or icterus. The pulse rate was 92 beats/min. with a BP of 160/94 mm Hg. The precordium was unremarkable and the apex beat was displaced to the left. The S1 was normal with a loud A2 and a S3 sound in early diastole. An ejection murmur was audible along the left sternal border. No pericardial friction rub was audible. There were bilateral basilar rales over the lung fields. An ECG was obtained (Fig. 37.1) following which she was immediately given an injection. Her laboratory reports were Hemoglobin 9.2 g/dL% Urine sugar +1 albumin +2, Glucose 144 mg/dl, Urea 124 mg/dl, Creatinine 5.2 mg/dl, Sodium 129 mEq/L, Potassium 6.8 mEq/L and Calcium 7.4 mg%.
Figure 37.1: ECG showing tall T waves with flat P waves
170 |
|
Section 11 Typical ECG Abnormalities |
|
|
|
ECG INTERPRETATION
The ECG showed normal sinus rhythm. The P wave was flattened and the P-R interval was prolonged. There were no significant Q waves and the S-T segment was isoelectric. The T wave was upright, tall and peaked. The Q-T interval was short. These findings are consistent with the diagnosis of hyperkalemia. A T-wave that exceeds a voltage of 5 mm in the standard leads and 10 mm in the precordial leads is considered tall. Besides hyperkalemia, causes of tall T wave are myocardial ischemia and the hyperacute phase of myocardial infarction. The T wave of hyperkalemia is tall, peaked symmetrical and has a narrow base, the so called ‘tented’ T wave. The Q-T interval is short. On the other hand, the T wave of coronary insufficiency is tall but broad-based and the Q-T interval is prolonged.
The normal Q-T interval is 0.39 + 0.04 sec. and ranges from 0.35 to 0.43 sec. A Q-T interval measuring less than 0.35 sec is considered short. Besides hyperkalemia, causes of short Q-T interval are hypercalcemia and digitalis toxicity. Hyperkalemia shortens the Q-T interval and is associated with tall T waves, wide QRS complexes and diminished P waves. Hypercalcemia also shortens the Q-T interval but there are no changes in the morphology of the QRS deflection. The proximal limb of the T-wave has an abrupt upslope to its peak.
Figure 37.2: ECG features of progressively increasing hyperkalemia
The ECG features of hyperkalemia depend upon its severity (Fig. 37.2). When the serum level exceeds 6.8 mEq/L, tall T waves and short Q-T interval are seen. When it exceeds 8.4 mEq/L, additionally the P wave gets flattened and the P-R interval gets prolonged. At a serum level which is in excess of 9.1 mEq/L, the QRS complex also becomes wide and ventricular arrhythmias occur (Table 37.1).
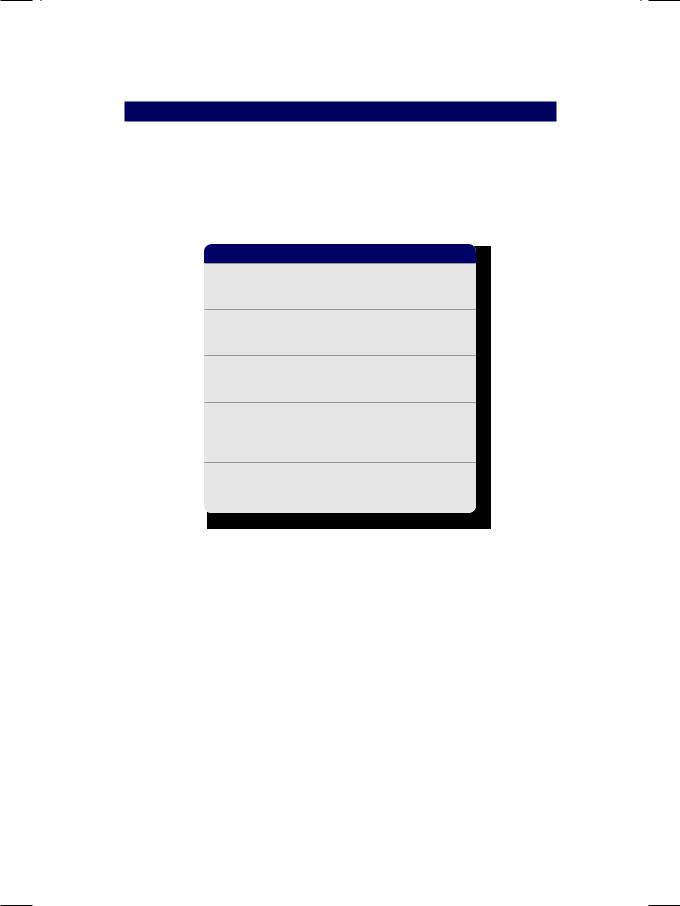
Table 37.1: ECG features of progressive hyperkalemia
A. |
Serum K>6.8 mEq/L |
tall T waves; |
|
|
short Q-T interval |
|
|
|
B. |
Serum K>8.4 mEq/L |
(A) plus flat P waves; |
|
|
prolonged P-R interval |
|
|
|
C. |
Serum K>9.1 mEq/L |
(B) plus wide QRS complex; |
|
|
A-V block and arrhythmias |
|
|
|
Case 37 Features of Hyperkalemia |
|
171 |
|
|
|
CLINICAL DISCUSSION
The electrocardiogram often shows changes due to an electrolyte abnormality. These changes are observed even before the biochemical reports from the laboratory are available. Variation in the blood levels of potassium and calcium are chiefly responsible for these ECG changes. Abnormal levels of calcium and magnesium produce similar changes. Hypercalcemia shortens the Q-T interval while hypocalcemia prolongs it.
Table 37.2: Causes of hyperkalemia
• Potassium gain
Hemolysis, tumour lysis Rhabdomyolysis, burns
• Redistribution
Metabolic acidosis Hyperglycemia
• Hypoaldosteronism
Addison’s disease Acute renal failure
• Drug induced
Potassium sparing diuretics Non-steroidal anti-inflammatory drugs Anti-angiotensin drugs (ACEi & ARBs)
• Genetic Causes
Hyperkalemic periodic paralysis Renal tubular acidosis Type 4.
There are several causes of hyperkalemia which have been enlisted in Table 37.2. True gain of potassium is often due to hemolysis, rhabdomyolysis, burns or tumour lysis. Redistribution of potassium occurs in metabolic acidosis (extracellular shift), with beta-blocker therapy and in severe insulin deficiency. Hyperkalemia is a feature of hypoaldosteronism due to Addison’s disease or acute on chronic renal failure. Drugs known to cause hyperkalemia include potassium-sparing diuretics, non steroidal anti-inflammatory drugs (NSAIDs), and the angiotensin converting enzyme (ACE) inhibitors. Genetic causes of hyperkalemia are Type 4 renal tubular acidosis (RTA-4) and hyperkalemic periodic paralysis.
The clinical picture of hyperkalemia depends upon the cause. The most common scenario is of acute on chronic renal failure with fluid overload, hypertension and metabolic acidosis, which are characteristic features of uremia. Sometimes, hyperkalemia is a part of diabetic ketoacidosis. At other times, burns and crush-injuries with rhabdomyolysis are associated with hyperkalemia. Severe hyperkalemia can cause serious ventricular arrhythmias.
172 |
|
Section 11 Typical ECG Abnormalities |
|
|
|
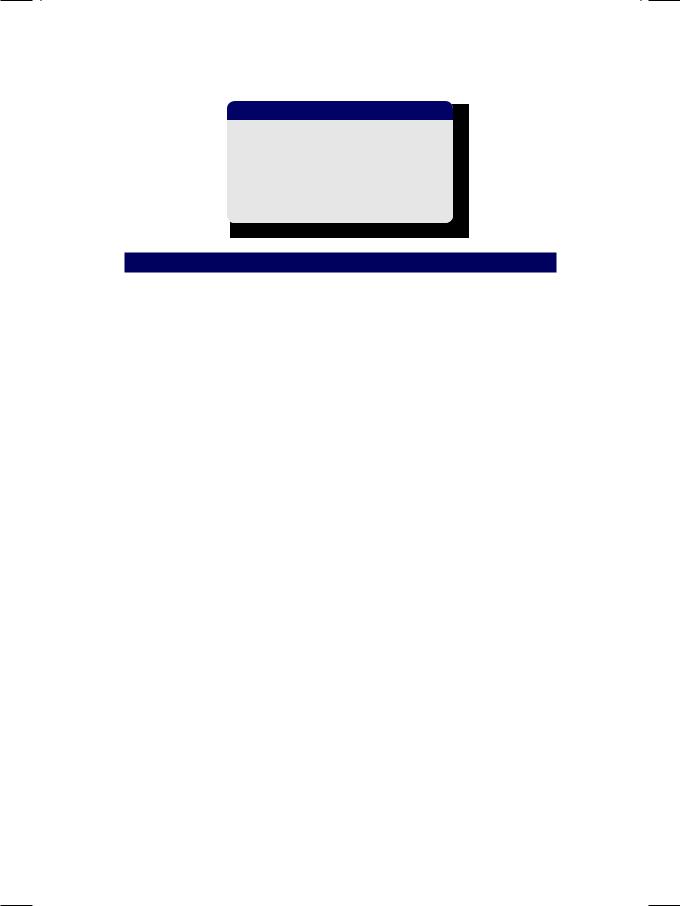
Table 37.3: Management of hyperkalemia
• Calcium gluconate injection • Glucose-insulin infusion
• Nebulized salbutamol • Oral polystyrene resin • Hemodialysis
MANAGEMENT ISSUES
Since hyperkalemia can cause serious ventricular arrhythmias, the first priority is to protect the heart. Calcium gluconate has membrane stabilizing properties and is administered intravenously as 10 ml of 10% injection over 10 minutes. The next step is to drive potassium into the cells using 100 ml of 25% glucose with 10 units of insulin given by an infusion. Nebulized salbutamol increases the urinary excretion of potassium by increasing the Na-K-ATPase pump activity. Excess potassium in the body can be depleted by potassium-binding resin like polystyrene sulphonate administered orally. Finally, if severe hyperkalemia is associated with metabolic acidosis and fluid overload, hemodialysis is the answer (Table 37.3).

S E C T I O N
12
Electrocardiac
Syndromes
