

224 PANCREAS, ARTIFICIAL
are used, but these options are based on the standard pacing approaches.
Implantable defibrillators can have an additional pacing function so that if the heart stops rather than developing ventricular fibrillation, pacing can be initiated. The pacing technology is exactly the same as for pacemakers described above, except that the electrode system will be different.
Devices are used for control of tachyarrhythmias. These devices, rather than using the regular pacing interval, usually use a series of pacing intervals at different rates to terminate the arrhythmia.
Some patients in heart failure were, in the past, often assumed to be untreatable unless by heart transplantation. Much can now be done for these patients, including pacing in all four cardiac chambers, which maximizes the pumping function of the heart by pacing the left as well as the right heart chambers, and pacing the atria and ventricles with an appropriate atrio-ventricular delay. This solution requires complex and multiple leads, and as these leads are used in sick patients, success is not always assured. Many of these patients may also require a defibrillation function.
FUTURE
Cardiac pacing had a small beginning but has grown at a steady rate each decade. With an aging population, the need for pacing will continue to grow. The development and production of pacemakers will remain a major medical device industry.
Of those devices currently available, increased use of physiological or rate responsive devices is likely as clinical studies prove their clinical value to patients, especially those who are active.
Technical advances will, to some extent, be dependent on the production of improved batteries, and then the decision will be either to make them smaller, last longer, or power more microprocessor technology. Improved electrode design to reduce energy requirements could also make a significant impact in reducing pacing pulse energy, and hence overall energy requirements. Improvements in setting the optimum AV delay will help many patients and, in particular, children who are active. Increased ability to store intracardiac data for review will ensure more research into effective use of pacing.
Pacing will continue as an essential therapeutic technique, saving lives and bringing some normality to patients with abnormal physiological heart rate control.
BIBLIOGRAPHY
1.Trohman RG, Kim MH, Pinski SL. Cardiac pacing: The state of the art. Lancet 2004;364:1701–1719.
2.ACC/AHA/NASPE 2002 guideline update for implementation of cardiac pacemakers and antiarrhythmia devices. American College of Cardiology and the American Heart Association; 2002.
3.Gold MR. Permanent pacing: New indications. Heart 2001;86: 355–360.
4.Senning A. Problems in the use of pacemakers. J Cardiovasc Surg 1964;5:651–656.
5.Greatbatch W, Chardack W. A transistorized implantable pacemaker for the long-term correction of complete heart
block. Trans Northeast Electron Res Eng Meet Conf 1959; 1:8.
6.Chardack WM, Gage AA, Greatbatch W. A transistorized, selfcontained, implantable pacemaker for the long-term correction of complete heart block. Surgery 1960;48:643–654.
7.Elmqvist R. Review of early pacemaker development. PACE 1978;1:535–536.
8.Parsonnet V, Furman S, Smyth NP. Implantable cardiac pacemakers: Status report and resource guideline (ICHD). Circulation 1974;50:A21–35.
9.Bernstein AD, Camm AJ, Fletcher RD, Gold RD, Rickards AF, Smyth NPD, Spielman SR, Sutton R. The NASPE/BPEG generic pacemaker code for antibradyarrhythmia and adap- tive-rate pacing and antiachyarrhythmia devices. PACE 1987;10:794–799.
10.Bernstein AD, Daubert J-C, Fletcher RD, Hayes DL, Luderitz B, Reynolds DW, Schoenfeld MH, Sutton R. The revised NASPE/BPEG generic code for antibradycardia, adaptiverate, and multisite pacing. PACE 2002;25:260–264.
11.Mond HG, Irwin M, Morillo C, Ector H. The world survey of cardiac pacing and cardiovertor defibrillators: Calendar year 2001. PACE 2004;27:955–964.
12.National Institute of Clinical Excellence. Technology Appraisal 88, Dual-chamber pacemakers for symptomatic bradycardia due to sick sinus syndrome and/or artrioventricular block. London, UK: National Institute of Clinical Excellence; 2005.
13.Schaldach M. Electrophysiology of the Heart: Technical Aspects of Cardiac Pacing. Berlin: Springer-Verlag; 1992.
14.Webster JG, ed. Design of Cardiac Pacemakers. Piscataway, NJ: IEEE Press; 1995.
15.Greatbatch W, Lee J, Mathias W, Eldridge M, Moser J, Schneider A. The solid state lithium battery. IEEE Trans Biomed Eng 1971;18:317–323.
16.Hill WE, Murray A, Bourke JP, Howell L, Gold R-G. Minimum energy for cardiac pacing. Clin Phys Physiol Meas 1988;9: 41–46.
See also AMBULATORY MONITORING; BIOELECTRODES; BIOTELEMETRY;
DEFIBRILLATORS; MICROPOWER FOR MEDICAL APPLICATIONS.
PAIN CONTROL BY
ELECTROSTIMULATION. See TRANSCUTANEOUS
ELECTRICAL NERVE STIMULATION (TENS).
PAIN SYNDROMES. See BIOFEEDBACK.
PANCREAS, ARTIFICIAL
ROMAN HOVORKA
University of Cambridge
Cambridge, United Kingdom
INTRODUCTION
In 2000, some 171 million people worldwide had diabetes. By 2030, a conservative forecast suggests that this number will increase to 366 million attaining epidemic proportions as the prevalence increases from 2.8 to 4.4% in all age groups (1) due to, primarily, a relative increase in developing countries (2).
Diabetes is a group of heterogeneous chronic disorders characterized by hyperglycemia due to relative
or absolute insulin deficiency. Two major categories of diabetes are recognized according to aetiology and clinical presentation, type 1 diabetes and type 2 diabetes. More than 90% cases are accounted for by type 2 diabetes. Regional and ethnic differences in diabetes incidence and prevalence exist.
Type 1 diabetes is one of the most common chronic childhood disease in developed nations (3), but occurs at all ages. Type 1 diabetes is caused by autoimmune destruction of pancreatic islet beta-cells resulting in the absolute loss of insulin production. Treatment demands the administration of exogenous insulin. Type 1 diabetes is associated with a high rate of complications normally occurring at young ages placing a considerable burden on the individual and the society.
Type 2 diabetes is caused by insulin resistance and relative insulin deficiency, both of which are normally present at the diagnosis of the disease. Environmental and polygenic factors contribute to these abnormalities (4), but specific reasons for their development are not known. A considerable number of subjects with type 2 diabetes progresses to insulin dependency.
The persistent hyperglycemia in diabetes is associated with long-term complications and dysfunction of various organs, especially the eyes, kidneys, nerves, heart, and blood vessels. The Diabetes Control and Complications Trial (DCCT) (5) and the United Kingdom Prospective Diabetes Study (UKPDS) (6) demonstrated that tight glycaemic control reduces the risk of long-term complications of type 1 and type 2 diabetes reducing the cost to the healthcare system (7). There is no threshold for the relationship between blood glucose, that is, glycosylated hemoglobin (HbA1C) and reduced risk. This indicates that glucose levels in subjects with type 1 or 2 diabetes should be as close as possible to those observed in healthy subjects. However, tight glucose control is associated with an increased risk of hypoglycemia (8), which acts as a limiting factor to the effective diabetes management.
In health, insulin is secreted by the pancreas in a highly controlled fashion to maintain the plasma glucose concentration within a narrow physiological range. In type 1 diabetes, insulin is delivered exogenously to mimic the basal and postprandial insulin needs. The standard therapy is based on multiple insulin injections using a combination of shortand long-acting insulin analogs supported by blood glucose self-monitoring (9). Treatment by the continuous subcutaneous insulin infusion (CSII), that is, using insulin pumps, is on the rise (10).
The present review is limited to the artificial electromechanical endocrine pancreas, which has the potential to revolutionize diabetes management. The artificial pancreas replaces the glucose sensing and insulin delivery by beta-cells and is therefore sometimes called an ‘‘artificial beta-cell’’. It consists of three components, a glucose monitor to measure continuously glucose concentration, a titrating algorithm to compute the amount of insulin to be delivered, and an insulin pump to deliver the insulin. Only few prototypes have been developed and tested in a controlled clinical environment. Further progress depends on advancements of continuous glucose monitoring (11).
PANCREAS, ARTIFICIAL |
225 |
HISTORICAL BACKGROUND
The hormone insulin was discovered by Banting and Best in 1921. The first patient was treated a year later in 1922.
The first reported continuous ex vivo glucose measurement in humans was by Weller et al. in 1960 (12). In 1964, Kadish (13) was first to use continuous real-time glucose monitoring in a subject with diabetes to close the loop. The system employed an intravenous (iv) infusion of insulin and glucose, which could be switched on or off, denoted as an ‘‘on–off system’’. At that time, no suitable computational means were available.
In 1974, two groups developed a true ‘‘artificial endocrine pancreas’’. Albisser et al. (14,15) in Toronto and Pfeiffer et al. (16) in Ulm combined continuous glucose monitors with algorithms implemented on a microcomputer to automate iv delivery of insulin and glucose. The first commercial device, the Biostator (17) (Life Science Instruments, Miles, Elkhart, IN) was put into production in 1977 thanks to the determination by Clemens. The golden age of the Biostator was between late 1970s and early 1980s. It is still used for research purposes.
The last two decades have witnessed a considerable technological progress. Between 1999 and 2005, five continuous or semicontinuous monitors have received regulatory approval in the United States or Europe and further are under development (18). Since the introduction of continuous subcutaneous insulin infusion (CSII) (19), insulin pumps have been miniaturized and their reliability improved (20). Advanced titrating algorithms have been developed.
PHYSIOLOGICAL CONSIDERATIONS
Pancreas
The pancreas has digestive and hormonal functions. It is divided into the endocrine tissues secreting hormones insulin, glucagons, and somatostatin, and the exocrine tissues secreting digestive enzymes.
The endocrine tissues consist of many small clusters of cells called islets of Langerhans. Humans have roughly 1 million islets. Three major cell types are located in islets. Alpha-cells secrete the hormone glucagon. Beta-cells produce insulin and are the most abundant of the islet cells. Delta-cells secrete the hormone somatostatin.
Endogenous Insulin Secretion
Pancreatic beta-cells secrete insulin by sensing the levels of nutrients, such as glucose and certain amino acids. The beta-cells therefore integrate the sensing and secreting functions and are efficient in maintaining glucose homeostasis.
Four different phases of insulin secretion can be identified (21). Basal insulin secretion represents insulin released in the postabsorptive state. The cephalic phase of insulin secretion is evoked by the sight, smell, and taste of food before its digestion or absorption and is mediated by pancreatic innervations. The early-phase relates to the first 0–30 min postmeal insulin secretion, whereas the
226 PANCREAS, ARTIFICIAL
late-phase relates to the secretion between 60 and 120 min. During all phases, insulin is secreted in a pulsatile fashion with rapid pulses occurring every 8–15 min superimposed on slower, ultradian oscillations occurring every 80– 120 min.
Insulin secretion is induced by other energetic substrates besides glucose, such as amino acids and drugs. Incretin hormones, such as glucagon-like peptide-1 (GLP–1) and to a lesser extent, glucose-dependent insulinotropic polypeptide (GIP), are responsible, in part, for the higher insulin secretory response after oral compared to the intravenous glucose administration.
COMPONENTS
The artificial pancreas consists of three components, a glucose monitor to measure glucose concentration, an algorithm to decide the amount of insulin to be delivered, and a device delivering insulin. This is a minimum setup. Some argue that a safe system should include a device for the delivery of glucose but all existing prototypes, with the exception of the Biostator, avoid the delivery of glucose.
The glucose monitor could be an implantable or extracorporeal device and based on a minimally or noninvasive technology (22). Generally, the implantable sensors are projected to have several months to years lifetime whereas the nonimplantable devices have, at present, lifetime of one-half of a day to several days.
Similarly, the insulin pump can be implanted or extracorporeal. The implantable pump normally delivers insulin intraperitoneally whereas the extracorporeal insulin pump delivers insulin subcutaneously.
The control algorithm can be implemented on a separate device or on the same platform as the insulin pump. The communication between the devices can be achieved using wire or wireless technologies. The latter are becoming prevalent for the transfer of data from insulin pumps onto diabetes management systems. Integrated systems exist which allow wireless transfer of data between glucose meters and insulin pumps such as the ‘‘all-in-one’’ CozMore Insulin Technology System (Smiths Medical MD, Inc. MN).
TYPES OF ARTIFICIAL PANCREAS
Meal Time Insulin Delivery
Artificial pancreas can handle meal delivery in different ways. In a ‘‘fully closed-loop’’ setting, the artificial pancreas delivers insulin without information about the time or size of the meal. Insulin is administered purely by evaluating the glucose excursions and the system works autonomously.
Alternatively, the artificial pancreas is provided with information about the time and size of the meal. The controller generates an advice, in an open-loop manner, on prandial insulin bolus. This can be termed ‘‘closed–loop with meal announcement’’ or ‘‘semiclosed-loop’’ control.
Other ways exist to handle the meal-related insulin delivery, but most systems adopt a fully closed-loop or semiclosed-loop setting.
Body Interface
Depending on body interface, three major types of artificial pancreas are recognized, (i) the subcutaneous (sc) sensing and sc delivery (sc–sc) system, (ii) the iv sensing and intraperitoneal (ip) delivery (iv–ip) system, and (iii) the iv glucose sensing and iv insulin delivery (iv–iv) system. The approaches differ in their invasiveness and associated kinetic delays (11).
Subcutaneous: Subcutaneous Body Interface
As a minimally invasive solution, the sc–sc approach has the potential to achieve a widespread application. However, it is unlikely to be compatible with a fully closed-loop system due to considerable delays disallowing effective compensation of large disturbances, such as meals.
The overall delay from the time of insulin delivery to the peak of its detectable glucose lowering effect is 100 min (11). This consists of a 50 min delay due to insulin absorption with short-acting insulin analogs (23), 30 min and more due to insulin action (24), 10 min due to interstitial glucose kinetics (25), and 10–30 min due to the transport time for ex vivo based monitoring system, such as those based on the microdialysis technique (26).
It is likely that users of the sc–sc approach will have to enter nutritional information to assist in the delivery of the prandial insulin dose. Most present prototypes adopt the sc–sc approach.
Intravenous: Intraperitoneal Body Interface
The iv–ip can benefit from existing intraperitoneal insulin pumps. The delays in the system are about 70 min, which comprises a 40 min time-to-peak of plasma insulin following intraperitoneal administration and a 30 min delay due to insulin action (11). Additionally, a delay due to kinetic properties of the glucose sensor applies, such as a 16 min kinetic and transport delay introduced by the long-term sensor system (27). It is unclear whether a fully closed-loop system can be developed under such circumstances.
The drawback of the iv–ip route is considerable invasiveness and relative inexperience with intraperitoneal compared to subcutaneous insulin pumps. Only > 1000 intraperitoneal pumps have been implanted so far (28) compared to > 200,000 subcutaneous pump users (29). Intraperitoneal insulin can be delivered by an implantable insulin pump Minimed 2007 (28) or via an indwelling intraperitoneal catheter such as DiaPort by Disetronic.
Intravenous: Intravenous Body Interface
The iv–iv approach was the first to have been investigated. It is embodied by the Biostator device. At present, the iv–iv approach is usable at special situations, such as in critically ill patients, surgical operations, or for research investigations. The drawback of the approach is its invasiveness requiring vascular access for both glucose monitoring and insulin delivery and is associated with a high risk of complications arising from, for example, biocompatibility issues.
The benefit of the approach is that the kinetic delays,30 min due to the delay in insulin action, are minimized enabling the development of a fully closed-loop system.
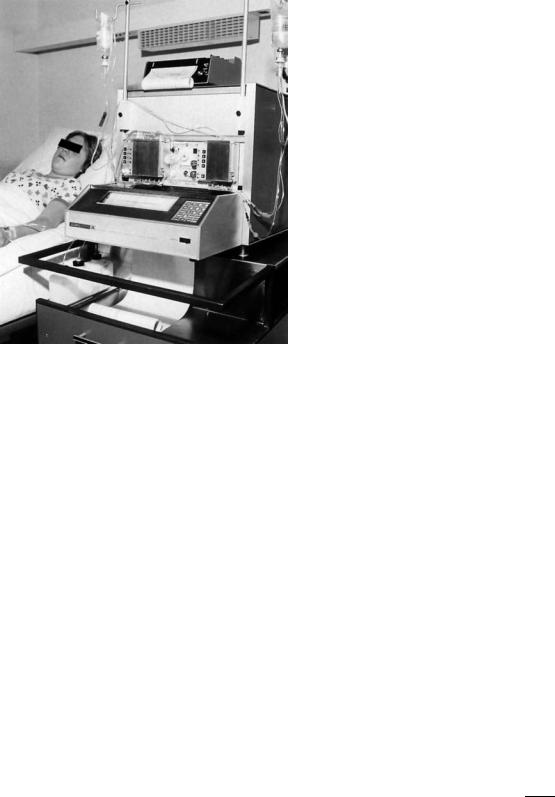
Figure 1. Biostator is the first commercial artificial endocrine pancreas. (Courtesy of Dr. Freckmann, Institute for Diabetes Technology, Ulm, Germany.)
PROTOTYPES
Biostator
Introduced in 1977, the Glucose-Controlled Insulin Infusion System (GCIIS), trademark name Biostator, is a modular, computerized, feedback control system for control of blood glucose concentrations (17), see Fig. 1. The Biostator is an example of an iv–iv system working in the fully closedloop mode.
The Biostator was developed to normalise glucose in acute metabolic disturbances such as during diabetic ketoacidosis. However, its primary use has been in research investigating insulin sensitivity by the method of the glucose clamp and assessing insulin requirements and associated inter and intrasubject variability in subjects with type 1 diabetes and other conditions.
The rapid on-line glucose analyzer uses whole blood utilising a glucose oxidase sensor in the measurement process. The analyzer demonstrated both shortand long-range stability based on a two-point calibration.
The nonlinear proportional-derivative controller uses a five-point moving average smoothing and titrates insulin or dextrose intravenous infusion using a multichannel peristaltic infusion system to achieve user-defined glucose concentration. A printer records, on a minute-by-minute basis, the glucose value measured, the insulin and/or dextrose infusion rates, and the cumulative total of the insulin infused. A serial RS232 link allows these data to be downloaded to an external computer. The system response is < 90 s including transport of blood from the patient.
PANCREAS, ARTIFICIAL |
227 |
Although a pioneering device, the Biostator suffers from serious limitations. It needs constant technician’s supervision. It discards continuously venous blood at a rate of 50 mL per 24 h. The control algorithm is oversimplistic. The original insulin titrating algorithm was linked to the rate of glucose change by Albisser et al. (14) with modifications, for example, by Botz (30), Marliss et al. (31), and Kraegen et al. (32) to reduce postprandial hyperglycemia and hyperinsulinemia. The algorithms require individualization by assigning values to constants. No formal adaptive approach was used to support the assignment, which is based on heuristics. These and similar algorithms were reviewed by Broekhuyse et al. (33), who concluded that none of the algorithms was superior and that further work was required to achieved normalization of the glucose concentration.
Over 200 devices have been sold worldwide. The Biostator contributed to the development and acceptance of the present gold standard in the diabetes management by multiple daily injections. At present, it is used for research purposes to evaluate diabetes drugs and technologies. The number of functioning prototypes counts in tens as spare parts run out. The Glucostator (mtb GmbH, Lonsee, Germany) is a CE-marked device recently marketed to replace the aging Biostator devices.
Shichiri’s Group
Professor Shichiri and co-workers, Kumamoto, Japan, has developed as early as in 1975, a prototype of an iv–iv artificial endocrine pancreas (34) made later into a compact bedside version, STG-22 (Nikkiso Co. Ltd., Japan) (35) with a similar properties to the Biostator. The device is still marketed. STG-22 uses a glucose sensor for continuous glucose monitoring by combining the immobilised glucose oxidase membrane glucose enzyme sensor measuring hydrogen peroxide.
Following on, the group developed a prototype wearable artificial pancreas using the sc–sc route with the regular (36,37) and short acting insulin (38), and the sc–ip route (39). The latest versions use a microdialysis-type (40) or a ferrocene-mediated needle-type (39) glucose sensor working over a period of 7 days without any in vivo calibration (i.e., without using blood glucose measurement to calibrate the glucose sensor) followed by 14 days with one point calibration (41).
The results of the performance of their closed-loop system are even more impressive. With a fully closed sc–sc route using short acting insulin Lispro, the group claimed to have achieved ‘‘perfect’’ normalization of blood glucose over 24 h (38,42).
These results are surprising given that the control algorithm was a simple, nonadaptive PD controller in
the form |
|
|
|
|
|
|
|
IIR t |
K |
G t |
K |
dGðtÞ |
þ |
K |
|
D dt |
|
||||||
ð Þ ¼ |
P |
ð Þ þ |
|
|
C |
where IIR(t) is insulin infusion rate, G(t) is the monitored glucose concentration, and KP, KD, and KC are constants, which are dependent on the type of insulin delivery, subcutaneous versus intravenous, and also on the type of insulin, regular versus short-acting insulin lispro (38,43).

228 PANCREAS, ARTIFICIAL
These enviable groundbreaking results, however, failed to be confirmed by other groups. The achievements of the group are summarized in an edited monograph (34).
Minimed: Medtronic
The Continuous Glucose Monitoring System (CGMS; Medtronic MiniMed, Northridge CA) (44) is the first commercial continuous glucose monitor. Approved in 1999, CGMS adopts a Holter-style monitoring to store up to 3-day data for retrospective analysis.
The CGMS employs an electrochemical sensor inserted into the subcutaneous tissue adopting the hydrogen per- oxide-based enzyme electrode (45), which provides signal every 10 s. Calibration is achieved using self-monitoring of blood glucose. The new ‘‘gold’’ sensor introduced in November 2002 is more accurate than the original sensor [the mean absolute deviation 0.83 vs 1.11 mmol L 1 (46)].
Employing the CGMS sensor, an external physiologic insulin delivery (ePID) has been developed by Minimed– Medronic. The system uses a PID controller (47), which was designed to reproduce the first phase insulin secretion by linking insulin administration to the rate of change in glucose concentration (the proportional component of the controller) and the second phase by linking insulin administration to the difference between the ambient and target glucose (the integrative component of the controller).
First studies with a fully closed loop were executed in dogs (48). The example presented in (49) shows peak postmeal glucose of 15 mmol L 1 with the set point reached in 11 h indicating a suboptimal performance of a fully closed loop with the sc–sc approach. The adaptation of the PID controller was achieved by assigning the proportional gain KP a value resulting in a normal daily insulin dose of the dog at euglycemia (48).
An evaluation of the ePID system in six subjects with type 1 diabetes > 27.5 h resulted in preprandial and postprandial (2 h) glucose levels at 5.8 1.2 and 9.8 1.6 mmol L 1 (mean SD) (50). Morning glucose after overnight control was 6.8 1.0 mmol L 1.
Roche Diagnostics
The sc–sc closed-loop prototype with meal announcement (51,52) developed by Roche adopted the subcutaneous continuous glucose monitor (SCGM1; Roche Diagnostics GmbH, Manheim, Germany), which has been designed to monitor glucose in the subcutaneous interstitial fluid for up to 4–5 days (53).
SCGM1 is based on the microdialysis technique with an ex vivo glucose measurement. The sensor produces a signal every second. This is reduced to one glucose measurement every 5 min. Calibration is required once every 24 h (26,53). SCGM1 has a low flow rate (0.3 mL min 1), achieves a 100% recovery of the subcutaneous glucose in the dialysate, but has a 30 min technical lag. In vitro performance is excellent with a mean absolute difference of 0.2–3.8% in 10 sensor units (53).
An ‘‘empirical algorithm’’ (51) was develop to titrate sc insulin. A set of rules, derived from clinical observations, determine the insulin bolus administered every 10 min.
The closed-loop system with meal announcement was tested in 12 well-controlled (HbA1C< 8.5%) subjects with type 1 diabetes (51). Control lasted over 32 h and included the digestion of breakfast, lunch, dinner, and a snack. The target glucose concentration for the algorithm was 6.7 mmol L 1. Prandial bolus was calculated from the carbohydrate content of the meal.
The algorithm achieved a near-target monitored glucose concentration (6.9 vs. 6.2 mmol L 1; mean, algorithm vs. self-directed therapy) and reduced the number of hypoglycemia interventions from 3.2 to 1.1 per day per subject. During the algorithm therapy, 60% of SCGM1 values were within the 5–8.3 mmol L 1 range compared to 45% with the self-directed therapy.
Adicol Project
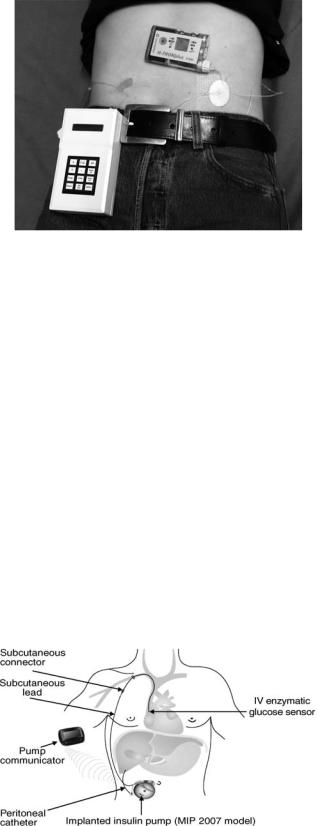
The project Advanced Insulin Infusion using a Control Loop (Adicol) (54) was an EC funded project that completed at the end of 2002. The Adicol’s sc–sc closed loop with meal announcement consisted of a minimally invasive subcutaneous glucose system, a handheld PocketPC computer, and an insulin pump (Disetronic D-Tron) delivering subcutaneously insulin lispro, see Fig. 2.
As continuous sensor was developed in parallel with the control algorithm and was not sufficiently stable, throughout the Adicol project, the intravenous glucose measurement was used, delayed by 30 min to simulate the lag associated with sc glucose sampling.
Adicol adopted an adaptive nonlinear model predictive controller (MPC) (55), which included a model based on a two compartment representation of glucose kinetics (24)
Figure 2. Components used by the Adicol’s biomechanical artificial pancreas. Top left corner shows the microperfusion probe connected to the glucose monitor, which includes microfluidics components, Bluetooth communication, and the sensor. The handheld iPAQ PocketPC maintains wireless communication with the other two components, runs the MPC controller. Disetronic D-Tron insulin pump is equipment with a special sleeve visible on the left hand side of the pump which converts the Bluetooth radiofrequency signal to an infrared signal accepted by the pump (reprinted with permission from (54)).
extended by submodels representing the absorption of short acting insulin lispro, the insulin kinetics, the renal clearance of glucose, and the gut absorption. The MPC approach was combined with an adaptive Bayesian technique to individualize the glucoregulatory model to represent the interand intrasubject variability. The individualization was integrated within the control algorithm and was executed at each 15 min control cycle.
The largest clinical study performed in the Adicol project assessed the efficacy of the MPC controller with 30 min delayed glucose sampling > 26 h in 11 subjects with type 1 diabetes. Glucose was normalized from 1400 to 1800. Dinner followed with an individually determined prandial bolus at 1800, and control by the MPC from 1930 to 2200 the following day.
One hypoglycemia event (touchdown at 3.3 mmol L 1) due to the MPC control was recorded. The highest glucose concentration was 13.3 mmol L 1 following breakfast; 84% of glucose measurements were between 3.5 and 9.5 mmol L 1 (56).
Following the completion of the Adicol project, a viscometric sensor (57) was tested with the MPC algorithm. Five subjects with type 1 diabetes treated by CSII were studied for 24 h (58). No hypoglycemia event (< 3.3 mmol L 1) due to the MPC control was observed. Overall, 87% sensor values were between 3.5 and 9.5 mmol L 1. Outside the 3 h postmeal periods, 74% of sensor measurements were in the range 3.5–7.5 mmol L 1.
Institute for Diabetes Technology, Ulm
Building on foundations laid by Professor Pfeiffer in the early 1970s, the work in Ulm continues (59).
The group used the amperometric–enzymatic approach in combination with the microdialysis technique. The continuous flow method uses a slow continuous flow through the tubing achieving nearly a 100% recovery with a 30 min lag (59). The comparative method does not require calibration (60). Saline with glucose (5.5 mmol L 1) is pumped through the probe in a stop-flow mode. During the stop mode, a nearly 100% equilibrium between the interstitial plasma glucose and the perfusate is achieved. In the flow mode, the dialysate is pumped rapidly to the sensor chamber. The technique facilitates sensor internal calibration for each measuring cycle and yields five glucose measurements per hour.
The group developed and tested an sc–sc closed-loop approach with meal announcement (61,62), see Fig. 3.
The algorithm uses the basal insulin need, determined from an individual insulin need, and a postprandial insulin need, expressed as an insulin/carbohydrate ratio. A model exploits these values and predicts future glucose excursions. The algorithm was tested in eight subjects with type 1 diabetes over a period of 24 h. The average glucose value was 7.8 0.7 mmol L 1 (mean SD). The postprandial increases were at 2.9 1.3 mmol L 1 with largest excursions recorded after breakfast. One hypoglycemia (< 3.3 mmol L 1) was observed (62).
EVADIAC Group
Exploiting the progress made by the French group on implantable pumps ‘‘Evaluation dans le Diabete du Traite-
PANCREAS, ARTIFICIAL |
229 |
Figure 3. The system V4-IDT from the ULM group. The system uses a glucose monitor based on microdialysis integrated with a portable computer and an H-Tron pump, Disetronic. (Courtesy of Dr. Freckmann, Institute for Diabetes Technology, Ulm, Germany.)
ment par Implants Actifs’’ (EVADIAC), the work by Renard et al. is at the forefront of the fully closed-loop iv–ip approach. The group has developed the implantable physiologic insulin delivery (iPID) system, which uses a longterm sensor system (LTSS) (63,64).
Long-term sensor system, an intravenous enzymatic oxygen-based sensor developed by Medtronic MiniMed (Northridge CA), is implanted by direct jugular access in the superior vena cava. It is connected by a subcutaneous lead to an insulin pump delivering insulin intraperitoneally and implanted in the abdominal wall, see Fig. 4. The pump implements a PD controller similar to that used by the ePID system.
The system has been investigated in subjects with type 1 diabetes with collected data per sensor of 280 days (65). Most investigations with LTSS have adopted the open-loop approach. The fully closed-loop system was tested > 48 h reducing % time spent at < 3.9 mmol L 1 from 18 to 6%, and % time spent at > 13.3 mmol L 1 from 17 to 2%. The addition of insulin bolus at meal time, all glucose values were inside the range 3.9–13.3 mmol L 1.
Figure 4. Scheme of human implantation of the Long-Term Sensor System (LTSS, Medtronic-MiniMed), a prototype of artificial pancreas. (Courtesy of Dr. Renard, Lapeyronie Hospital, Montpellier, France.)
230 PANCREAS, ARTIFICIAL
Recently, the iPID system was evaluated in four elderly lean subjects with type 1 diabetes over 48 h (66). During the second 24 h control period following empirical tuning of the algorithm, 4 and 7% of time was spent < 4.4 mmol L 1 in the postprandial (0–2 h) and outside meal conditions, respectively, 12 and 32% was spent in the region 4.4–6.7 mmol L 1, 63 and 60% was spent in
the region 6.7–13.3 mmol L 1, and 20 and 2% was spent > 13.3 mmol L 1.
CLINICAL STUDIES
Clinical studies performed with prototypes of an artificial pancreas in subjects with type 1 diabetes are summarized in Table 1. All experiments were performed in hospital environment. No prototype has yet been studied in home settings.
Table 1 excludes numerous experiments carried out with the Biostator as the invasiveness and the setup adopted by the device does not permit development into a routinely used system.
Numerous experiments have been carried out in pancreatectomized dogs especially in the early phases of prototype development. This includes the ePID system (48), but some approaches such as that adopted by the Adicol project, did not use testing on animal models, but adopted testing on a simulation environment (82).
INDICATIONS
Artificial pancreas has the potential to be used in various disease conditions. For subjects with type 1 diabetes, the system offers ‘‘cure’’ especially if implemented as a fully closed-loop iv–ip system. Realistically, first prototypes for home setting are expected to adopt the sc-sc route with meal announcement and thus participation of the subjects with type 1 diabetes in the disease management process is required. Fail-safe procedures are needed for such a setup.
An increasing proportion of subjects with type 2 diabetes is treated by insulin. It has been reported that nearly 50% of subjects with type 2 diabetes require insulin treatment at some stage of their disease. The artificial pancreas could provide a solution for a subgroup of subjects with type 2 diabetes, but this has to be justified by a cost-benefit analysis.
The sc–sc route may require a continuing close subject involvement in the disease management. This would restrict the treatment group to those well motivated, who generally have good glucose control. The greatest treatment benefit would be for those with poor glucose control, but other aspects, such as psychological factors might impair or even prevent the system deployment.
A recent study in adult critically ill subjects revealed that glucose control < 6.1 mmol L 1 is associated with reduced mortality by 43%, overall inhospital mortality by 34%, newly developed kidney failure requiring dialysis by 41%, bacteremia by 46%, the number of red blood cell transfusions by 50%, and critical illness polyneuropathy by 44% (83). Although still awaiting confirmation by another
prospective study, the results indicate that artificial pancreas for critically ill is likely to bring about major improvements in therapeutic outcomes. Whether these results apply to a broader category of inpatients be it a general ward or pediatric population is yet to be determined. It is also unclear what is the most appropriate setup of a ‘‘hospital-based’’ artificial pancreas.
COST
The cost of the artificial pancreas can only be inferred from the cost of existing technology. The cost of the Biostator was $70,000 prohibiting its wider use.
Insulin pumps cost from $5,000 to 6,000. The monthly cost of pump treatment is $100. The CGMS monitor costs$4,000 and the single-use 3 day sensors cost $50 each. It is likely that the sc-sc artificial pancreas will be at least as expensive as the combined cost of the insulin pump and the glucose monitor.
The cost needs to be set against the total cost of diabetes which, in developed countries such as in the United States or the United Kingdom, is 10% of the total health care budget (84). Most of the direct expenditure is on treating diabetes complications, which could be delayed or prevented with tight glucose control.
OUTLOOK
Present technology has made considerable advances toward a truly personal wearable treatment system. The lack of availability of a glucose monitor with adequate properties appears to hinder further progress and the development of a commercially viable system. The algorithms need to be improved and subjected to rigorous clinical testing.
With regard to the existing glucose monitors, it is possible that their potential has not been fully exploited. The regulatory-driven research and development to achieve an equivalence between finger-prick glucose measurements and values provided by continuous glucose monitors in the interstitial fluid hinders the engagement of the industry and the academia in the development and testing of closedloop systems.
In the first instance, the artificial pancreas is most likely to find its wider use in the supervised hospital environment, such as at the intensive care units. The application in home settings will most likely be gradual starting with a supervised system (by the treated subjects) and increasing its autonomous function following on from wider experience.
The regulatory bodies will play an important role in the introduction of the artificial pancreas into the clinical practice. Until recently, the perception of closed-loop systems was not overly positive by the regulatory authorities. Artificial pancreas with its potential to ‘‘cure’’ diabetes, but also to lead to life-threatening complications, if malfunctioned, will have to pave the way to a new generation of closed-loop home-based biomedical devices if it is ever to succeed.
