

MusculoSkeletal Exam
.pdfChapter 10 The Wrist and Hand
Abductor pollicis longus
Radial styloid process
Figure 10.80 The abductor pollicis longus. Note that the tendon rides over the radial styloid process and is often affected by tenosynovitis in de Quervain’s syndrome.
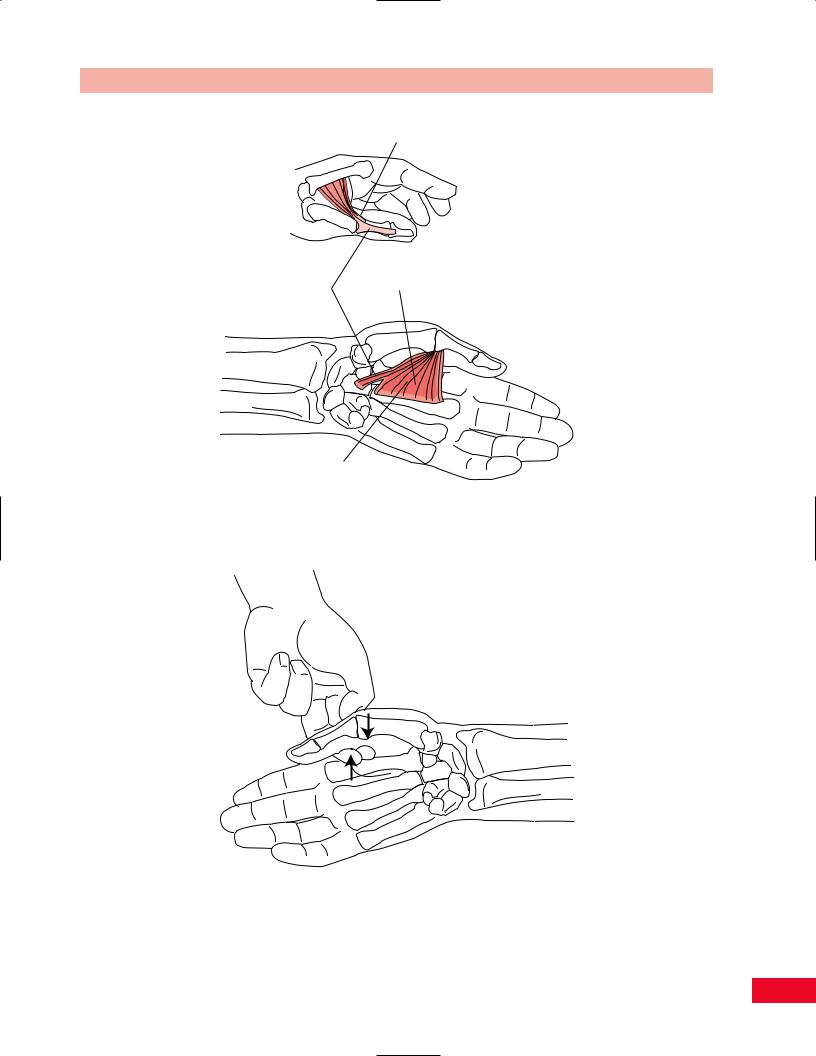
Abductor pollicis brevis
Figure 10.81 The abductor pollicis brevis.
•Position of patient: Sitting. The forearm is supinated and the wrist is in neutral.
•Resisted test: The abductor pollicis longus is tested by resisting first metacarpal abduction
with your hand, putting pressure on the palmar aspect of the first metacarpal as the patient attempts to elevate the thumb in a plane perpendicular to the hand. Support the hand and wrist from underneath with your other hand (Figure 10.82). Testing the abductor pollicis brevis is accomplished by applying pressure
to the radial aspect of the proximal phalanx of the thumb as the patient attempts to abduct
the thumb in a plane perpendicular to the hand (Figure 10.83).
Painful abduction of the first metacarpal can be due to de Quervain’s syndrome affecting the tendon of the abductor pollicis longus as it crosses the radial styloid process (see the special test for de Quervain’s syndrome on p. 284).
Weakness of thumb abduction results in the patient’s inability to grasp a large object, as the thumb cannot be moved away from the hand. Weakness of the abductor pollicis brevis is seen in advanced cases of carpal tunnel syndrome.
Adduction
Thumb adduction is accomplished by the adductor pollicis muscle (Figure 10.84). This muscle is assisted by the deep head of the flexor pollicis brevis. Both of these muscles are innervated by the ulnar nerve.
275

The Wrist and Hand Chapter 10
Figure 10.82 Testing abduction of the carpometacarpal joint of the thumb.
Figure 10.83 Testing abduction of the metacarpophalangeal joint of the thumb. The abductor pollicis brevis is weak in patients with carpal tunnel syndrome.
•Position of patient: Sitting.
•Resisted test: Place your index and long fingers in the patient’s first web space. Ask the patient to press your fingers into his or her palm with the thumb. Try to pull the patient’s thumb upward into abduction in a plane perpendicular to his or her palm (Figure 10.85).
Weakness of thumb adduction prevents the patient
from making a strong clenched fist.
To test for Froment’s sign, ask the patient to hold a piece of paper between the thumb and the radial aspect of the index finger. Try to pull the paper away from the patient and if the adductor pollicis is weak, the patient will flex the thumb interphalangeal joint as a compensatory measure as he or she attempts to compensate with the flexor pollicis longus for a weak adductor pollicis (Figure 10.86).
276
Chapter 10 The Wrist and Hand
Transverse head
Transverse Oblique head
head
Adductor pollicis
Figure 10.84 The adductor pollicis.
Figure 10.85 Testing adduction of the thumb.
277

The Wrist and Hand Chapter 10
normal |
abnormal |
Figure 10.86 Froment’s sign. The patient will flex the interphalangeal joint of the thumb to compensate for weakness of the adductor pollicis seen in ulnar nerve injury.
Opposition of the Thumb and Fifth Finger
The muscles responsible for opposition are the opponens pollicis and opponens digiti minimi (Figure 10.87). They are innervated by the median and ulnar nerves, respectively.
•Position of patient: Sitting.
•Resisted test: The patient attempts to bring the palmar surfaces of the tips of the thumb and fifth finger together. Apply resistance against the anterior aspect of the first and fifth metacarpals so
|
Opponens |
|
Opponens |
digiti |
|
minimi |
||
pollicis |
||
|
Figure 10.87 The opponens pollicis and the opponens digiti minimi muscles.
Figure 10.88 Testing opposition of the thumb and fifth finger.
278

as to pry them apart (Figure 10.88). The muscles can be tested separately to note their individual strengths. Note that the patient can attempt to flex the thumb with the flexor pollicis longus and brevis in the plane of the palm. Opposition occurs with the thumb away from the palm.
Weakness of opposition of the thumb and fifth finger results in the inability to hold a pencil and grasp objects firmly.
Chapter 10 The Wrist and Hand
Neurological Examination
Motor
The innervation and spinal levels of the muscles that function across the wrist and hand are outlined in Table 10.1.
Table 10.1 Muscle, innervation, and root levels of the hand and wrist.
Movement |
Muscles |
Innervation |
Root levels |
|
Flexion of wrist |
1 Flexor carpi radialis |
Median |
C6, C7 |
|
|
2 |
Flexor carpi ulnaris |
Ulnar |
C8, T1 |
Extension of wrist |
1 Extensor carpi radialis longus |
Radial |
C6, C7 |
|
|
2 |
Extensor carpi radialis brevis |
Posterior interosseous (radial) |
C6, C7 (radial) |
|
3 |
Extensor carpi ulnaris |
Posterior interosseous (radial) |
C6, C7, C8 |
Flexion of fingers |
1 Flexor digitorum profundus |
Anterior interosseous profundus |
C8, T1 |
|
|
|
|
(median): lateral two digits |
|
|
|
|
Ulnar: medial two digits |
C8, T1 |
|
2 |
Flexor digitorum sublimis |
Median |
C7, C8, T1 |
|
3 |
Lumbricals |
First and second: median; |
C7, C8, T1 |
|
|
|
Third and fourth: ulnar |
C8, T1 |
|
|
|
(deep terminal branch) |
|
|
4 |
Interossei |
Ulnar (deep terminal branch) |
C8, T1 |
|
5 |
Flexor digiti minimi |
Ulnar (deep terminal branch) little finger |
C8, T1 |
Extension of fingers |
1 Extensor digitorum communis |
Posterior interosseous (radial) |
C6, C7, C8 |
|
|
2 |
Extensor indicis (second finger) |
Posterior interosseous (radial) |
C7, C8 |
|
3 |
Extensor digiti minimi (little finger) |
Posterior interosseous (radial) |
C6, C7, C8 |
Abduction of fingers |
1 Dorsal interossei |
Ulnar (deep terminal branch) |
C8, T1 |
|
(with fingers extended) |
2 Abductor digiti minimi (little finger) |
Ulnar (deep terminal branch) |
C8, T1 |
|
Adduction of fingers |
Palmar interossei |
Ulnar (deep terminal branch) |
C8, T1 |
|
(with fingers extended) |
|
|
|
|
Flexion of thumb |
1 Flexor pollicis brevis |
Superficial head: median |
C8, T1 |
|
|
|
|
(lateral terminal branch) |
|
|
|
|
Deep head: ulnar |
C8, T1 |
|
2 |
Flexor pollicis longus |
Anterior interosseous (median) |
C8, T1 |
|
3 |
Opponens pollicis |
Median (lateral terminal branch) |
C8, T1 |
Extension of thumb |
1 |
Extensor pollicis longus |
Posterior interosseous (radial) |
C6, C7, C8 |
|
2 |
Extensor pollicis brevis |
Posterior interosseous (radial) |
C6, C7 |
|
3 |
Abductor pollicis longus |
Posterior interosseous (radial) |
C6, C7 |
Abduction of thumb |
1 |
Abductor pollicis longus |
Posterior interosseous (radial) |
C6, C7 |
|
2 |
Abductor pollicis brevis |
Median (lateral terminal branch) |
C6, C7, C8 |
Adduction of thumb |
Adductor pollicis |
Ulnar (deep terminal branch) |
C8, T1 |
|
Opposition of thumb |
1 Opponens pollicis |
Median (lateral terminal branch) |
C8, T1 |
|
and little finger |
2 Flexor pollicis brevis |
Superficial head: median |
C8, T1 |
|
|
|
|
(lateral terminal branch) |
|
|
3 |
Abductor pollicis brevis |
Median (lateral terminal branch) |
C6, C7, C8 |
|
4 |
Opponens digiti minimi |
Ulnar (deep terminal branch) |
C8, T1 |
|
|
|
|
|
279

The Wrist and Hand Chapter 10
( ) Key sensory areas
) Key sensory areas
and 10.91. Note the key sensory areas for the C6, C7, and C8 dermatomes.
Entrapment Neuropathies
C6 |
C6 |
|
C7 |
C7 |
C8 |
C8 |
|
|
Posterior |
Anterior |
Median Nerve
Entrapment of the median nerve within the carpal tunnel is extremely common (Figure 10.92). A variety of primary conditions are associated with carpal tunnel syndrome (Table 10.2). The definitive diagnosis of carpal tunnel syndrome is made with electrodiagnostic studies. Pain or numbness of the thumb, index and middle fingers, as well as thenar atrophy may be noted in the patient with carpal tunnel syndrome.
Various tests have been used to diagnose carpal tunnel syndrome on physical examination. They include Tinel’s test, the tourniquet test, and Phalen’s test.
Figure 10.89 The dermatomes of the hand and wrist. Note the key sensory areas for C6, C7, and C8 at the interphalangeal joints of the thumb and the long and fifth fingers, respectively.
Sensation
Light touch and pinprick sensation should be checked in the wrist and hand after the motor examination. The dermatomes for the hand are C6, C7, and C8 (Figure 10.89). Peripheral nerves and their distributions in the wrist and hand are shown in Figures 10.90
Tinel’s Test
This test is performed by tapping over the median nerve, which is located just medial to the flexor carpi radialis tendon at the most proximal aspect of the palm (Figure 10.93). The test result is positive when the patient reports pain or tingling in the first three digits.
Tourniquet Test
This test attempts to exacerbate the median neuropathy in the carpal tunnel by causing temporary ischemia. A
Palmar branch |
Superficial |
|
radial nerve |
||
median nerve |
||
C6, C7, C8 |
||
|
Palmer branch, ulnar nerve
Ulnar nerve
C7, C8
Median nerve
C6, C7
Anterior view
Figure 10.90 The anterior view of the wrist and hand shows the peripheral nerves and their respective territories.
280

Chapter 10 The Wrist and Hand
Superficial |
Superficial |
radial nerve |
radial nerve |
C6, C7, C8 |
C6, C7, C8 |
Dorsal
cutaneous branch, ulnar nerve
Ulnar nerve C7, C8
Posterior view
Median nerve |
Median nerve |
|
C6, C7 |
||
C6, C7 |
||
|
Figure 10.91
Pisiform
Hook of hamate
The posterior view of the wrist and hand shows the peripheral nerves and their respective territories.
|
|
Median nerve |
|
Scaphoid |
|
Ulnar A & N |
|
tuberosity |
Transverse carpal |
||
|
ligament |
Palmaris |
|
|
longus |
||
|
Tubercle of |
||
Tubercle of |
|
||
trapezium |
Pisiform |
||
trapezium |
|||
|
|
||
|
|
Flexor |
|
Carpal tunnel |
|
digitorum |
|
|
superficialis |
||
|
|
||
|
Flexor |
Flexor |
|
|
digitorum |
||
|
pollicis |
||
|
profundus |
||
|
longus |
||
|
Trapezium |
Triquetrum |
|
|
|
Capitate |
|
|
|
Lunate |
|
|
Trapezoid |
||
Figure 10.92 The carpal tunnel and its contents. The roof of the tunnel is formed by the transverse carpal ligament. The flexor tendons of all five fingers and the flexor carpi radialis are located within the carpal tunnel, along with the median nerve. Note that the tunnel is located at the proximal palm and not under the creases of the wrist.
281

The Wrist and Hand Chapter 10
Table 10.2 Disorders associated with carpal tunnel syndrome.
Trauma
Wrist fracture (Colles’ fracture, scaphoid fracture, etc.) Wrist contusion or hematoma
Endocrine disorders
Hypothyroidism
Pregnancy
Diabetes mellitus
Menopause
Obesity
Inflammation
Tenosynovitis
Others
Gout
Ganglion cysts
Osteoarthritis of the carpal bones
Generalized edema from any cause
blood pressure cuff is inflated proximal to the elbow, about where you would take measurements for systolic pressure. The test result is positive if the patient notes numbness or tingling in the distribution of the median nerve within 60 seconds. This test produces a high rate of false-positive results.
Phalen’s Test
This test makes use of the fact that the carpal tunnel narrows in a position of increased wrist flexion. The patient is asked to flex both of the wrists against one another. The test result is positive if the patient notes parasthesias or numbness in the thumb, index, or middle fingers after holding this position for 60 seconds or less (Figure 10.94). This test has the fewest falsenegative results.
Ulnar Nerve
The ulnar nerve gives off a dorsal cutaneous branch approximately 8 cm proximal to the wrist (Figure 10.95). This branch has no motor function.
The ulnar nerve continues into the wrist through Guyon’s canal (Figure 10.96). There are two motor branches of the ulnar nerve in the hand and one sensory branch to the palmar aspect of the medial hand.
Dorsal Cutaneous Ulnar Nerve Entrapment
This sensory branch of the ulnar nerve may be injured by a fracture of the ulna, a ganglion cyst, or an ulnar artery aneurysm. Loss of sensation on the dorsal
Figure 10.93 Testing Tinel’s sign at the wrist for carpal tunnel syndrome.
282

Figure 10.94 Phalen’s test. This position is held for at least 60 seconds.
Dorsal ulnar cutaneous nerve
Ulnar nerve
Guyon canal
Deep ulnar motor branch
Figure 10.95 The ulnar nerve and its branches.
Chapter 10 The Wrist and Hand
Ulnar nerve
Pisohamate ligament
Pisiform
Hamate
Ulnar nerve
Pisohamate ligament
Pisiform
Hamate
Figure 10.96 The anatomy of Guyon’s canal. the ulnar nerve enters the wrist through this canal. It gives off a superficial sensory branch and a deep motor branch. Three types of lesions are possible at Guyon’s canal. The trunk may be affected, the sensory branch may be affected, or the deep motor branch may be affected. These lesions can occur simultaneously.
Injury to the ulnar nerve at Guyon’s canal can result from pressure due to crutch walking, pressure from bicycle handlebars, or a pneumatic drill.
medial aspect of the hand will be noted. Hand function will otherwise be normal.
Ulnar Nerve Compression at Guyon’s Canal
Compression of the ulnar nerve in Guyon’s canal (see Figure 10.96) most often results from a ganglion, but can also occur with rheumatoid arthritis or trauma. The findings on examination include weakness of the ulnar-innervated intrinsic hand muscles, which include the interossei and the medial two lumbricals. If the superficial sensory branch to the fourth and fifth digits is involved, decreased sensation will be noted on the palmar aspect of these fingers. A characteristic posture of the hand known as a benediction deformity (Figure 10.97) results from ulnar nerve damage at Guyon’s canal, affecting both the hypothenar and intrinsic muscles.
Damage to the median and ulnar nerves at the wrist, which occurs most commonly with trauma, results in a deformity known as a claw hand (Figure 10.98). This is also referred to as an intrinsic minus hand.
283

The Wrist and Hand Chapter 10
Pain here in radial styloid
Extensor pollicis brevis
Abductor pollicis longus
Figure 10.97 The benediction hand deformity results from damage to the ulnar nerve. There is wasting of the interosseous muscles, the hypothenar muscles, and the two medial lumbrical muscles.
Figure 10.99 Finkelstein’s test is used to diagnose tenosynovitis of the first dorsal compartment of the wrist, which includes the extensor pollicis brevis and abductor pollicis longus muscles.
Special Tests
Finkelstein’s Test (de Quervain’s
Syndrome)
This test is used to diagnose tenosynovitis of the first dorsal compartment of the wrist, which contains the tendons of the abductor pollicis longus and extensor pollicis brevis muscles (Figure 10.99). Pain and swelling are usually present over the radial styloid process. A ganglion cyst may be noted. Finkelstein’s test is performed by having the patient place the thumb inside the closed fist. Take the patient’s hand and deviate the hand and wrist in the ulnar direction to stretch the tendons of the first extensor compartment.
Figure 10.98 (left) The claw hand deformity results from loss of intrinsic muscles with overactivity of the extensor digitorum, causing hyperextension of the metacarpophalangeal joints. This is most often caused by combined damage to the median and ulnar nerves at the wrist.
284