

44 3 Basic Surgical Instruments
3.4 Ancillary Soft Tissue Instruments
The process of dental extraction often involves more than just tooth removal. Prior to removal, manipulation of the soft tissues may be necessary to gain sufficient access before elevators or forceps can be applied to a tooth. Following removal, there may be debris or pathology within the socket that requires debridement or removal to ensure satisfactory postoperative healing.
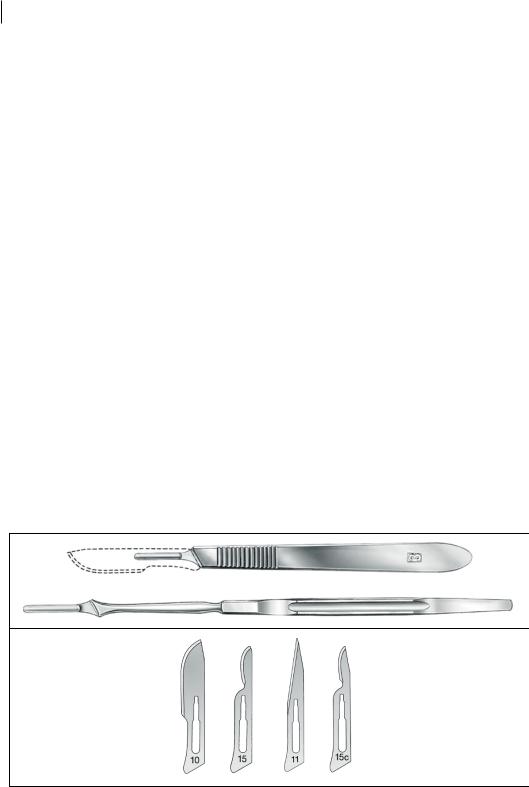
The scalpel is the main instrument used to cut the fine periodontal soft tissues of the oral cavity (Figure 3.7). A key consideration in the selection of cutting instruments for use in the oral cavity is the need to maintain control over them, as larger instruments may cause damage to the surrounding perioral tissues such as the lips and cheeks. Whilst a large variety of scalpel handle and blade configurations are available, a No. 3 or No. 7 handle with a 15 blade affords good instrument control and safe application in the mouth.
A periosteal elevator is used to lift a mucoperiosteal flap off the bone, either to facilitate access to the subgingival root of the tooth or to visualise the alveolar bone prior to removal. Whilst many designs are available, the Molt elevator is the most versatile for use in the oral cavity (Figure 3.8). It is designed with one sharp, pointed end and one flat, curved, ‘beaver-tail’ end, and is useful for elevating crestal gingiva.
The Mitchell’s trimmer was historically intended as a crown-preparation instrument in dentistry, but now is more commonly used in minor oral surgery as an instrument of soft tissue curettage (Figure 3.9). It is a double-ended instrument on a shank; one end is spoon-shaped, and is small enough to enucleate periapical cysts or remove debris from a tooth socket, whilst the other is a tapered, right-angled point, and can be used for curettage or for removal of sharp alveolar bone edges.
An angled curette is a common, double-ended surgical instrument with two curettes at opposite angles to one another which can be used in a similar fashion as a Mitchell’s trimmer to debride sockets or enucleate periapical cysts (Figure 3.10). Angled curettes are relatively unlikely to be found in a basic dentoalveolar set, as their function is largely met by the Mitchell’s trimmer.
A cleoid-discoid carver is another instrument of restorative dentistry that has become a feature of dentoalveolar surgical setups (Figure 3.11). This fine, double-ended instrument has a
Figure 3.7 Scalpel handle and blade types commonly used in dentoalveolar surgery. Source: KLS Martin.
https://t.me/DentalBooksWorld

Figure 3.8 Molt periosteal elevator. Each end has two surfaces: one rounded and one relatively flat. The round surface should be directed towards the soft tissue, whilst the flat, sharp surface should be directed towards the alveolar bone. The pointed end can be used to retract the interdental papilla, which makes raising a full-thickness mucoperiosteal flap much easier and limits tearing of the flap due to cleavage in a supraperiosteal plane. Source: KLS Martin.
3,4 mm
1,6 mm
Figure 3.9 Mitchell’s trimmer. Source: Laurence Jordan, Francois Bronnec, Pierre Machtou. https://t.me/DentalBooksWorld

46 3 Basic Surgical Instruments
Figure 3.10 Angled curette. Source: KLS Martin.
leaf-shaped (‘cleoid’) element and a disc-shaped (‘discoid’) element. It is ideal for access to and debridement of the restricted apical areas of the tooth socket, where other curettage instruments may be too large.
Curved artery forceps are an all-purpose grasping instrument, used to remove loose bone or tooth fragments from a socket (Figure 3.12). The end of the instrument is blunt and curved, with a serrated working surface.
https://t.me/DentalBooksWorld
3.5 Suturing Instruments 47
Figure 3.11 Cleoid-discoid carver. Source: KLS Martin.
3.5Suturing Instruments
During removal of a tooth, the soft tissues may be intentionally or inadvertently compromised. Instruments for the manipulation and suturing of soft tissues thus form an important part of a basic oral surgical setup (Figure 3.13). This is a very common requirement after extraction of multiple teeth or surgical extraction, or in medically compromised patients where good wound closure or haemostasis is critical.
https://t.me/DentalBooksWorld

Figure 3.12 Curved artery forceps. Source: KLS Martin.
Figure 3.13 Basic suturing equipment. Needle holders, forceps, and scissors come in a variety of sizes. As dentoalveolar surgery is carried out in the confines of the patient’s mouth, larger instruments make it more difficult to access the posterior aspects. Small needle holders with a fine tip offer good manoeuvrability and control of the soft tissues. Source: KLS Martin.
https://t.me/DentalBooksWorld