

Ghai Essential Pediatrics8th
.pdf
|
|
|
Disorders of Cardiovascular System - |
|
STAGE 1: |
"A.----+ |
|
|
|
Immune recogniti;nv v |
GAS pharyngitis |
|
|
|
|
"Rheumatogenic |
ANTIGEN? |
||
STAGE 2: |
GAS" |
t |
||
|
SKIN? |
/ 1 IL-2, TNF-a, others |
||
Immune cell circulation |
||||
Cytokine release |
|
|
|
|
STAGE 3: Antibody attachment
STAGE 4:
T cell recruitment CD4 and Cd8 infiltration
STAGE 5: Neoascularization T cell recruitment
'VJ
1 VCAM-1
l Th1 cells 7INF-y, TNF-a
Epitope spreading
IMMUNE
MECHANISM?
T cells respond to other cardiac a-helical proteins including tropomyosin and vimentin
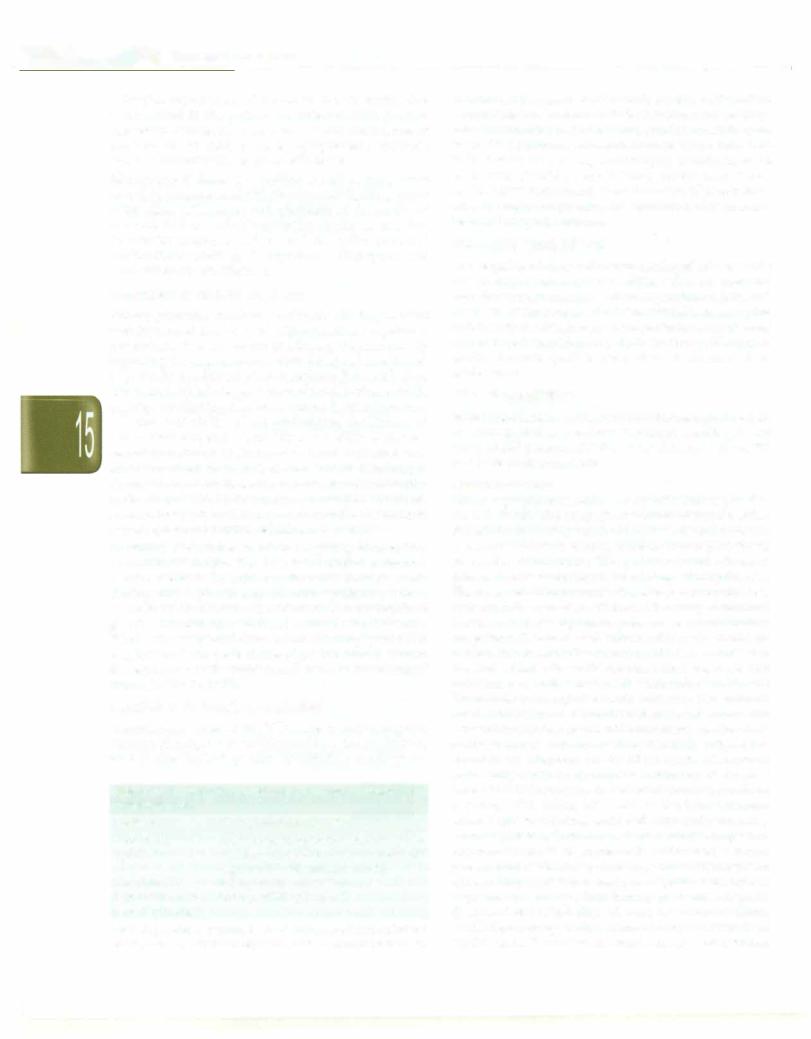
Fig. 15.40: Presumed pathogenesis of rheumatic fever; It is likely that the endothelium suffers initial damage due to a humoral immune response, the damage resulting in vascular cell adhesion molecule 1 (VCANl-1) being expressed on the endothelium. This is followed by activation of cellular immune response. As a result CD4+, CD8+ T lymphocytes and macrophages get attached to the valvar endothelium and migrate to the connective tissue core. This sets up an inflammatory response. The inflammation is accompanied by neovascularization of the valve substance. GAS group A streptococcus, INF-y gamma Interferon, TNF-a tumor necrosis factor alpha, Th1 T helper cells 1
Table 15.16: WHO criteria for diagnosis of rheumatic fever (RF) and rheumatic heart disease (based on the revised Jones criteria)
Major manifestations: Carditis, polyarthritis, chorea, erythema marginatum, subcutaneous nodules
Minor manifestations: Clinical (fever, polyarthralgia); Laboratory (elevated erythrocyte sedimentation rate, leukocyte count), Electrocardiogram (prolonged P-R interval)
Supporting evidence of preceding streptococcal infection within last 45 days: Elevated or rising antistreptolysin O or other streptococcal; antibody, or a positive throat culture, or rapid antigen test for group A streptococci, or recent scarlet fever
Priman; episode of RF: Two major or one major and two minor manifestations plus evidence of a preceding group A streptococcal infection
Recurrent attack of RF in a patient without rheumatic heart disease: Two major or one major and two minor manifestations plus evidence of a preceding group A streptococcal infection
Recurrent attack of RF in a patient with established rheumatic heart disease: Two minor manifestations plus evidence of a preceding group A streptococcal infection
Rheumatic chorea, insidious onset rheumatic carditis: Other major manifestations or evidence of group A streptococcal infection not required
Chronic valve lesions of rheumatic heart disease: Patients do not require any other criteria to be present if diagnosed for the first time as having rheumatic heart mitral stenosis, mixed mitral valve and/or aortic valve disease
Patients that present with polyarthritis, polyarthralgia or monoarthritis and L3 minor manifestations along with evidence of recent group A streptococcal infection should be considered as probable rhe11111nticfever once other diagnoses are excluded, particularly in vulnerable age groups in high incidence settings. They require close followup and regular secondary prophylaxis.

- E_s_s_e_n_ tia_P_e_d_i_atr-ics_________________________________
Pericarditis results in precordial pain that may be quite severe. On auscultation a friction rub is present. Clinical pericarditis is seen in approximately 15% of those who have carditis. The electrocardiogram may show ST and T changes consistent with pericarditis. As a rule, the rheumatic pericarditis is associated with only small effusionsanddoesnotresult either intamponade or cons trictive pericarditis. A patient of rheumatic pericarditis always has additional mitral or mitral and aortic regurgitation murmurs.
Other features of carditis are (i) cardiac enlargement, (ii) soft first sound, (iii) protodiastolic (S3) gallop, (iv) congestive cardiac failure and (v) Carey Coombs' murmur. This is a soft delayed diastolic mitral murmur heard transiently during the course of acute rheumatic fever possibly as a result of flow across the inflamed and thickened mitral valve.
Endocarditis is represented by a pansystolic murmur of mitralregurgitationwith orwithout an associated aortic regurgitation murmur. Pathologically mitral valve is involved in all cases of rheumatic fever with carditis. Clinically, however, 5-8% patients may present as pure aortic regurgitation. Thus almost 95% patients will have mitral regurgitationmurmur, a quarter of them also have an aortic regurgitation murmur and only 5% present as pure aortic regurgitation. Tricuspid valvulitis resulting in tricuspidregurgitation occurs in 10-30% of cases. Isolated tricuspid valvulitis as a manifestation of acute rheumatic endocarditis does not occur. Clinical evidence of pul monary valve involvement in acute rheumatic fever is never seen. The acute hemodynamic overload resulting from acute mitral regurgitation and/or aortic regur gitation leads to left ventricular failure and is the main reason for the morbidity and mortality of rheumatic fever and RHD.
(ii) Arthritis. Rheumatic arthritis is a polyarthritis involving large joints that include knees, ankles and elbows. Uncommonly smaller joints mayalsobe involved. It is a migratory polyarthritis with the affected joints showing redness, warmth, swelling, pain and limitation of movement. It is an early manifestation and occurs in 70-75% of cases according to western literature. However, the figures from India indicate that arthritis is seen in 30 to 50% of patients. The pain and swelling appear rather quickly, last 3 to 7 days and subside spontaneously to appear in some other joint. There is no residual damage to thejoint. Arthritis tends to be commoner in older patients.
(iii) Subcutaneous nodules. Subcutaneous nodules appear on bony prominences like elbows, shins, occiput and spine. They vary in size from pinhead to an almond. They are non-tender. Subcutaneous nodules are a late manifestation and appear around 6 weeks after the onset of rheumatic fever though they have been described as early as 3 weeks from the onset. They occur in about 3 to 20% ofcasesofrheumatic fever inIndia. Patients whohave
subcutaneous nodules almost always have carditis. They last from a few days to weeks but have been known to last for almost a year.
(iv)Chorea. Sydenham's chorea is also a late manifestation occurring about three months after the onset of acute rheumatic fever. Generally by the time a patient manifests chorea, the signs of inflammationusually subside. Chorea consists of semi-purposeful, jerky movements resulting in deranged speech, muscular incoordination, awkward gait and weakness. The affected child is emotionally disturbedanddrops things she or he is carrying. It is three to four times more common in females as compared to males. Untreated, it has a self-limiting course of two to six weeks.
(v)Erythema marginatum. It is an early manifestation, predominantly seen over the trunk. The rash is faintly reddish,notraisedabovethe skin andnon-itching.It starts as a red spot with a pale center, increasing in size to coalescewithadjacentspots to form aserpiginousoutline. We believe that the inability to recognize erythema marginatum is not because it does not occur but because of the dark complexion of the skin.
Minor criteria These include:
(i)Clinical criteria
(a)Fever. Rheumaticfeveris almostalwaysassociatedwith fever. The temperature rarely goes above 39.5°C.
(b)Arthralgia. Arthralgia is defined as subjective pain whereas arthritis means subjective symptoms as well as objective signs of joint inflammation. Whereas arthritis is a majormanifestation, arthralgia is a minor manifestation. Figures from India indicate that arthritis and arthralgia together occur in about 90% of the patients
(c)Previous rheumaticfever or rheumatic heart disease. This minor criterion is applicable only for a second attack of rheumatic fever.
Laboratory Manifestations
(a)Acute phase reactants consist of polymorphonuclear leukocytosis, increased sedimentationrateand C-reactive protein. Theleukocytecountusuallyliesbetween 10,000 to 15,000/cu mm. The sedimentation rate is elevated during acute rheumatic fever and remains so for 4 to 10 weeks in almost 80% of patients. In a small proportion of patients it may remain elevated even beyond 12 weeks. Although congestivecardiacfailuretendstobringthesedimentation rate down toward normal, it is unlikely that a patient of acute rheumatic fever in congestive cardiac failure will have a normal sedimentation rate. C-reactive protein is increased in all patients of acute rheumatic fever. It subsidesrapidlyifthepatientisonsteroids.Whileabsence of C-reactive protein is strongly against the diagnosis of acute rheumatic fever, its presence is non-specific.
(b)Prolonged PR interval in tfte electrocardiogram. Prolonged PR interval is a non-diagnostic criterion since it can get

prolonged in many infections. It is also not diagnostic of carditis. Higher grades of block like second degree atrioventricular block specially of the Wenckebach type may also be seen. Complete atrioventricular block is extremely rare.
Essential Criteria
These include evidences of recent streptococcal infection. The commonest in use is the antistreptolysin 'O' titer (ASO). Elevated levels of ASO only indicate previous streptococcal infection andnotrheumaticfever. Although generally the higher the level the more likely one can conclude a recent streptococcal infection, lower levels considered "normal" do not necessarily exclude a recent streptococcal infection. If the basal ASO titer of an individual is 50 units and it goes up to 250 units, it is indicative of recent streptococcal infection. Rising titer of ASO is a strong evidence for a recent streptococcal infection.
Positive throat culture for streptococci is relatively uncommon,when a patient presents with acute rheumatic fever. Positive throat culture can also not be equated with the diagnosis of rheumatic fever. Positive throat culture means that streptococci are present in the throat. The patient may or may not have rheumatic fever.
The third feature suggestive for the diagnosis of recent streptococcal infection is the presence of residua of scarlet fever. The desquamation of skin of palms and soles indicates that the patient has had scarlet fever within the previous two weeks. Scarlet fever is rare in India.
Echocardiography. Although the revised Jones criteria do not include echocardiographic findings for the diagnosis of carditis, this is a sensitive investigation for diagnosis of rheumatic carditis. The features indicative of rheumatic carditis consist of annular dilatation, elongation of the chordae to the anterior leaflet of the mitral valve causing a prolapse andlack of coaptation of the two leaflets result ing in mitral regurgitation. There is focal nodular thickening of the tips of the mitral leaflets, which do not have an independent chaotic movement seen with infective endocarditis. In addition, there is variable degree of increase in the left atrial and ventricular size. Involve ment of the aortic valve is recognized as aortic regur gitation. Occasionally, the leaflet tip of the mitral valve becomes flail during an episode of rheumatic fever because of chordal rupture resulting in severe mitral regurgitation.
Echocardiography has improved recognition of the presenceofcarditis,which at times isnotpossible clinically by auscultation. This has lead to the recognition of the entity of subclinical carditis in which although there are no clinical findings to suggest mitral regurgitation, the echocardiograpic findings indicate mitral regurgitation. While the course of patients with subclinical carditis is not clear, most patients are advised longterm penicillin prophylaxis.
Disorders of Cardiovascular System -
Treatment
Management is symptomaticcombined with suppressive therapy.
Bed rest. Bed rest is generally recommended for acute rheumatic fever. Patients who do not have cardiac involvement can be ambulant in two to three weeks whereas when carditis is present, immobilization may have to be continued for one to three months specially in the presence of congestive failure.
Diet. In the absence of cardiac involvement there should be no restriction in salt intake. Even in the presence of cardiacinvolvement, saltrestrictionis notnecessaryunless congestive cardiac failure is present and not responding well to treatment.
Penicillin. After obtaining throat cultures the patient should be put on penicillin. A single injection of benzathine penicillin can be administered when the diagnosis of rheumatic fever is made. Penicillin V (250 mg four times a day for 10 days) is another alternative; erythromycin (250 mg qidfor10 days)canbeadministered for those with penicillin allergy.
Suppressive therapy Aspirin or steroids are given as suppressive therapy. Since untreated rheumatic fever subsidesin12weeksin80%ofthepatients,eitherofthetwo suppressive agents is given for 12 weeks. Steroids are a more potent suppressive agent as compared to aspirin. However,there is no proofthat the use of steroids results in less cardiac damage as compared to aspirin. A number of observations indicate that steroids act faster and are superioratleastintheinitialphases.Pericardia!frictionrub tends to disappear within three to five days after starting thesteroidsandanewfrictionrubdoesnotappear. Despite adequatedosesofaspirinhavingbeengiven,anewfriction rub may still make its appearance. Subcutaneous nodules tend to disappear faster with the use of steroids as compared to aspirin. Patients who have carditis with congestivecardiacfailurehaveahighermortalityifaspirin is used compared to steroids. In selecting the medication, the following guidelines are followed:
•Carditis with congestive cardiac failure: use steroids
•Carditis without congestive cardiac failure: One may use either steroids or aspirin, however, steroids are preferred
•If the patient does not have carditis, it is preferable to use aspirin.
The total duration of course for the suppressive agent, aspirin or steroids, is 12 weeks. Aspirin is given at a dose of 90-120 mg/kg/day (in 4 divided doses) for 10 weeks, and then tapered in the next two weeks. Alternatively, prednisolone (2 mg/kg daily; maximum dose 60 mg) is given for three weeks and then tapered gradually in next 9 weeks. The management of congestive cardiac failure is based on principles discussed above.
. ---E-ssentia_lPe_diatrics_----------------------------------
Surgical replacement of the mitral and/or aortic valve is indicated if the patient is deteriorating despite aggressive decongestive measures. Acute hemodynamic overload due to mitral or aortic regurgitation is the main cause of mortality due to rheumatic fever.
Management ofchorea. The patient as well as the parents should bereassuredand toldabout theself-limitingcourse of the disease. The signs and symptoms of chorea do not respond well to anti-inflammatory agents or steroids. Supportive measures such as rest in a quiet room and medications such as haloperidol, diazepam and carbamazepine are effective.
Prevention of Rheumatic Fever
Primaryprevention requires identification of streptococcal sore throat and its treatment with penicillin. For primary prevention, it is necessary to educate the community regarding the consequences of streptococcal sore throat. Logistically it is difficult since it requires (i) identification ofsorethroat thatisdependentoneducationof parents, (ii) rapidly confirming that sore throat is streptococcal: requires availability of microbiological facilities, and (iii) medical help and availability of penicillin. Data from recent epidemics of rheumatic fever indicates that anywhere from 30 to 80% of sore throats resulting in rheumatic fever can be asymptomatic. Because asympto matic streptococcal pharyngitis can result in rheumatic fever, primarypreventioncanonlybepossiblebyusingan anti-streptococcal vaccine, which is not available.
Secondary prevention consists in giving long-acting benzathine penicillin. The dose is 1.2 million units once every 3 weeks or 0.6 million units every alternate week. The injection is painful and since some patients get fever for 24 to 36 hr following the injection, it is preferable to give the injection on a weekend to avoid school absence. While the responsibility of continuing penicillin prophylaxis is on parents, the physician should explain theseriousness of the problem and the needfor prolonged treatment (Table 15.17).
Duration of Secondary Prophylaxis
Recommendations of the WHO are widely accepted. Patientwithoutprovencarditisshouldreceiveprophylaxis for 5 yr after the last episode, or until they are 18-yr-old
Table 15.17: Secondary prophylaxis following an episode of rheumatic fever
Antibiotic |
Mode of administration, dose |
Benzathine |
Single intramuscular injection every 3 to |
penicillin |
4 weeks*, 1200 000 units for patients ;?.30 |
|
kg; and 600 000 units for <30 kg |
Penicillin V |
250 mg orally twice daily |
Erythromycin (for |
250 mg orally twice daily |
penicillin allergy) |
|
*In high prevalence regions, 3 wk injections are recommended for prophylaxis, in patients >30 kg and every 2 weeks in patients <30 kg
(whichever is longer). Patient with carditis (mild mitral regurgitation or healed carditis) should receive prophy laxisfor 10yrafterthelastepisode,or at leastuntiltheyare 25-yr-old (whichever is longer). Patients with established RHD disease orfollowing valve surgery or balloon mitral valvotomy should receive lifelong prophylaxis. Some cardiologists recommend discontinuation of prophylaxis after the age of 40 yr, since the likelihood of recurrence beyond this age is minimal.
Rheumatic Heart Disease
The sequelae of rheumatic fever consist of mitral, aortic and tricuspid valve disease. Mitral valve involvement manifests predominantly as mitral regurgitation (MR) and much less commonly asmitral stenosis (MS).Aortic valve and tricuspid valve involvement presents as aortic (AR) andtricuspid regurgitation (TR), respectively.Rheumatic aortic stenosis (AS) is very rare in childhood or adolescence.
Mitral Regurgitation
Mitral regurgitation (MR) is the commonest manifestation of acute as well as previous rheumatic carditis. In our study of 850 patients of RHD below the age of 12 yr, 750 had pure or dominant MR.
Hemodynamics
Mitral regurgitation results in a systolic leak of blood to the left atrium. The regurgitant volume of blood reaches the left atrium during ventricular systole at almost systolic pressure. However, during diastole it can pass freely across the mitral valve. Thus, although the left atrial pressureincreases during systole, it drops during diastole. The mean left atrial pressure, therefore, stays normal or is only slightly increased. There is thus only a minimal increase in pulmonaryvenous pressure andno pulmonary congestion. The increased volume of blood handled by the left atrium and left ventricle results in an increase in the size of both these chambers. Mitral regurgitation provides two exits for the left ventricular blood-the forward flow through the aortic valve into the systemic circulation and thebackwardleak into the left atrium. The forwardoutputbecomesinsufficientduring exertion.This decrease in the systemic output results in fatigue, the commonest symptom of significant MR. Absence of pulmonary congestion prevents occurrence of dyspnea unless the MR issevereor the left ventricular myocardium is failing. With failing left ventricle, the left ventricular diastolic pressure increases, the left atrial and pulmonary venous pressure increase and pulmonary congestion appears. There is an increase in pulmonary arterial pressure andfeatures of pulmonary arterial hypertension appear. Thus presence of features of pulmonary arterial hypertension in a patient having pure MR suggests
(i) severe MR or (ii) failing left ventricular myocardium. MR developing during acute rheumatic fever is of sudden onset. It results in anacute hemodynamicoverload

over the left ventricle. The features of left ventricular failure can occur even with relatively moderate leaks during the acute illness. The size of the left atrium also plays asignificantrole in MR. Withacute MR the left atrial size is normal and the increased volume reaching the left atrium increases the left atrial and the pulmonary venous pressure, resulting in pulmonary congestion and features of left ventricular failure. With long-standing MR the left atrium increases in size to accommodate the regurgitant volume without increasing the left atrial pressure and features of left ventricular failure are absent. Another important adjustment consists of decrease in the systemic
vascular resistance to help increase the forward flow. The maximum ejection of blood into the aorta takes place duringearlysystole.The combination ofthese two factors results in an increased systolic and decreased diastolic pressure in the systemic circuit. The pulse pressure is, therefore, increased resulting in the small water hammer pulse of MR.
Clinical Features
Therestingpulse rate is increased tomaintain an adequate cardiac output. In absence of pulmonary congestion the respiratory rate is normal. Features of left ventricular failure are absent and appear late unless the MR is acute, severe or left ventricular myocardium isJailing. The heart size isdependentonthe severity of MR as well asthe status of the left ventricular myocardium. The cardiac apex is displaceddownward andoutward withforcibleapex and hyperkineticprecordium. Less than 10% of patients have a systolic thrill because of posterior direction of the regurgitant stream. The first sound may be soft as it is masked by the systolic murmur. The second sound is normally split with mild MR. With moderate or severe MR the second sound is widely and variably split. The wide split is due to an early aortic componentofthe second sound. With failing left ventricle the wide splitting disappears. Except with very mild MR, a third sound is
audible at the apex and indicates increased early rapidfilling of the leftventricle.WithsevereMR a delayeddiastolicmitral murmur starting with the third sound is audible. The delayed diastolic murmur is secondary to a largeflow across the mitral valve during diastole. Not infrequently this delayed diastolic murmur may be palpable as a short diastolic thrill. InpureMR, the delayed diastolic murmur always ends somewhere in mid-diastole and there is no late diastolic (presystolic) accentuation. The classical diagnostic sign is the pansystolic murmur, best heard at the apex and widely radiating to the axilla and back as well as to the left sternal border (Fig. 15.41).
The electrocardiogram shows sinus tachycardia and a normal axis. Signs of left ventricular hypertrophy may be present with long-standing and severe MR. The thoracic roentgenogram shows cardiac enlargement secondary to left ventricular enlargement, the size depending on the severity of MR. Left atrial enlargement may be inferred
Disorders of Cardiovascular System
_ |
____Lb--T \ |
. |
||
• |
L |
|||
|
------ |
|||
|
|
|
||
- |
|
|||
81 P8M 82 |
|
|||
Fig. 15.41: The characteristic pansystolic murmur. As the left ventricular (LV) pressure exceeds the left atrial pressure (LA) the first sound (51) occurs. However, the murmur of mitral regurgitation will also start at the same time masking the 51. Since the maximum difference in the LV and LA pressure is quickly reached and maintained throughout systole, the murmur maintains the same intensity throughout systole appearing pansystolic. Finally as the LV pressure drops below the aortic (Ao) pressure, N2 occurs. The LV pressure is higher than LA pressure at this time and the murmur goes beyond, A2 thus masking both the 51 and A2. (PSM pansystolic murmur)
from the elevation of left bronchus. In the absence of left ventricular failure, there is absence of prominence of pulmonary veins as well as features of pulmonary congestion. Echocardiogram shows enlarged left atrium and ventricle. The specific findings of pathology of mitral valve affliction can be demonstrated vividly by two dimensional and three-dimensional echocardiography, and this is essential to plan treatment. Color Doppler can quantify MR non-invasively (Fig. 15.42).
Differential Diagnosis
Other causes of MR in childhood include: (i) atrial septal defect of the primum variety; (ii) coarctation of the aorta with MR (congenital); (iii) left ventricular fibroelastosis;
(iv)congenital corrected transposition of great arteries;
(v)papillary muscle dysfunction in dilatation of left ventricle fromany cause including myocarditis; (vi) atrial septal defect of the secundum type with floppy mitral valve; (vii) Marfan and Hurler syndrome, and
(viii)anomalous origin of left coronary artery from pulmonary artery.
Treatment
Mild to moderate MR is well tolerated for long periods. However, its severity increases with time. Medical management consists of the use of digitalis and diuretics

___E_s_s_ en_t_ai1_P_ed_ai_t _rics __________________________________
Diastole
Fig. 15.42: Rheumatic mitral valve disease with mitral stenosis and regurgitation. These frames are from a 10 yr old child with rheumatic heart disease with severe affliction of the mitral valve. Although the predominant lesion is mitral regurgitation, there is also some mitral stenosis. Three dimensional (3D) echocardiograms are shown in the upper panel and equivalent two dimensional frames obtained from apical four chamber views are in the lower panel; (A) The diastolic frame in the 3D image shows the mitral valve from its left atrial aspect. Note that the leaflet substance is seen in diastole; CB) Equivalent diastolicframe on 2D shows several featuresrheumaticaffliction. The anteriormitralleaflet(AML) isthickened. The tip of theAML isoriented horizontally and does not point downwards suggesting restriction of mobility of diastolic motion. The posterior mitral leaflet (PML) is also thickened and mobility is restricted to a greater degree. The chordae tendinae beneath the PML are visibly thickened; (C) During systole the PML stays in a relatively fixed position. The free edge of the AML moves to a position above the optimal zone of coaptation between the two leaflets. The resultantregurgitation orifice is shown by white arrows inboththe 3D and 2D frames. Thisorificeistypicallycrescentic and extends along the length of the AML; (D) The resultant color Dopplerjet of mitral regurgitation is directed posteriorly and laterally
besides penicillin prophylaxis for prevention of recurrences. The role of systemic vasodilators, most commonly ACE inhibitors and calcium channel blockers, to reduce afterload in isolated MR and aortic regurgitation is controversial. An important additional consideration in RHD is the presence of varying degrees of mitral stenosis that accompanies MR.
There are no clear guidelines for the timing of mitral valve surgery (particularly replacement) in children. The natural history of MR is quite different in children and standard guidelines for mitral valve surgery in adults mightnotapplyto children. Persistent symptoms, in spite ofmaximallytoleratedmedications, warrantconsideration of surgery especially in the presence of pulmonary artery
hypertension. For anasymptomaticchild,evidenceofeven the slightestventriculardysfunction merits consideration for surgery. The treatment of choice is mitral valve repair. At present the commonest surgical approach is prosthetic valve replacement because rheumatic mitral valves are difficult to repair. It is necessary to emphasize that valve replacement is not a cure and patients need to receive anticoagulants on the longterm, which might be a challenge in young children.
Rheumatci Mtrali Stenossi (MS)
Rheumatic MS is less common than MR in children. Juvenile MS (<18 yr) is typicallyseen in regionswith high prevalence of RHD.
Hemodynamics (Fig. 15.43)
MS results in obstruction to flowof blood across the mitral valve during left ventricular diastole. The left atrium compensatesfor this obstruction by increasingitspressure. This increase in pressure results in hypertrophy of the left atrial wall. Unfortunately, the left atrium is a thin walled chamber and the capacity for hypertrophy of the left atrial wall is limited. The increase in left atrial pressure prevents decrease in the blood flow across the mitral valve. The increased left atrial pressure is transmitted to pulmonary veins andresultsin pulmonarycapillaryengorgementand pulmonary congestion, which produces dyspnea, the commonest symptom of MS. The pulmonary arterial pressure increases to maintain forward flow from the pulmonary artery to the left side of the heart. In the absence of tricuspid regurgitation the right ventricular hypertrophy is concentric without an increase in the size of right ventricular chamber. The heart size usually stays normal.
Fig. 15.43: Hemodynamics of mitral valve stenosis: A cardiac catheterization tracing with simultaneous recording of left atrial (LA) with ·a· and 'v' waves and left ventricular (LV) waveforms is shown. A continuous wave Doppler record is superimposed during diastole; note the two peaks in flow acceleration-the second peak coincides with pre-systolic accentuation. The flow patterns reflect the pressure gradients across the mitral valve in diastole. A2 aortic component of second heart sound; OS opening snap

With mild or moderate MS, the forward flow through the mitral valve remains normal. With severe obstruction the forward flow is diminished with reduced cardiac output resulting in a small volume pulse and cold extremities.
Clinical Features
Boys are twice as commonly affected as girls in the age group up to 12 yr. Juvenile rheumatic MS has been described in children as young as 5 yr. Patients with MS give history of shortness of breath on exertion or even at restdependingon theseverity. Other importantsymptoms consist of cough, hemoptysis, paroxysmal nocturnal dyspnea, attacks of acute pulmonary edema and atypical angina. On examination, the pulse volume is small. The respiratory rate is increased except in patients with mild mitral obstruction. Depending on the severity, there may or may not be signs of right-sided congestion, in the form ofengorgedneck veins andenlarged tender liver. Theliver mayhavesystolicpulsationsif there is associated tricuspid regurgitation; the jugular venous pulse shows prominent 'a' waves. If tricuspid regurgitation is present, the jugular veins show dominant 'V waves. With moderate or severe MS, signs of pulmonary congestion in the form of rales are present.
Examination of the precordium reveals a normal sized heart with a tapping apex beat, parasternal impulse and an apical diastolic thrill. The second sound may be palpable at the second left interspace. On auscultation the firstsoundis accentuated, the second soundnormallysplit with a loud pulmonary component. An opening snap of the mitral valve is best audible just medial to the apex. The delayed diastolic mitral murmur starts immediately following the opening snap, diminishes somewhat in intensity during mid diastole and accentuates again at the end of diastole. The late diastolic accentuation is always present in the presence of MS. Absence of late diastolic accentuation of murmur is against the diagnosis of dominant MS.
The electrocardiogram shows right axis deviation with right ventricular hypertrophy. In addition, there is evidence for P mitrale. Thoracic roentgenogram shows a normal sized heart with features of pulmonary venous and arterial hypertension, as well as left atrial enlarge ment. Echocardiogram shows decreased EF slope, para doxicalposteriorleafletmotion,left atrialenlargementand pulmonary arterial hypertension.2D echo can identify the narrowed mitral opening. Doppler echo provides accurate information on transmitral gradient.
Assessment of severity The minimum criteria for the
clinical diagnosis of MS are accentuatedfirst sound, the mitral
opening snap and delayed diastolic murmur with late diastolic
accentuation. The closer the openings snap to the second sound, the more severe the mitral obstruction. The intensity or the duration of the diastolic murmur does not correlate with the severity since mild as well as severe
Disorders of Cardiovascular System -
MS may result in very soft murmurs. The duration of the murmur depends on the heart rate. Whereas mild pulmonary arterial hypertension may be present with mild, moderate or severe mitral obstruction, severe pulmonary arterial hypertension can occur only with severemitralobstruction. Echocardiogram (determination of cross-sectional area) combined with Doppler gradient gives more precise assessment of severity. Atrial fibrillation is rare in the pediatric age group.
Differential Diagnosis
Very few conditions can be considered in the differential diagnosis in children. Isolated congenital MS is very rare. The opening snap is less commonly heard in congenital MS. Cortriatriatum, obstruction of individual pulmonary veins and left atrial myxoma should be considered in the differential diagnosis.
Treatment
The management of MS is essentially catheter based or surgical. Beta blockers or digoxin work equally well by reducing resting and exercise heart rates thereby improving diastolic filling. Diuretics help by reducing pulmonaryvenous congestion. Balloonmitral valvotomy (BMV), also known as percutaneous trans-septal mitral commissurotomy (PTMC) has largely replaced closed or open mitral commissurotomy for MS in children. Improvement in mitral valve area following these procedures largely results from splitting of the fused commissures. The sub-valvar pathologic abnormalities of MS remain after valvotomy, so the mitral valve area does not normalize. The balloon, introduced through the femoral vein is passed through the atrial septum, positioned in the mitral valve and inflated to open the stenotic valve.
Longterm followup after valvotomy is mandatory because of significant risk of restenosis with time. Restenosis is typically associated with significant residual MS following balloon mitral valvotomy. A repeat procedure is an option for restenosis and helps postpone mitral valve surgery. Closed mitral valvotomy (CMV) is an inexpensive and equally effective surgical alternative to BMV.
Aortic Regurgitation (AR)
Aortic valve involvement in RHD results inAR. Clinically pure AR, without associated mitral valve disease, is rare and occurs in 5 to 8% patients. Pathologically pure rheumatic aortic valve disease is almost unknown.
Hemodynamics
AR is a backward leak from the aorta into the left ventricle during diastole. This increases the volume of blood reachingtheleftventricle. Theleftventricleincreasesinsize to accommodate the extra volume. The size of the left ventricleis thusdirectlyrelatedtothedegree ofaorticleak,

__E_s_s_ en_t_ia_l_P_ed_ait _rcis_ __________________________________
unless there is myocardial disease. Because of the backward flowofbloodthe forwardflowisimpaired. This is compensated by peripheral vasodilatation as well as increased ejection from the left ventricle during early part of the systole. However, significant AR results in low forward output. Signs of wide pulse pressure in the form ofexaggeratedarterialandarteriolarpulsationsarepresent unless the AR is mild. Slowing of heart rate increases the diastolic period and increases the regurgitant volume of blood in AR. With good left ventricular myocardial function, even moderate AR is tolerated well for long periods. If theleft ventricularmyocardiumisfailingtheleft ventricular diastolic pressure goes up and results in an increase in left atrial pressure and pulmonarycongestion.
Clinical Features
Aortic valve disease is more common in boys compared to girls. The main symptom is palpitation, related to the large stroke volume. With mild to moderate AR the forward flow can be raised effectively on exercise. Thus fatigue is not an early symptom.
The pulse pressure is wide. The wider the pulse pressure, the more severe the aortic leak. The diastolic blood pressure may be recorded as zero with severe AR. Prominent carotid pulsations (Corrigan sign), visible arterial pulsations over extremity vessels (dancing peripheral arteries) and visible pulsations of the abdominal aorta are evidencesofwide pulsepressurefrom any cause. Holding the middle of the forearm or leg and elevating it discloses a sharply rising and abruptly falling pulse
(Corrigan pulse or water hammer pulse). Nodding of head may be present with each systole (de Musset sign) due to sudden filling of carotid vessels in severe AR. Arteriolar pulsations may be seen over the nail bed, uvula, lips, ear lobes and in the eye grounds. There is also exaggeration of the systolic pressure difference between the brachia! and femoral arteries (Hill sign). Normally the difference between the pressures in brachia! artery and femoral arteryis lessthan20 mmHg, thefemoral systolic pressure being higher. Systolic pressure difference between 20 to 40 mm Hg suggests mild AR, 40 to 60 mm moderate AR, and more than 60 mm Hg severe AR. If a stethoscope is put over the brachia! or the femoral artery without applying pressure pistol shot sounds may be heard in moderate or severe AR. A systolic murmurmay be heard if pressure is applied to partially occlude the artery proximal to the chest piece, and diastolic murmur if pressure is applied distally; the combination of systolic and diastolic murmurs is the
The apex is displaced downward and outward and is forcible or heaving. A diastolic thrill is unusual. The first soundissoftandthe aortic componentofthesecondsound may be audible or may be masked by the regurgitant diastolic murmur. The murmur of AR is a high-pitched, decrescendo diastolic murmur starting with the aortic component of the second sound. The intensity and the
length of the murmur do not correlate with the severity of AR. The murmur is heard along the left sternal border and radiates to the apex and even beyond. With large aortic leaks there is also an ejection systolic murmur at the second right interspace, conducted to the neck and not infrequently associated with a systolic thrill. The systolic murmur is the result of a large stroke volume, passing across rough valves. It does not indicate aortic stenosis if the pulse pressure is wide and the carotid upstroke is brisk.
Theelectrocardiogramshowsincreaseinleftventricular voltages with deep S waves in Vl and tall R waves in V6. TherearealsodeepQwavesinleftchestleadsaccompanied withtallTwaves;thisiscalleddiastolicoverloadingpattern of the left ventricle. The thoracic roentgenogram shows cardiacenlargementoftheleftventriculartypeanddilated ascending aorta. Echocardiogram identifies enlarged left ventricle, dilatedaortaandflutterofanteriormitralleaflet. Doppler echo can quantitate the severity of AR.
Differential Diagnosis
The differential diagnosis of rheumatic AR includes two sets of conditions: (i) conditions associated with a wide pulse pressure like patent ductus arteriosus, arteriovenous fistulae, ventricular septal defect with AR, ruptured sinus of Valsalva, anemia and thyrotoxicosis, (ii) conditions
associated with a non-rheumatic regurgitant diastolic murmur like pulmonary regurgitation, AR with ventricular septal defect, ruptured sinus of Valsalva and congenital aortic valve disease. As a rule congenital aortic valve disease is either a leaking bicuspid aortic valve or aortic stenosis. Pure congenital AR is extremely rare. Other conditions that may result in AR include Marfan syndrome, Hurler syndrome and Takayasu aortoarteritis.
Management
Mild to moderate AR is well tolerated for years. There is role for therapy with calcium channel blockers. Significant AR, if associated with either chest pain or left ventricular failure, should be treated surgically. Surgical treatment consists of aortic valve replacement either by homograft or prosthetic valve; valve repair is not feasible for rheumatic AR. Better surgical results are obtained before onset of significant ventricular dysfunction.
Patients planned for valve replacement should be screened for: (i)rheumatic activity; (ii) abilityof the family to take lifelong anticoagulants. Aortic valve replacement has fewer longterm complications when compared to mitral valve replacement.
Tricuspid Regurgtati oni (TR)
Features indicative of TR are seen in 20 to 50% patients of RHD in children in our country. It is often difficult to determine whether TR is organic (due to involvement of thetricuspidvalve bytherheumaticprocess) or functional (due to pulmonary hypertension).

Hemodynamics and Clinical Features
TR results in a systolic backflow of blood from the right ventricle to the right atrium. The systolic leak thus results in a systolic murmur and a volume load of the right atrium as well as the right ventricle. As a rule, almost all patients who have TR also have features of pulmonary arterial hypertension. The systolic backflow under pressure results in a prominent systolic wave, the V wave, in the jugular venous pulse as well as the liver. Both the systolic as well as the diastolic murmurs at the tricuspid valve become louder during inspiration. In patients of rheumatic heart disease the TR may be associated either with MS or with MR. If the TR is associated with MS it may be either organic or functional due to pulmonary arterial hypertension. If, on the other hand, the TR is associated with dominant or pure MR it is most likely organic. This is because MR of a severity to result in pulmonary arterial hypertension of a degree to cause functional TR is rare.
There are no specific symptoms of TR. It is possible that with onset of TR the dyspnea may be relievedto some extent in patients of MS. The patients may give history of pain in right hypochondrium due to a congested liver and of fatigue due to a decrease in systemic output. In addition to features of TR there are signs of pulmonary arterial hypertension and those of mitral valve disease. In association with MS, severe TR may result in marked dilatation of the right ventricle and the whole of the anterior surface, including the apex may be formed by the right ventricle. In such patients the apex beat is not only displaced outward but also downward. This should not be mistaken for left ventricular enlargement. In these cases the pansystolic murmur of TR may be heard from the lower left sternal border to the apex. Since the left ventricle is displaced backwards, the MS murmur may be audible only in the axilla or may not be made out at all. It is not uncommon for these patients to be diagnosed as those of MR. Besides peripheral signs of TR, the electrocardiogram is helpful in separating these cases from those of MR. Patients of TR of this severity almost always show severe right ventricular hypertrophy in the electrocardiogram. Echocardiography and color Doppler can document and identify the nature (organic vs. functional) and quantitate severity of TR.
Management
Decongestive measures will help in reducing the severity of TR. Further management depends on the associated mitral valve lesion. TR may resolve following mitral valvotomy. In those patients undergoing surgery for the MR, the tricuspid valve can be inspected and tricuspid annuloplasty or repair performed if needed.
Clinical Problems in Patients with Rheumatic Heart Disease
Two major problems that clinicians face in patients of RHD are discussed below.
Disorders of Cardiovascular System -
Active or Inactive Rheumatic Fever?
A lot of 'judgment' or personal bias is generally involved in this decision. For the diagnosis of activity one has to fall back on the Jones criteria. Presence of cardiac involvement cannot be used as a major criterion since the carditis may be the result of a previous attack of rheumatic fever. However, presence of a pericardia! friction rub is evidence of active carditis. If the patient has well documented cardiac findings then the appearance of a new murmur or a significant increase in a pre-existing murmur is very suggestive for active rheumatic fever. History of arthralgia or arthritis within a period of less than 12 weeks is suggestive of active rheumatic fever specially if associated with elevated sedimentation rate and ASO titer. Despite congestive cardiac failure, it is unusual for the sedimentation rate to be normal in a patient of active rheumatic fever. All patients of RHD should show
elevated ASO titer before they can be labeled as active I rheumatic fever. The difficulty arises in those patients who
have relatively low levels of the ASO titer. In such cases, unless serial serum samples are available it is difficult to decide whether there is rise in level of ASO liter. An ASO titer of 250 units may indicate a significant rise if the baseline was 50 units.
In a Febrile Patient, Is it Active Rheumatic Fever or Infective Endocarditis?
At times separation of rheumatic activity from infective endocarditis can be very difficult. The arguments used above for separating active from inactive rheumatic fever can be used for diagnosis of active rheumatic fever. A detailed description of endocarditis follows.
Suggested Reading
Bland EF, Jones TD. Rheumatic fever and rheumatic heart disease. A twenty year report on 1000 patients followed since childhood. Circula tion 1951; 42:836
Narula J, Virmani R, Reddy KS, Tandon R. Rheumatic fever. Amer Registry Path AFIP. Washington DC, 1999
Rheumatic fever and rheumatic heart disease. Report of a WHO ex pert consultation. World Health Organization, Geneva, 2004 (Techni cal Report Series No. 923)
l FECTIVE ENDOCARDITIS
Infection of the endocardial lining of the heart is called infective endocarditis, and may involve the endocardium of the valves, the mural endocardium or the endothelium of blood vessels (infective endarteritis). The commonest site of infection is a diseased valve from where the infection can spread along the endothelium. The injection has significant morbidity.
Etiopathogenesis
Infective endocarditis predominantly occurs in a diseased heart. The commonest substrate is a damaged endothelium or endocardium resulting from contact with a high

__E_s_s_ _en_t_ial_P_ed_iat _rics __________________________________
velocity jet together with the presence of a significant bacteremia. Endocarditis can occur following a surgical shunt as in Blalock-Taussig shunt. Other congenital lesions, associated with endocarditis are patent ductus arteriosus, pulmonic stenosis and mitral valve prolapse syndrome. It is rare in atrial septal defect of the secundum type unless associated with mitral valve prolapse and mitral regurgitation.
Infective endocarditis occurs over the mitral valve or the aortic valve in patients with rheumatic heart disease. Patients with prosthetic valves or those who have had a recent cardiac operation are also especially prone to endocarditis. Infections anywhere in body like boils or furuncles, tooth abscess, ear infection, urinary tract infection or osteomyelitis may result in endocarditis. Although interventions like dental procedures, cardiac catheterization, genitourinary procedures or bronchos copy can be followed by endocarditis, it is rare to be able toidentifyapredisposingevent. An importantpredispos ing cause is poor dental hygiene. Parenteral drug abuse is a frequent cause of right-sided endocarditis involving the tricuspid or the pulmonary valve. Occasionally it can result in mitral and/or aortic valve disease as well.
Pathogenesis
The pathogenesis of endocarditis depends on the invasiveness and virulenceofthe infective organisms. The infection generally starts at a jet lesion, where the high pressure jet strikes the endocardium or the endothelium. The right ventricular mural endocardium or the tricuspid valve in VSD, aortic endothelium in AS or coarctation of the aorta, ventricular surface of the aortic valve in AR are the usual sites. Endocarditis results in immune mediated vasculitis and thrombocytopenia.
Bacteremia resulting from an infection such as a boil, furuncle, otitis media or initiated by an intervention such as cardiac or urinary catheterization or dental extraction is necessary for initiation of endocarditis. Bacteremia may also result from simple events such as brushing teeth. Bacteria that are deposited on the endocardium are covered by fibrin and platelets forming vegetations. Almost any species of bacteria and some species of fungi can cause endocarditis. Streptococcus viridians, 5. aureus, enterococci, P. aeruginosa and some gram negative bacilli are responsible for most episodes. Fungal endocarditis typically results in the setting of chronic hospitalization with indwelling central venous catheters.
Diagnosis
Any fever in a patient with known heart disease raises the question of endocarditis. The minimum criteria for the diagnosis of endocarditis consist of unexplained fever of 7 to 10 days duration in a patient with known heart disease. If this is associated with other clinical manifestations of endocarditis the diagnosis becomes more likely.
Endocarditis has been subdivided into acute and sub acute types, depending on whether the patient presented with achronicillnessor assepticemia.Endocarditis is also identified by the infective organism, for example viridans endocarditis, staphylococcal endocarditis and enterococcal endocarditis. 5. viridans results in the sub-acute form of illness while 5. aureus and other pyogenic organisms cause a fulminant (acute) and rapidly progressive illness. It is possible, for an organism like staphylococcus to cause a subacute or acute type of illness. Identification of the organism is necessary, as it helps determine the choice of antibiotics.
Clinical Features
Infective endocarditis is uncommon below the age of two years. The clinical features of endocarditis may be grouped into those (i) indicating the presence of an infection; (ii) indicating involvement of the cardiovascular system; and (iii) indicating the presence of an immunological reaction to infection. The features indicating the presence of infection consist of fever, chills, rigors, night sweats, general malaise, weakness, loss of appetite, weight loss and amenorrhea in females. Loss of appetite is a very persistent andimportantsymptom.Arthralgiaand diffuse myalgia can occur, however, arthritis does not occur except in acute endocarditis as part of septicemia when it is likely to be monoarticular.
Features indicative of the involvement of the cardiovascular system may be absent in the initial stages. Appearances of left or right heart failure, development of a new murmur or change in a pre-existing murmur, presence of embolic episodes to various parts of the body (like stroke from central nervous system embolism, hematuria from renal infarct, left flank painfrom splenic infarct, gastrointestinal hemorrhage from mesenteric embolism etc.) indicate involvement of the cardiovascular system. As damage to the valve tissue occurs, regurgitant lesions appear. These regurgitant lesions, aortic, mitral or tricuspid,progress rapidlycausinghemodynamic changes that result in congestive failure.
Features of immunological response presenting as vasculitis consist of arthralgia, myalgia, clubbing, splenomegaly and microscopic hematuria. Splinter hemorrhages are hemorrhagic spots under the nails, though suggestive, are not specificforendocarditis as they can result from minor injuries. Petechiae over the skin or mucousmembranesandconjunctiva are seeninabout50% patients. Petechiaeinthe retinaarecalledRoth spots. Osler nodes are tender erythematous nodules over the pulp of fingertips, but are relatively rare. Janeway lesions are non tender erythematous patches on the palms and soles. Clubbing and splenomegaly tend to appear 3 weeks after the onset of endocarditis.
In the acute form, the symptoms appear early and progress rapidly with hectic fever, chills and rigors. Perforation of valve cusps may result in appearance of