

|
7.4 Surgica Approac h t Thir d Mola |
91 |
|
|
|
7.3 Radiographic |
Assessment of Inferior Alveolar Nerve Risk |
|
A panoramic radiograph is the minimum requirement for radiographic assessment of third molars. There are two reasons for this. First, a whole-of-mouth approach is required when determining the role of third molar extractions as part of an overall treatment plan. Second, the relationships of the third molars to their surrounding structures is best represented on a panoramic radiograph rather than on intraoral radiographs, which may be difficult to obtain in the most posterior areas of the oral cavity.
The assessment of a panoramic radiographic begins with a systematic and thorough examination of the whole radiograph for other incidental pathologic findings. Next, attention is paid to the wisdom teeth themselves, noting the size, location, type of impaction, root formation, presence of associated pathology (e.g. odontogenic cysts or tumours, periodontal pathology, or dental caries), and relationship to surrounding structures.
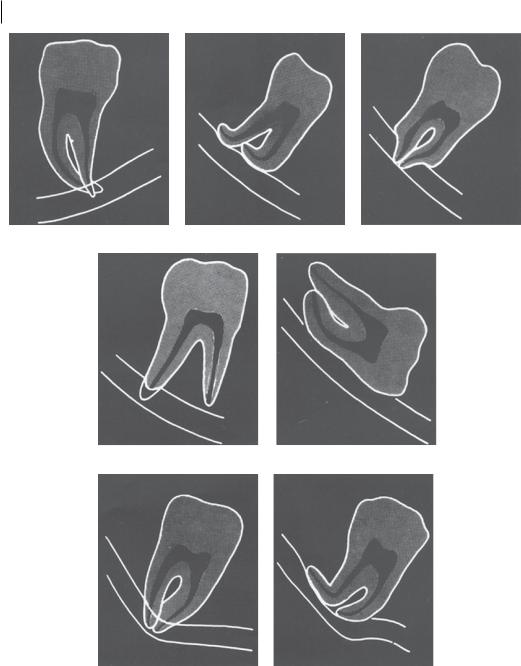
Of particular importance to mandibular third molars is the relationship of the roots to the inferior alveolar nerve. Damage to the inferior alveolar nerve can cause temporary or permanent anaesthesia, paraesthesia, or dysaesthesia, all of which may be extremely unpleasant for the patient and contribute to long-term morbidity. As such, avoidance of nerve injury during wisdom tooth extraction is of critical importance. There are seven radiographic signs that may be associated with injury to the inferior alveolar nerve, three of them (in bold) significantly so (Figure 7.2):
1)Darkening of the root
2)Deflection of the root
3)Narrowing of the root
4)Bifid root apex
5)Interruption of the ‘white line’ of the canal
6)Diversion of the canal
7)Narrowing of the canal
Importantly, inferior alveolar nerve injury may still occur even in the absence of these signs. However, the presence of any of them warrants additional radiographic investigation with CBCT and referral to a specialist oral and maxillofacial surgeon for further management.
7.4 Surgical Approach to Third Molars
In any approach to third molar extractions, the basic equipment required, final check, and local anaesthetic techniques are all largely the same as for other mandibular molar surgical extractions. For maxillary third molars, buccal and palatal infiltration anaesthetic is required to produce sufficient anaesthesia for extraction. For mandibular third molars, inferior alveolar nerve block, lingual nerve block, and buccal infiltration are required.
7.4.1 MaxillaryThird Molars
7.4.1.1 Erupted
Despite full crown eruption, maxillary third molars are usually indicated for extraction due to buccal or lingual positioning of the tooth, as a result of inadequate space. Maxillary third molars have a variable crown size and root configuration, which must be factored into the method of removal. Generally speaking, the approach to erupted maxillary third molars should mimic that to removal of a maxillary second molar; in situations where surgical extraction may be indicated (e.g. unfavourable root configuration), the principles of surgical extraction should be applied.
https://t.me/DentalBooksWorld
92 7 Third Molar Surgery
1–Darkening of root. |
2–Deflection of root. |
3–Narrowing of root. |
4–Dark and bifid apex of root. 5–Interruption of white line of canal.
6–Diversion of canal. |
7–Narrowing of canal. |
Figure 7.2 Radiographic signs that may be associated with an increased risk of damage to the inferior alveolar nerve during third molar extraction.Source: J.P.Rood,B.A.A.Nooraldeen Shehab,The radiological prediction of inferior alveolar nerve injury during third molar surgery,British Journal of Oral and Maxillofacial Surgery,Volume 28,Issue 1,1990,Pages 20–25.https://doi.org/10.1016/0266-4356(90)90005-6. Reprinted by permission from Elsevier.
7.4.1.2 Unerupted/Partially Erupted
The surgical approach to teeth in this category begins with adequate soft tissue exposure. A crestal incision with distal relieving arm, or alternatively an East Grinstead slash, is used to expose the crown of the tooth. It is rare to require bone removal, even in partly developed maxillary third
https://t.me/DentalBooksWorld