

Part seven. Dorsum of the foot
The skin of the dorsum of the foot is supplied mainly by the superficial peroneal nerve, assisted by the deep peroneal, saphenous, and sural nerves (Fig. 3.46). The large veins form a dorsal venous arch which receives most of its blood by marginal and interosseous tributaries from the sole of the foot. The dorsal venous arch, lying over the heads of the metatarsals, drains from its medial and lateral ends into the great and small saphenous veins respectively.
The superficial peroneal (superficial fibular) nerve becomes subcutaneous in the distal third of the leg and divides into medial and lateral branches which supply the skin of the dorsum of the foot. The medial branch further divides to supply the medial side of the dorsum of the great toe and the sides of the second cleft. The lateral branch divides to supply the third and fourth clefts. The lateral side of the foot and lateral side of the little toe are supplied by the sural nerve, while the first cleft is supplied by the deep peroneal nerve. The skin over the terminal phalanges is supplied by the medial and lateral plantar nerves. The medial side of the foot, usually as far forward as the first metatarsophalangeal joint, is supplied by the termination of the saphenous nerve.
The subcutaneous layer of the dorsum of the foot, as of the hand, contains little fat in most people, and the veins are consequently easily seen when distended.
The deep fascia on the dorsum of the foot binds down the underlying tendons. A Y-shaped thickening of the fascia, the inferior extensor retinaculum, prevents bowstringing of the extensor tendons as they pass across the front of the ankle joint.
The inferior extensor retinaculum arises by a stem from the anterior part of the upper surface of the calcaneus, on the lateral border of the dorsum of the foot (Fig. 3.32). From the stem two limbs diverge. The upper limb is attached to the medial malleolus, the lower limb arches across the tendons on the dorsum and blends with the plantar aponeurosis under the medial longitudinal arch of the foot. Most of the inferior retinacular fibres, however, sling around the tendons and return to be attached to the calcaneus, and only the superficial fibres pass across to the medial malleolus and plantar aponeurosis. All the extensor tendons are enclosed in synovial sheaths where they are slung in the inferior extensor retinaculum.
Extensor digitorum brevis
This is a muscle whose fleshy belly can be seen in most feet and felt in all. It arises from the upper surface of the calcaneus and from the deep surface of the stem of the Y-shaped inferior extensor retinaculum. It passes obliquely across the dorsum of the foot and gives off four tendons to the medial four toes. The tendon to the great toe is different from the others and is named extensor hallucis brevis. Its belly usually separates early from the main muscle mass and the tendon is inserted separately into the base of the proximal phalanx of the great toe. As in the thumb, so in the great toe there is no dorsal extensor expansion. The remaining three tendons are inserted into the dorsal extensor expansions of the second, third and fourth toes. All four tendons of the muscle pass deep to the tendons of extensor digitorum longus.
Nerve supply. By the deep peroneal nerve (S1, 2).
Action. To extend the medial four toes. It is particularly of value when the long extensor is out of
action, in the fully dorsiflexed ankle.
Test. The toes are dorsiflexed and the muscle belly is observed and palpated towards the lateral side of the dorsum of the foot.
The anterior tibial artery, lying over the lower end of the tibia midway between the malleoli, extends forwards as the dorsalis pedis artery (Fig. 3.32). This runs to the base of the first intermetatarsal space and passes down into the sole, where it joins the lateral plantar artery to complete the plantar arch. It lies between the tendon of extensor hallucis longus medially and the digital branch of the deep peroneal nerve laterally, and it is crossed by the tendon of extensor hallucis brevis. Its pulsation can be palpated lateral to the extensor hallucis longus tendon on a line from the midpoint between the two malleoli towards the first toe cleft, on the underlying navicular and intermediate cuneiform bones. Occasionally the vessel is replaced by an enlarged perforating peroneal artery, anastomosing with the lateral malleolar branch of the anterior tibial artery. It has three named branches. The lateral tarsal artery runs laterally beneath extensor digitorum brevis to supply that muscle and the underlying tarsal bones; a smaller medial tarsal artery passes to the medial border of the foot. The arcuate artery runs laterally beneath the tendons of extensor digitorum brevis over the bases of the metatarsal bones. It gives off dorsal metatarsal arteries which supply digital branches to the lateral three clefts. Each metatarsal artery gives off a perforating branch at the posterior and anterior end of its intermetatarsal space to communicate with the plantar arch and its metatarsal branches. It is the accompanying perforating veins that are responsible for bringing much of the blood from the sole of the foot through the intermetatarsal spaces to the dorsal venous arch. The first dorsal metatarsal artery, given off just before the dorsalis pedis enters the sole, supplies the first cleft and the medial side of the dorsum of the great toe.
The deep peroneal (deep fibular) nerve crosses the tibia lateral to the artery, midway between the malleoli. It passes forward, deep to the tendons, on the lateral side of the dorsalis pedis artery, to pierce the deep fascia and supply the first cleft. It gives off a branch which curves laterally beneath the muscle belly of extensor digitorum brevis supplying this muscle and the underlying periosteum and joint capsules. It also gives a branch as an additional supply to the first dorsal interosseous muscle.
Part eight. Lateral compartment of the leg
This muscular compartment lies between the peroneal surface of the fibula and deep fascia of the leg and is bounded in front and behind by the anterior and posterior intermuscular septa. It contains the peroneus longus and brevis muscles and the superficial peroneal nerve. Its blood supply is derived from branches of the peroneal artery which pierce flexor hallucis longus and the posterior intermuscular septum. Its veins drain, for the most part, into the small saphenous vein.
Peroneus longus and peroneus brevis
Peroneus (fibularis) longus arises from the head and the upper two-thirds of the peroneal surface of the fibula and from the intermuscular septa. Peroneus (fibularis) brevis arises from the lower twothirds of the fibula; in the middle third of the bone its origin lies in front of that of peroneus longus and the two muscles, and their tendons maintain this relationship.
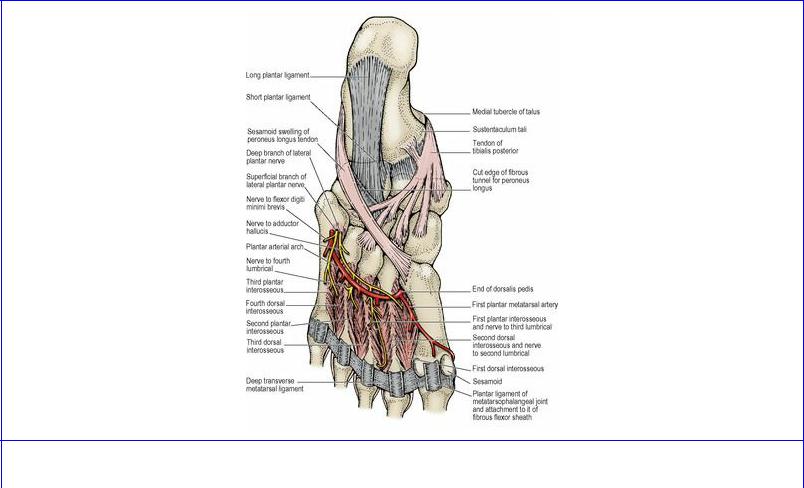
The broad tendon of peroneus brevis lies behind (and grooves) the lateral malleolus. The narrower tendon of peroneus longus lies on that of brevis and does not come into contact with the malleolus. The two tendons pass forwards to the peroneal trochlea on the lateral surface of the calcaneus, which separates them. The tendon of brevis passes above the peroneal trochlea to be inserted into the tubercle at the base of the fifth metatarsal bone. The tendon of peroneus longus passes below the peroneal trochlea and enters the sole of the foot, lying against the posterior ridge of the groove on the cuboid bone. Here the tendon possesses a sesamoid fibrocartilage which often ossifies. The tendon crosses the sole obliquely to be inserted into the lateral side of the base of the first metatarsal and the adjoining part of the medial cuneiform (Fig. 3.38).
Figure 3.38 Plantar muscles and tendons of left foot: fourth layer.
The tendons are bound down at the lateral malleolus by the superior peroneal retinaculum, a band of deep fascia that extends from the back of the malleolus to the lateral surface of the calcaneus; and at the peroneal trochlea by the inferior peroneal retinaculum, a band of fascia attached to the peroneal trochlea and to the calcaneus above and below the peroneal tendons. Its upper part is continuous with the stem of the Y-shaped inferior extensor retinaculum. The two tendons are enclosed in a common synovial sheath from above the lateral malleolus to the peroneal trochlea, where the sheath divides to accompany each tendon separately to its insertion.
Nerve supplies. Both muscles are supplied by the superficial peroneal nerve (L5, S1).
Action. Both muscles evert, and weakly plantarflex, the foot; they are the plantarflexors when the tibial nerve is paralysed. In addition, peroneus longus is a factor in maintaining the lateral longitudinal and transverse arches of the foot (see p. 161).
Test. The foot is everted and the tendons can be seen and felt below the lateral malleolus.
The superficial peroneal (superficial fibular) nerve begins in the substance of peroneus longus at the division of the common peroneal nerve. It passes downwards in the muscle and emerges at its anterior border behind the anterior intermuscular septum. It supplies both peronei, pierces the deep fascia between the middle and lower third of the leg, and divides into medial and lateral branches. (The distribution on the dorsum of the foot has been described on page 145.) It also supplies the skin of the anterolateral aspect of the lower leg (Fig. 3.46).