

MusculoSkeletal Exam
.pdfPectoralis
minor
Pectoralis
major
Figure 8.62 The primary adductor of the shoulder is the pectoralis major muscle.
Chapter 8 The Shoulder
Figure 8.64 Testing shoulder adduction with gravity eliminated.
Costal view (Anterior)
Subscapularis
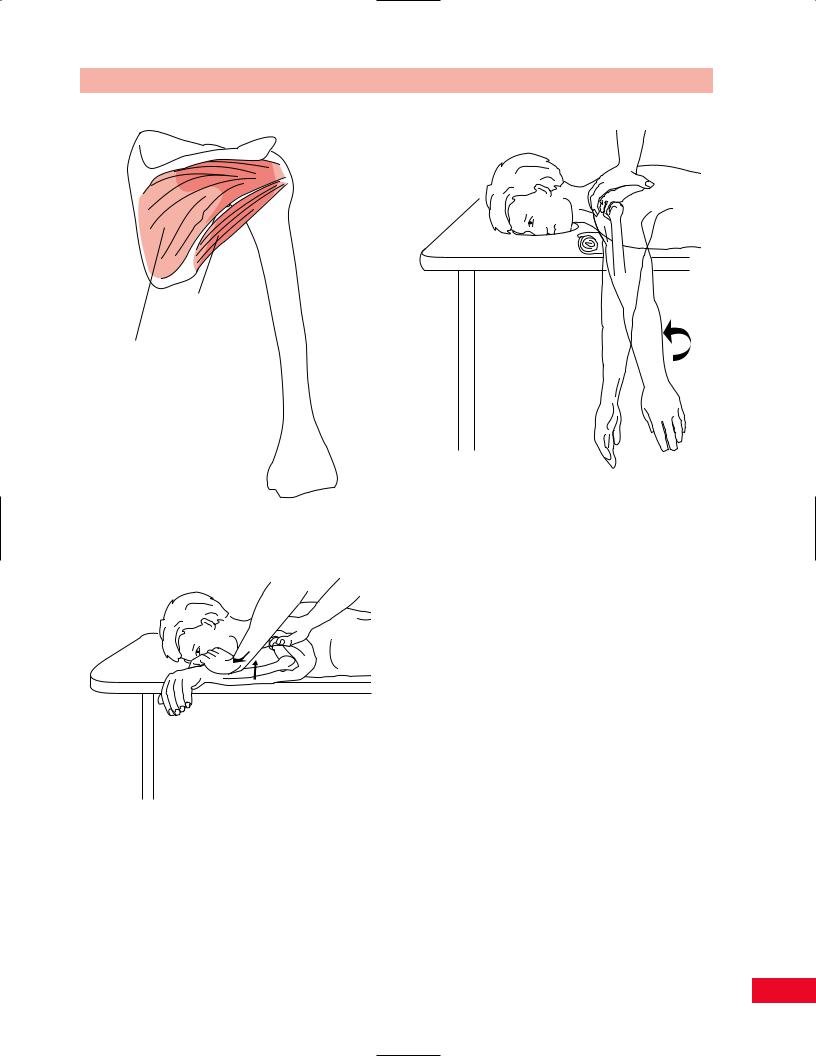
Figure 8.65 The primary shoulder internal rotators are the subscapularis, pectoralis major, and latissimus dorsi.
Figure 8.63 Testing shoulder adduction.
Painful resisted shoulder adduction can be caused by tendinitis of the contracting muscles.
Weakness of shoulder adduction can result in restricted bimanual activities. For example, carrying a heavy object at the level of the waist would be difficult.
Shoulder Internal (Medial) Rotation
The primary internal rotators of the shoulder are the latissimus dorsi, teres major, subscapularis, and pectoralis major (Figure 8.65).
•Position of patient: Prone with the arm abducted 90 degrees and the elbow flexed to 90 degrees.
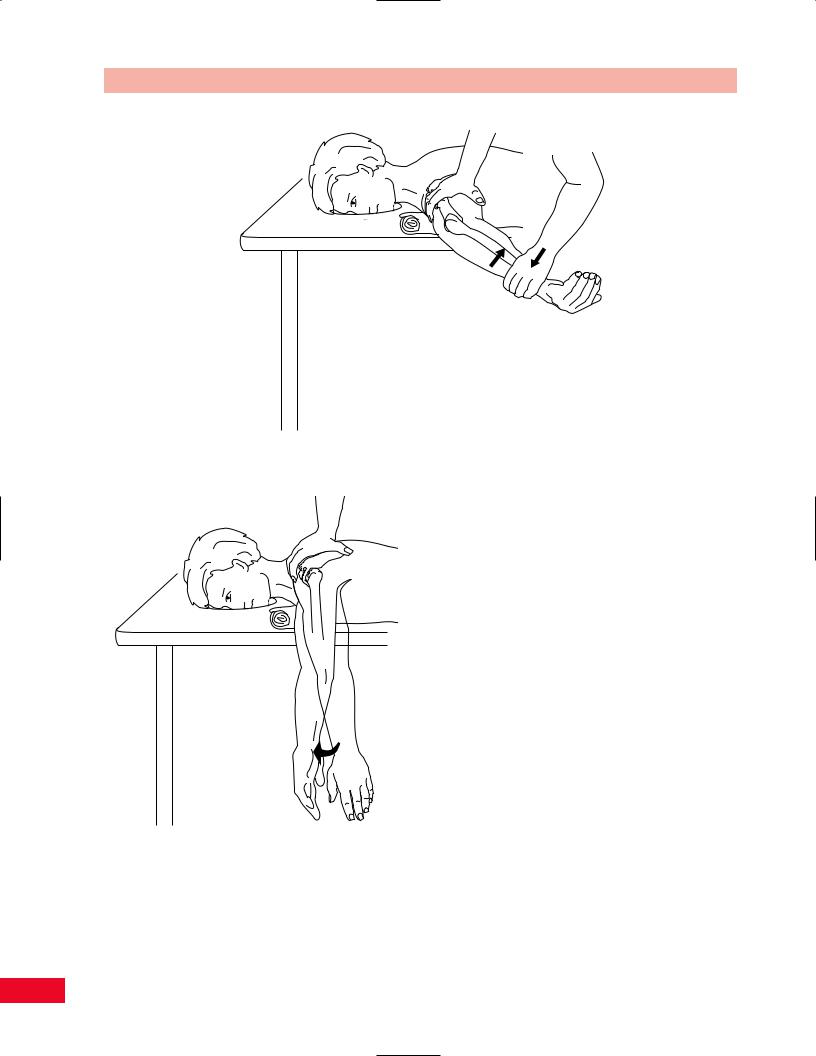
•Resisted test: Place one hand on the upper arm to stabilize it. Place your other hand above the patient’s wrist and push downward as the patient attempts to push your hand upward against your resistance (Figure 8.66).
175
The Shoulder Chapter 8
Figure 8.66 Testing shoulder internal rotation.
Figure 8.67 Testing shoulder internal rotation with gravity eliminated.
Testing shoulder internal rotation with gravity eliminated is performed by having the patient lie prone with the tested arm hanging from the table and in external rotation. The patient attempts to internally rotate the
arm from the externally rotated position while you support the scapula and thorax with your forearm and hand (Figure 8.67).
Painful internal rotation may be due to tendinitis of the working muscles.
Shoulder External (Lateral) Rotation
The external rotators of the shoulder are the infraspinatus and teres minor muscles (Figure 8.68). The posterior fibers of the deltoid muscle assist in this movement.
•Position of patient: Prone with the shoulder abducted to 90 degrees and the elbow bent at 90 degrees. The upper arm is supported by the examining table, with a pillow or folded towel placed underneath the upper arm.
•Resisted test: While stabilizing the scapula with the palm and fingers of one hand, take the patient’s arm just above the wrist with your other hand and apply downward
resistance as the patient attempts to upwardly rotate the shoulder so that the hand is elevated above the level of the examining table
(Figure 8.69).
Testing shoulder external rotation with gravity
eliminated is performed with the patient in the prone position, with the test arm dangling over the edge of
176
Chapter 8 The Shoulder
Teres minor
Infraspinatus
Figure 8.68 The primary external rotators of the shoulder are the infraspinatus and teres minor.
Figure 8.69 Testing external rotation.
the examining table in internal rotation. The patient attempts to externally rotate the arm while you stabilize the scapula with your hands (Figure 8.70).
Painful resisted external rotation may be due to tendinitis of the working muscles.
Figure 8.70 Testing external rotation with gravity eliminated.
Weakness of external rotation will prevent abduction of the shoulder to more than 95 degrees due to the impingement of the greater tuberosity of the humerus against the acromion, secondary to inability to depress the humeral head.
Scapular Elevation (Shoulder Shrug)
The primary scapular elevators are the upper trapezius and levator scapulae muscles (Figure 8.71). The rhomboid muscles assist in this movement.
•Position of patient: Standing with arms at the sides.
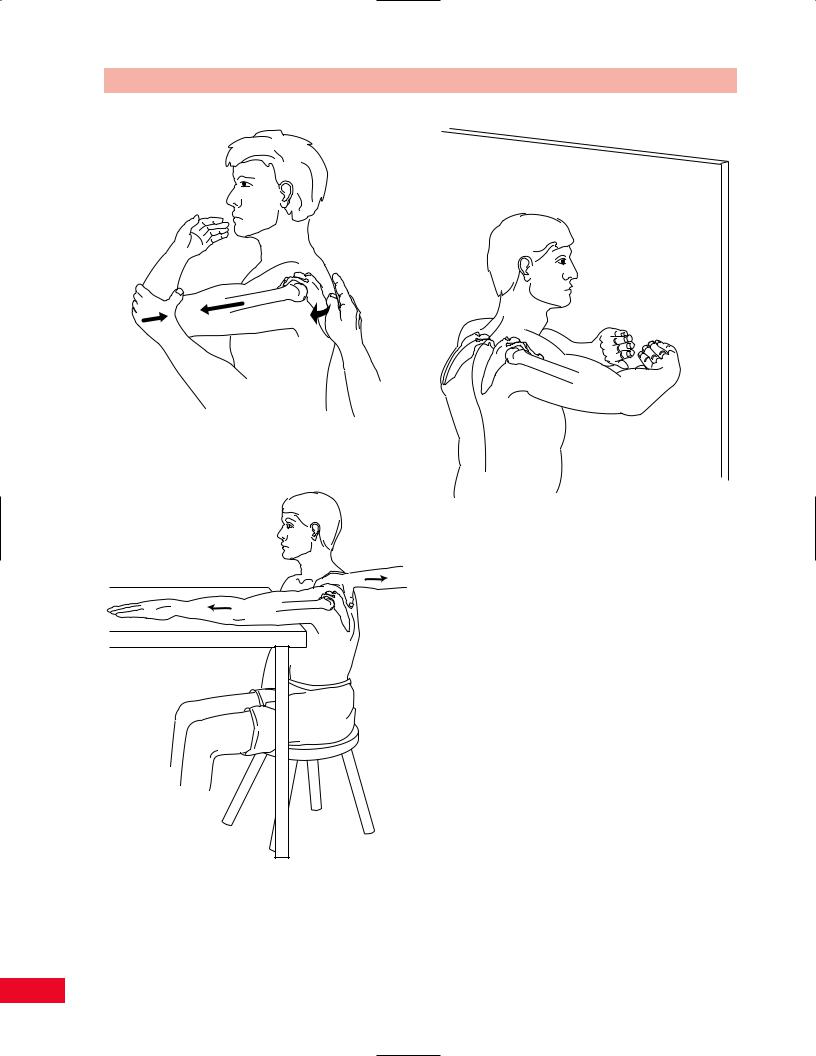
•Resisted test: Stand behind the patient, placing
each of your hands over the upper trapezius muscles. Ask the patient to shrug his or her shoulders against your resistance (Figure 8.72). Testing scapular elevation with gravity eliminated
is performed with the patient in the supine position with the arms at the sides. Ask the patient to shrug his or her shoulders in this position (Figure 8.73).
Painful resisted scapular elevation can be due to tendinitis of the working muscles or a sprain of the cervical spine.
Weakness of scapular elevation may be due to cranial nerve damage and other brain stem signs should
177

The Shoulder Chapter 8
|
Trapezius |
|
Levator |
(superior |
|
fibers) |
||
scapulae |
||
|
Figure 8.73 Testing scapular elevation with gravity eliminated.
Rhomboideus minor
Figure 8.71 The primary scapular elevators are the superior fibers of the trapezius and the levator scapulae muscles.
Rhomboideus major
Trapezius middle fibers (Overlay the rhomboids)
Figure 8.74 The scapular retractors are the rhomboideus major, rhomboideus minor, and the middle fibers of the trapezius muscles.
Figure 8.72 Testing scapular elevation.
be searched for. The spinal accessory nerve may be cut during a radical neck dissection.
Scapular Retraction
The scapular retractors are the rhomboideus major and minor muscles, assisted by the middle fibers of the trapezius (Figure 8.74).
•Position of patient: Standing with the arm adducted and the elbow slightly bent. The humerus is slightly extended.
178

Chapter 8 The Shoulder
Levator |
Trapezius (superior fibers) |
|
|
scapulae |
Trapezius (middle fibers) |
Rhomboideus minor
Rhomboideus major
Trapezius (lower fibers)
Figure 8.75 Testing scapular retraction.
•Resisted test: Stand beside the patient and place your hand so that you are cupping the elbow. Ask the patient to resist as you attempt to abduct the scapula, using his or her arm as leverage (Figure 8.75).
Testing scapular retraction with gravity eliminated
is performed with the patient in the same position. Painful scapular retraction may be due to tendinitis
of the contracting muscles or disorders of the thoracic spine.
Weakness of scapular fixation by the rhomboid muscles leads to weakness of humeral adduction and extension.
Scapular Protraction
The serratus anterior muscle is the primary scapular protractor (Figure 8.76). This muscle maintains the inferior angle of the scapula against the thoracic wall and rotates the inferior angle upward.
•Position of patient: Standing with the test arm flexed forward approximately 90 degrees and the elbow bent also about 90 degrees.
•Resisted test: Stand behind the patient and place one hand over the thoracic spine for stabilization.
Take your other hand and hold the proximal
Serratus
Anterior
Figure 8.76 The primary scapular protractor is the serratus anterior muscle.
179
The Shoulder Chapter 8
Figure 8.77 Testing scapular protraction.
Figure 8.78 Testing scapular protraction with gravity eliminated is performed with the patient in a sitting position with the arm outstretched on a table in front. Ask the patient to bring the entire extremity forward and watch for movement of the scapula away from the midline.
Figure 8.79 Medial winging of the scapula is caused by weakness of the serratus anterior muscle. This is frequently caused by damage to the long thoracic nerve (C5, C6, and C7 nerve roots).
aspect of the patient’s forearm and elbow and attempt to pull the arm backward toward you from this point while the patient attempts to push the arm forward (Figure 8.77).
Testing scapular protraction with gravity eliminated is performed with the patient in the sitting position (Figure 8.78).
Painful scapular protraction may be due to tendinitis of the contracting muscles.
Weakness of the serratus anterior muscle is frequently caused by damage to the long thoracic nerve. This nerve is comprised of the C5, C6, and C7 nerve roots. The result of weakness of this muscle is a medial winging of the scapula. This can be elicited by asking the patient to push against the wall, as shown in Figure 8.79. The scapula wings out medially because the trapezius muscle maintains the medial scapular border close to the vertebral column.
The inability to abduct and rotate the scapula prevents the patient from being able to forward flex the arm to the complete upright position (Figure 8.80).
180

Chapter 8 The Shoulder
Figure 8.80 Note that with weakness of the right serratus anterior, the patient is unable to fully rotate and abduct the scapula as compared to the left side. The result is an inability to forward flex the arm completely upward.
Neurological Examination
Motor
The innervation and spinal levels of the muscles that function in the shoulder are listed in Table 8.1.
Reflexes
The pectoralis major jerk test is performed to test the C5 nerve root and pectoralis major muscle (Figure 8.81). Perform the reflex test by having the patient lie in the supine position and placing your thumb over the tendon of the pectoralis major muscle just proximal to the shoulder joint. Tap your thumb with the reflex hammer and observe for contraction of the pectoralis major muscle. The shoulder may also adduct somewhat during this reflex. Compare your findings with those from the opposite side. This
Figure 8.81 Testing the pectoralis reflex (C5 nerve root).
reflex will be absent if there is severe injury to the pectoralis major muscle, medial and lateral pectoral nerves, upper trunk of the brachial plexus, or C5 nerve root.
Sensation
Light touch and pinprick sensation should be examined after the motor and reflex examination. The dermatomes for the shoulder are C4, C5, C6, and C7. The upper thoracic (T2, T3) dermatomes are responsible for the axilla and medial aspect of the arm (Figure 8.82). Peripheral nerves providing sensation in the shoulder region are shown in Figures 8.83 and 8.84.
Damage to the axillary or the musculocutaneous nerves can result from shoulder dislocation, and the sensory areas of these nerves should be examined carefully when the patient presents with a dislocation (Figure 8.85).
The suprascapular nerve may be damaged due to acromioclavicular joint separation or a ganglion cyst and this will result in pain and atrophy of the supraspinatus and infraspinatus muscles. Forced adduction of the arm across the chest worsens the pain due to stretching of the suprascapular nerve (Figure 8.86).
Damage to the upper trunk of the brachial plexus, which comprises the C5 and C6 nerve roots, leads to an Erb-Duchenne palsy of the upper extremity. This may be caused at birth by trauma due to shoulder dystocia, or may be congenital. Characteristic posture and weakness as well as sensory loss result (Figure 8.87).
181

The Shoulder Chapter 8
Table 8.1 Movements and innervation of shoulder muscles.
Movement |
Muscles |
Innervation |
Root level |
|
Forward flexion |
1 Deltoid |
Axillary |
C5, C6 |
|
|
2 |
Pectoralis major (clavicular fibers) |
Lateral pectoral |
C5, C6, C7 |
|
3 |
Coracobrachialis |
Musculocutaneous |
C6, C7 |
|
4 |
Biceps |
Musculocutaneous |
C5, C6 |
Extension |
1 |
Deltoid (posterior fibers) |
Axillary |
C5, C6 |
|
2 |
Teres major |
Subscapular |
C5, C6 |
|
3 |
Teres minor |
Axillary |
C5 |
|
4 |
Latissimus dorsi |
Thoracodorsal |
C6, C7, C8 |
|
5 |
Pectoralis major (sternocostal fibers) |
Lateral pectoral |
C5, C6, C7 |
|
|
|
Medial pectoral |
C7, C8, T1 |
|
6 |
Triceps (long head) |
Radial |
C7, C8 |
Abduction |
1 Deltoid |
Axillary |
C5, C6 |
|
|
2 |
Supraspinatus |
Suprascapular |
C5 |
|
3 |
Infraspinatus |
Suprascapular |
C5, C6 |
|
4 |
Subscapularis |
Subscapular |
C5, C6 |
|
5 |
Teres major |
Axillary |
C5 |
Adduction |
1 Pectoralis major |
Lateral pectoral |
C5, C6, C7 |
|
|
2 |
Latissimus dorsi |
Thoracodorsal |
C6, C7, C8 |
|
3 |
Teres major |
Subscapular |
C5, C6 |
|
4 |
Subscapularis |
Subscapular |
C5, C6 |
Internal (medial) rotation |
1 Pectoralis major |
Lateral pectoral |
C5, C6, C7 |
|
|
2 |
Deltoid (anterior fibers) |
Axillary |
C5, C6 |
|
3 |
Latissimus dorsi |
Thoracodorsal |
C6, C7, C8 |
|
4 |
Teres major |
Subscapular |
C5, C6 |
|
5 |
Subscapularis |
Subscapular |
C5, C6 |
External (lateral) rotation |
1 Infraspinatus |
Suprascapular |
C5, C6 |
|
|
2 |
Deltoid (posterior fibers) |
Axillary |
C5, C6 |
|
3 |
Teres minor |
Axillary |
C5 |
Elevation of scapula |
1 Trapezius (upper fibers) |
Accessory |
Cranial nerve XI |
|
|
|
|
C3, C4 nerve roots |
C3, C4 roots |
|
2 |
Levator scapulae |
C3, C4 nerve roots |
C3, C4 roots |
|
|
|
Dorsal scapular |
C5 |
|
3 |
Rhomboideus major |
Dorsal scapular |
C5 |
|
4 |
Rhomboideus minor |
Dorsal scapular |
C5 |
Retraction (backward |
1 Trapezius |
Accessory |
Cranial nerve XI |
|
movement of scapula) |
2 Rhomboid major |
Dorsal scapular |
C5 |
|
|
3 |
Rhomboideus minor |
Dorsal scapular |
C5 |
Protraction (forward |
1 Serratus anterior |
Long thoracic |
C5, C6, C7 |
|
movement of scapula) |
2 Pectoralis major |
Lateral pectoral |
C5, C6, C7 |
|
|
3 |
Pectoralis minor |
Medial pectoral |
C7, C8, T1 |
|
4 |
Latissimus dorsi |
Thoracodorsal |
C5, C6, C7 |
|
|
|
|
|
The spinal accessory nerve may be injured during surgery, and if the branch to the trapezius muscles is destroyed, the patient will present with an inability to shrug the shoulder and a lateral winging of the scapula. The scapula will move posteriorly away from the thorax, as in medial winging. However, the medial border of the scapula is set laterally away from the spinous processes by the strong serratus anterior.
Special Tests
Tests for Structural Stability and Integrity
Many tests have been devised to examine the shoulder for stability in the anterior, posterior, and inferior
182

Chapter 8 The Shoulder
C5
Key sensory area for C4
C4
C6
C7
Key sensory area for T2
C5
T2
C6
T3
T4
T6 T5
Figure 8.82 The dermatomes of the shoulder and axilla. Note the key sensory areas for the C4 and T2 dermatomes in this region.
183

The Shoulder Chapter 8
1
2
5
3
6 8
1
2
5
3
6
Anterior view
Figure 8.83 The nerve supply and distribution of the shoulder in the anterior view. 1 = supraclavicular nerve (C3, C4); 2 = upper lateral cutaneous (axillary) (C5, C6); 3 = intercostobrachial (T2); 4 = posterior cutaneous nerve of the arm (radial) (C5–C8);
5 = lower lateral cutaneous nerve (radial) (C5, C6); 6 = medial cutaneous nerve of the arm (C8, T1); 7 = posterior cutaneous nerve of the forearm (radial) (C5–C8); 8 = medial cutaneous nerve of the forearm (C8, T1).
1
2 |
|
|
|
|
5 |
3 |
4 |
7 |
|
||
|
|
6 |
1
2
5
4 3
6
7
Posterior view
Figure 8.84 The nerve supply and distribution of the shoulder in the posterior view. 1 = supraclavicular nerve (C3, C4); 2 = upper lateral cutaneous (axillary) (C5, C6); 3 = intercostobrachial (T2); 4 = posterior cutaneous nerve of the arm (radial) (C5–C8);
5 = lower lateral cutaneous nerve (radial) (C5, C6); 6 = medial cutaneous nerve of the arm (C8, T1); 7 = posterior cutaneous nerve of the forearm (radial) (C5–C8); 8 = medial cutaneous nerve of the forearm (C8, T1).
directions. There are also tests to examine the patient for multidirectional instability. All the tests are performed by applying passive forces to the glenohumeral joint in different directions. A great deal of experience is necessary to evaluate the degree of shoulder instability correctly.
Anterior Instability Test (Rockwood Test)
This test is used to evaluate the degree to which the humeral head can be anteriorly subluxed from the glenoid cavity of the scapula (Figure 8.88A–D). The patient is standing. Stand behind the patient and hold his or her arms just proximal to the wrists with your hands and laterally rotate the shoulders. Then abduct the arms to 45 degrees and again passively rotate the shoulders laterally. This same
procedure is repeated at 90 and 120 degrees. At 0 degree, there is rarely any complaint of apprehension or pain. At 45 and 120 degrees, the patient may show some signs of apprehension. The test result is positive when the patient shows marked apprehension and pain posteriorly when the arm is at 90 degrees of abduction. This is due to anterior capsular/labral insufficiency.
Rowe, Volk, Gerber and Ganz have described other tests for anterior instability.
Apprehension Test for Anterior Shoulder Dislocation (Crank Test)
The result of this test is frequently positive in patients who have had recent shoulder dislocation or are prone to recurrent shoulder dislocation. Ninety-five
184