

MusculoSkeletal Exam
.pdfradial head
Figure 9.30 Mobility testing of ventral and dorsal glide of the radial head.
the patient. Place your hand around the distal anterior aspect of the humerus to stabilize it. Place your thumb at the joint space to palpate the movement. Place your other hand at the distal end of the forearm just proximal to the wrist joint. Make sure that you are only holding the radius. Pull the radius in a longitudinal direction until you take up all the slack. This movement produces traction in the humero-radial joint (Figure 9.29).
Ventral and Dorsal Glide of the Radial Head
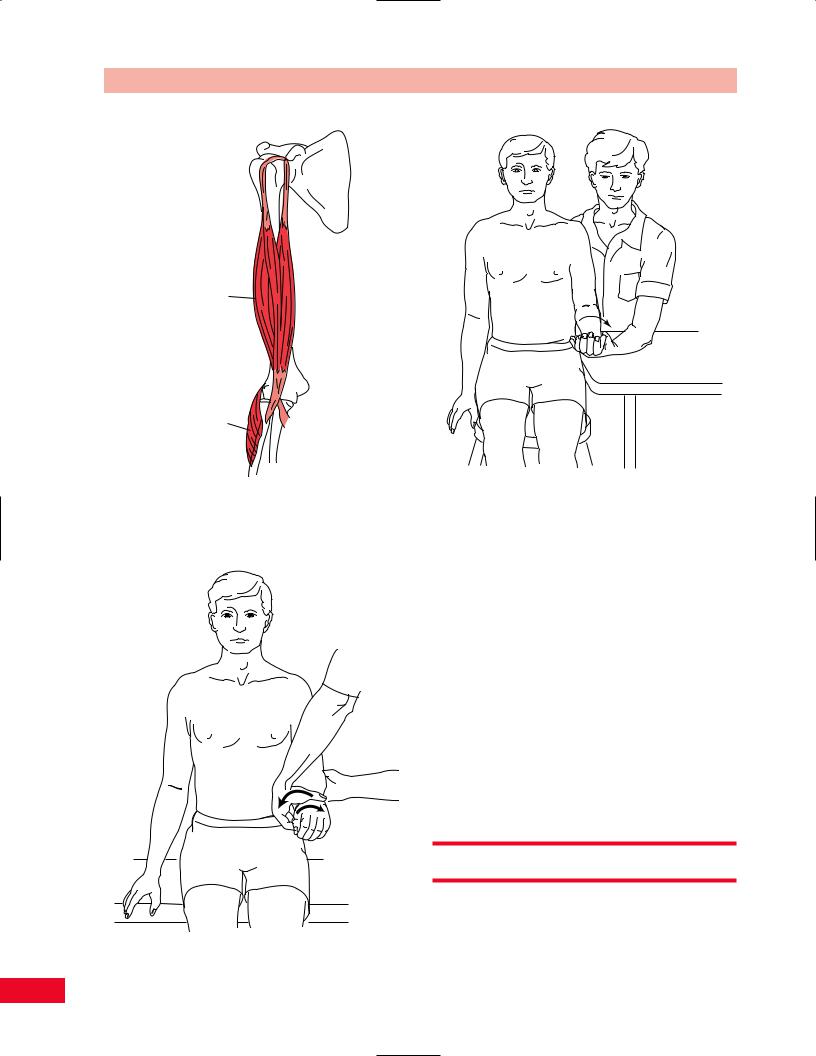
Place the patient in the seated position so that the arm is supported on the treatment table. Position the patient’s arm in the resting position. Stand so that you are facing the patient. Place one hand under the proximal dorsal aspect of the ulna to stabilize it. Place the index finger and thumb of your other hand around the radial head. Move the radial head in a ventral and then a dorsal direction until all the slack is taken up in both directions. This tests for the mobility of the proximal radio-ulnar joint (Figure 9.30).
Ventral and Dorsal Glide of the Radius
Place the patient in the seated position so that the arm is supported on the treatment table. Position the patient’s arm in the resting position. Stand so that you are facing the patient. Place one hand under the distal dorsal aspect of the ulna to stabilize it. Place the index
Chapter 9 The Elbow
Stabilize
Figure 9.31 Mobility testing of ventral and dorsal glide of the radius.
finger and thumb of your other hand around the distal end of the radius just proximal to the wrist joint. Move the radius in both a ventral and a dorsal direction until all the slack is taken up in both directions. This tests for the mobility of the distal radio-ulnar joint (Figure 9.31).
Resistive Testing
The muscles of the elbow function to position the hand in space. The motions to be tested are flexion, extension, pronation, and supination. The prime movers of the elbow joint are located in the arm.
Although the elbow is analogous to the knee in many respects, unlike the knee, the elbow usually functions as part of an open chain with the hand and wrist.
This may be why most of the flexors and extensors of the wrist and fingers also cross the elbow joint, affording more precise control of the fingers and hand in space. Note that none of the muscles of the toes cross the knee joint. The gastrocnemius is the only muscle that crosses the knee and ankle joints.
Elbow Flexion
The flexors of the elbow are the biceps brachii, the brachialis, and brachioradialis (Figure 9.32).
215

The Elbow Chapter 9
Biceps |
Brachioradialis |
brachii |
|
Brachialis |
|
Figure 9.32 The flexors of the elbow.
Figure 9.33 Testing elbow flexion.
•Position of patient: Sitting with the arm at the side. The forearm is supinated (Figure 9.33).
•Resisted test: Take the patient’s wrist with your hand and stabilize his or her upper arm with your other hand. Ask the patient to flex the elbow as you resist this motion by holding the forearm and pulling downward.
Testing elbow flexion with gravity eliminated is
performed with the patient in a supine position and the shoulder abducted to 90 degrees and externally rotated (Figure 9.34). Stabilize the upper arm as the patient attempts to slide the forearm along the table into elbow flexion through the complete range of motion.
Painful resisted elbow flexion accompanied by a large bulge in the midarm may be due to rupture of the biceps tendon.
Weakness of elbow flexion caused by damage to the musculocutaneous nerve, which innervates the biceps and brachialis muscles, will cause the patient to pronate the forearm and substitute for loss of elbow flexion by using the brachioradialis, extensor carpi radialis longus, wrist flexors, and pronator teres. Weakness of elbow flexion causes a substantial restriction in activities of daily living such as feeding and grooming.
216

Chapter 9 The Elbow
Figure 9.34 Testing elbow flexion with gravity eliminated.
Long
head of Lateral head of triceps triceps
Medial head of triceps
Figure 9.35 The elbow extensors.
Elbow Extension
The elbow extensors are the triceps brachii and anconeus muscles (Figure 9.35).
•Position of patient: Supine with the shoulder flexed to 90 degrees and the elbow flexed (Figure 9.36).
•Resisted test: Stabilize the arm with one hand just proximal to the elbow and apply a downward flexing resistive force with your other hand to the forearm just proximal to the wrist. Ask the patient to extend the elbow upward against your resistance.
Testing elbow extension with gravity eliminated
is performed with the patient supine and the shoulder abducted to 90 degrees and internally rotated (Figure 9.37).
Painful resisted elbow extension associated with a swelling over the olecranon process is likely due to olecranon bursitis.
Weakness of elbow extension causes difficulty in using a cane or crutches owing to an inability to bear weight on the extended elbow. Activities such as throwing, reaching upward toward a high object, and doing push-ups are also restricted.
Forearm Pronation
The pronators of the forearm are the pronator teres and pronator quadratus muscles (Figure 9.38).
217

The Elbow Chapter 9
Figure 9.36 Testing elbow extension.
Figure 9.37 Testing elbow extension with gravity eliminated.
218

Chapter 9 The Elbow
Pronator teres
Pronator quadratus
Figure 9.38 The forearm pronators.
Figure 9.40 Testing forearm pronation with gravity eliminated.
Figure 9.39 Testing forearm pronation.
•Position of patient: Sitting with the arm at the side and the elbow flexed to 90 degrees to prevent rotation at the shoulder. The forearm is initially supinated (Figure 9.39).
•Resisted test: Stabilize the upper arm with one hand placed just proximal to the elbow joint. With your other hand, take the patient’s forearm just proximal to the wrist and apply a rotational stress into supination as the patient attempts to pronate the forearm. Do not allow the patient to internally rotate the shoulder in an effort to increase the movement of the forearm.
Testing forearm pronation with gravity eliminated
is performed with the patient in the same position. The test is performed without resistance (Figure 9.40).
The pronator quadratus muscle can be isolated by performing the resisted test with the elbow in extreme flexion. This puts the pronator teres muscle at a mechanical disadvantage. This is useful in testing for anterior interosseous nerve syndrome (see p. 225).
Forearm Supination
The supinators of the forearm are the biceps brachii and the supinator muscles (Figure 9.41).
219
The Elbow Chapter 9
Biceps brachii
Supinator
Figure 9.43 Testing forearm supination with gravity eliminated.
Figure 9.41 The forearm supinators.
Figure 9.42 Testing forearm supination.
•Position of patient: Seated with the arm at the side and the elbow flexed to 90 degrees to prevent external rotation of the shoulder, which is used to
compensate for lack of supination range of motion. The forearm is in neutral position (Figure 9.42).
•Resisted test: Stabilize the upper arm with one hand placed above the elbow and take the patient’s forearm just proximal to the wrist. The patient attempts to supinate the forearm as you apply a rotational force into pronation to resist him or her. Testing forearm supination with gravity eliminated
is performed with the patient in the same position, but without resistance (Figure 9.43).
Painful resisted supination may be due to biceps tendinitis.
Weakness of forearm supination affects many activities of daily living, including feeding oneself and personal hygiene.
Neurological Examination
Motor
The innervation and spinal levels of the muscles that function across the elbow are listed in Table 9.1.
220
Chapter 9 The Elbow
Table 9.1 Muscles, innervation, and root levels of the elbow.
Movement |
Muscles |
Innervation |
Root levels |
|
Flexion of elbow |
1 Biceps brachii |
Musculocutaneous |
C5, C6 |
|
|
2 |
Brachialis |
Musculocutaneous |
C5, C6 |
|
3 |
Brachioradialis |
Radial |
C5, C6 |
|
4 |
Pronator teres |
Median |
C6, C7 |
|
5 |
Flexor carpi ulnaris |
Ulnar |
C7, C8, T1 |
Extension of elbow |
1 Triceps |
Radial |
C7, C8 |
|
|
2 |
Anconeus |
Radial |
C7, C8 |
Pronation of forearm |
1 Pronator teres |
Median |
C6, C7 |
|
|
2 |
Pronator quadratus |
Anterior interosseous (median) |
C8, T1 |
|
|
|
|
|
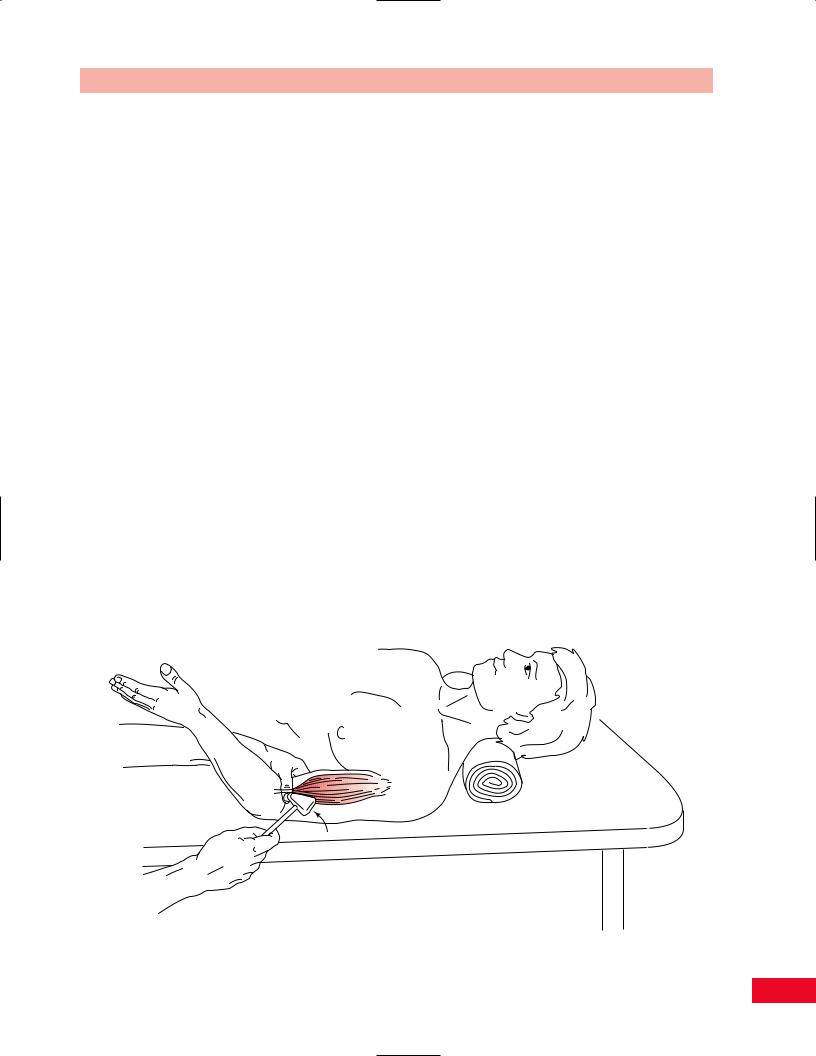
Reflexes
Biceps Reflex
The biceps reflex (Figure 9.44) is used to test the C5, and to a lesser extent, the C6 neurological levels. The test is performed by having the patient rest their forearm on your forearm as you take the patient’s elbow in your hand with your thumb pressing downward on the biceps tendon. The tendon becomes more prominent as the patient flexes the elbow slightly. Ask the patient to relax and take the reflex hammer with your other hand and tap onto your thumbnail. The biceps will contract and the arm may jump slightly. Absence of this reflex indicates damage to the C5 nerve root level, or the upper trunk or lateral cord of the brachial
plexus, musculocutaneous nerve, or biceps musculotendinous unit. Always compare to the opposite side.
Brachioradialis Reflex
The brachioradialis reflex (Figure 9.45) is used to test the C6 nerve root level. Have the patient rest their forearm over yours with the elbow in slight flexion. Use the flat end of the reflex hammer to tap the distal end of the radius. The test result is positive when the brachioradialis muscle contracts and the forearm jumps up slightly. Absence of this reflex signifies damage in the C6 nerve root level, the upper trunk or posterior cord of the brachial plexus, the radial nerve, or the brachioradialis musculotendinous unit. Always compare to the opposite side.
Figure 9.44 Testing the biceps reflex.
221

The Elbow Chapter 9
Figure 9.45 Testing the brachioradialis reflex.
Figure 9.46 Testing the triceps reflex.
222

Chapter 9 The Elbow
Key sensory area for C5
Anterior
C5
C5
Posterior |
|
Anterior |
T2 |
|
|
|
C6 |
C7
Posterior
T1 
Anterior
Key sensory area for T1
Figure 9.47 The dermatomes of the upper arm and forearm. Note the key sensory areas for C5 and T1, located laterally and medially in the antecubital fossa.
Triceps Reflex
The triceps reflex (Figure 9.46) tests the C7 nerve root level. The test is performed by having the patient’s forearm resting over yours. Hold the patient’s arm proximal to the elbow joint to stabilize the upper arm. Ask the patient to relax, and tap the triceps tendon with the reflex hammer, just proximal to the olecranon process. The test result is positive when contraction of the triceps muscle is visualized. Absence of this reflex signifies damage to the C7 nerve root or middle trunk or posterior cord of the brachial plexus, radial nerve, or triceps musculotendinous unit. Always compare your findings to the opposite side.
Sensation
Light touch and pinprick sensation should be examined after the motor and reflex examination. The dermatomes for the elbow are C5, C6, C7, C8, and T1. Peripheral nerves and their distribution in the elbow region are shown in Figures 9.47, 9.48, and 9.49.
Entrapment Neuropathies
Median Nerve
Median nerve entrapment at the elbow is much less common than at the wrist, as in carpal tunnel syndrome. The median nerve may be compressed above the elbow by an anomalous structure known as the ligament of Struthers. At and below the elbow, the median nerve may be compressed by the bicipital aponeurosis (lacertus fibrosus). It may also be compressed at the level of the pronator teres and the flexor digitorum superficialis muscles (Figure 9.50).
The anterior interosseous nerve, which is a branch of the median nerve, may be compressed in the proximal part of the forearm.
Ligament of Struthers
The ligament of Struthers is a relatively rare compression site of the median nerve. The patient usually complains of pain and parasthesias in the index or long finger. You may exacerbate the pain in this condition by having the patient extend the elbow and supinate
223

The Elbow Chapter 9
2
4
1
3 |
6 |
5
2
4
6
1
|
5 |
1. |
Intercostobrachial |
|
2. |
Upper lateral cutaneous |
|
|
|
||
3 |
|
3. |
Medial cutaneous of arm |
|
|
4. |
Lower lateral cutaneous |
|
|
5. |
Medial cutaneous of forearm |
|
|
6. |
Lateral cutaneous of forearm |
Figure 9.48 Anterior view of the sensory nerves and their distributions in the upper arm and forearm.
the forearm. In addition, you may be able to palpate a bony spur proximal to the medial epicondyle of the humerus, which is the attachment site of this anomalous ligament.
Pronator Teres Syndrome
Here, the median nerve is being compressed between the two heads of the pronator teres muscle (Figure 9.51). The other entrapment sites at the bicipital aponeurosis and flexor digitorum superficialis are usually grouped with pronator teres syndrome.
A patient with entrapment of the median nerve at the pronator teres will frequently have tenderness over the proximal portion of the pronator teres muscle.
Compression of the pronator teres for 30 seconds, resulting in parasthesias in the thumb and index fingers, is positive for pronator teres syndrome. Reproduction of symptoms of pain or parasthesias during resisted wrist flexion and pronation is also positive for pronator teres syndrome (Figure 9.52).
Reproduction of symptoms of pain or parasthesias in the proximal part of the forearm caused by resisted supination and elbow flexion (biceps muscle) is a positive sign for median nerve compression at the lacertus fibrosus (Figure 9.53).
Reproduction of the symptoms of pain or parasthesias in the forearm or hand following resisted flexion of the long finger is positive for median nerve
224