

Honeycombing |
17 |
|
Honeycombing with Subpleural or Basal Predominance
Definition
Pathologically, honeycombing (HC) represents destroyed and Þbrotic lung tissue containing numerous cystic airspaces with thick Þbrous walls [1] (Fig. 17.1). In addition, HC on pathology is characterized by cysts usually measuring <1 mm, often below the resolution of CT, and therefore not necessarily concordant with macroscopic HC seen on CT images. On thin-section CT (TSCT) scans, the appearance is of clustered cystic air spaces, typically of comparable diameters on the order of 3Ð10 mm but occasionally as large as 25 mm [2] (Fig. 17.1b). Some researchers may consider HC as a multilayer cluster of cysts with shared walls, but others may recognize a single layer cluster of cysts [3] (Fig. 17.1c).
Diseases Causing the Pattern
Cystic structures of HC on transverse CT images consist of either dilated peripheral bronchioles or alveolar ducts, surrounded by several in-folded layers of thickened alveolar septa (a true HC cyst) or tangential view of traction bronchiectasis (TB). In idiopathic pulmonary fibrosis (IPF) and usual interstitial pneumonia (UIP) (Figs. 17.1 and 17.2), cystic structures are mainly composed of true HC cysts in the peripheral portion of the lungs, while most cystic structures in patients with nonspecific interstitial pneumonia (NSIP) (Fig. 17.3) seem to be tangential views of TB [4]. Of course, even in patients with NSIP, main cysts of HC are the true HC cysts as in IPF/UIP. Honeycombing has been reported in up to 40 % of NSIP [5]. HC may be observed in approximately 10 % of patients with asbestosis (Fig. 17.4) along with Þndings
of irregular interlobular septal thickening, intralobular interstitial thickening, subpleural dot-like or branching opacity, and ground-glass opacity (GGO), not to mention of pleural plaques [6].
Distribution
In most diseases, lung abnormalities show lower lung zone and subpleural-distribution predominance. In NSIP, abnormalities may be located along the bronchovascular bundles and may demonstrate subpleural sparing [7].
Clinical Considerations
The identiÞcation of HC is essential for making the certain CT diagnosis of UIP and for predicting patient prognosis with Þbrotic IIPs [8].
Even in cases of Þbrotic idiopathic interstitial pneumonias (IIPs) with little HC, serial CT reveals an increase in the extent of HC and reticulation and a decrease in the extent of GGO. Overall extent of lung Þbrosis on the baseline CT examination appears predictive of survival in Þbrotic IIPs with little HC [9].
Measuring a Þbrotic score (the extent of reticulation plus HC) at TSCT helps predict patient prognosis. In other words, patients with UIP or Þbrotic NSIP who have a high Þbrotic score determined at thin-section CT and a low DLco level have a high death risk [10].
HC mimickers at CT are paraseptal emphysema and TB of varying severity. NSIP may simulate UIP at CT in the presence of emphysema [11]. Any Þbrotic interstitial pneumonia with concurrent emphysema may cause problems in CT interpretation [12].
K.S. Lee et al., Radiology Illustrated: Chest Radiology, Radiology Illustrated, |
153 |
DOI 10.1007/978-3-642-37096-0_17, © Springer-Verlag Berlin Heidelberg 2014 |
|
154 |
17 Honeycombing |
|
|
a |
b |
c |
d |
e
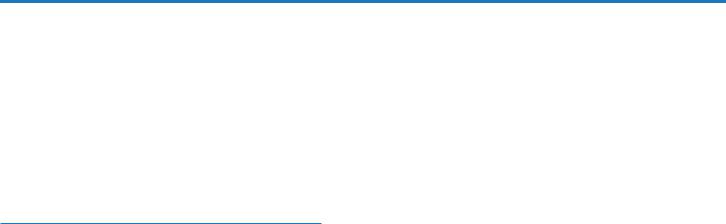
Fig. 17.1 Typical honeycomb cysts in a 50-year-old man with usual interstitial pneumonia. (a, b) Lung window images of thin-section (1.5- mm section thickness) CT scans obtained at levels of aortic arch (a) and liver dome (b), respectively, show back-to-back cysts (arrows) in subpleural regions of both lungs. Cysts are at least two layers or more in both lungs. (c) Coronal reformatted image (2.0-mm section thickness) demonstrates subpleural honeycomb cysts (arrows) in both lungs. (d)
Explanted lungs from a different patient who suffered from acute exacerbation of usual interstitial pneumonia depict consolidative lower lobes (arrowheads) through which honeycomb cysts (arrows) are visualized. Also note traction bronchiectasis (open arrows). (e) HighmagniÞcation (× 200) photomicrograph discloses combined Þndings of honeycomb cysts Þlled with mucus (arrows), interstitial Þbrosis (open arrows), and inßammatory cell inÞltration (arrowheads)
Honeycombing with Subpleural or Basal Predominance |
155 |
|
|
a |
b |
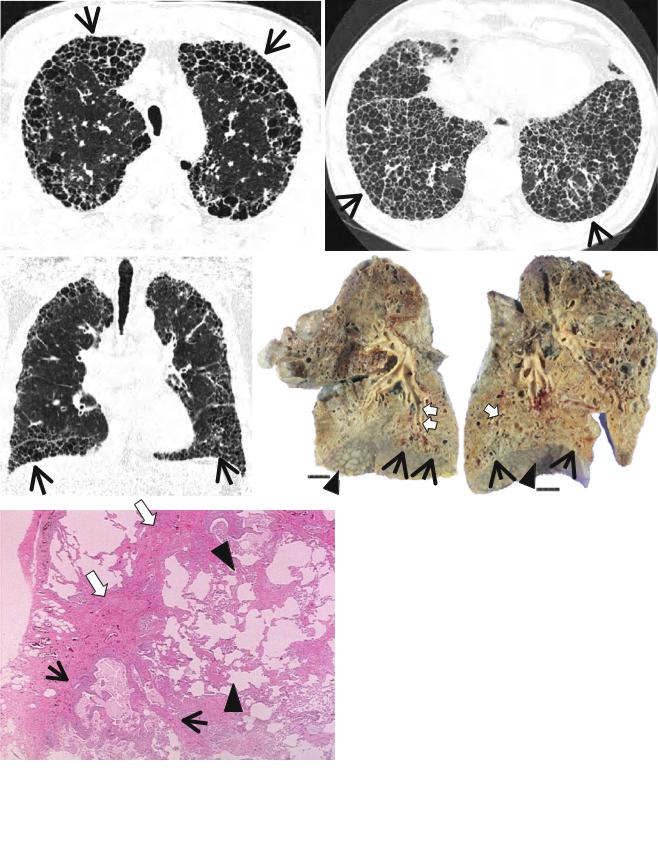
Fig. 17.2 Typical honeycomb cysts in a 58-year-old man with usual interstitial pneumonia. (a, b) Lung window images of thin-section (1.5- mm section thickness) CT scans obtained at levels of distal bronchus intermedius (a) and liver dome (b), respectively, show back-to-back
cysts (arrows) in subpleural regions of both lungs. Most cysts are at least two layers or more in both lungs. Also note some areas of pulmonary emphysema (arrowheads) in anterior lungs of the middle lung zones
a |
b |
Fig. 17.3 Honeycomb cysts in a 67-year-old woman with progressive systemic sclerosis (PSS)-associated nonspeciÞc interstitial pneumonia. (a, b) Lung window images of thin-section (1.5-mm section thickness) CT scans obtained at levels of inferior pulmonary veins (a) and liver dome (b), respectively, show honeycomb cysts (arrows) seen through
ground-glass opacity in bilateral lower lung zones. Patient had acute exacerbation of pulmonary Þbrosis and, thus, had accompanying ground-glass opacity with background honeycomb cysts. Also note distal esophageal dilatation with air Þlling (open arrows) owing to esophageal involvement of PSS
Key Points for Differential Diagnosis
|
Distribution |
|
|
|
|
|
|
|
|
|
|
Zones |
|
|
|
|
|
Clinical presentations |
|
|
|
Diseases |
U M |
L |
SP |
C R |
BV |
R |
Acute |
Subacute |
Chronic |
Others |
IPF/UIP |
+ |
+ |
+ |
|
|
+ |
|
|
+ |
|
NSIP |
+ |
+ |
+ |
+ |
+ |
+ |
|
+ |
+ |
Female predominance; subpleural |
|
|
|
|
|
|
|
|
|
|
sparing and along BV bundles |
Asbestosis |
+ |
+ |
+ |
|
|
+ |
|
|
+ |
Exposure history and pleural plaques; |
|
|
|
|
|
|
|
|
|
|
with subpleural dot-like or branching |
|
|
|
|
|
|
|
|
|
|
opacity and subpleural lines |
Note: IPF idiopathic pulmonary Þbrosis, UIP usual interstitial pneumonia, NSIP nonspeciÞc interstitial pneumonia, U upper, M middle, L lower, SP subpleural, C central, R random, BV bronchovascular
156 |
17 Honeycombing |
|
|
a |
b |
c
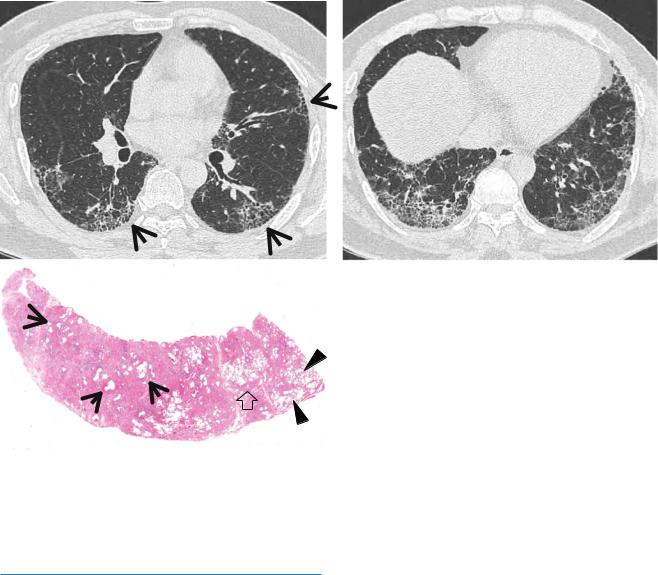
Fig. 17.4 Honeycomb cysts in a 39-year-old man with asbestosis who is working in a building demolition place. (a, b) Lung window images of thin-section (1.5-mm section thickness) CT scans obtained at levels of right middle lobar bronchus (a) and liver dome (b), respectively, show reticulation and ground-glass opacity in subpleural regions of lower lung zones. Also note scattered areas of honeycomb cysts
(arrows). (c) Low-magniÞcation (×40) photomicrograph of surgical biopsy specimen obtained from right lower lobe discloses pulmonary Þbrosis of usual interstitial pneumonia pattern with large area of irregular interstitial Þbrosis including microscopic honeycombing (arrows), few areas of chronic inßammatory cell inÞltration (open arrow), and normal lung areas (arrowheads)
Idiopathic Pulmonary Fibrosis/Usual
Interstitial Pneumonia
Pathology and Pathogenesis
In a typical case, the lungs are shrunken and Þrm when removed at autopsy or explanted. The lower lobes are most severely affected, with the pleura having a Þnely nodular ÒcobblestoneÓ pattern, resembling that of a cirrhotic liver. Pleural Þbrosis is uncommon, in contrast to asbestosis. The cut surface of the lung shows Þbrosis and a variable degree of Òhoneycombing,Ó which is most marked beneath the pleura (Fig. 17.1). The cardinal features of UIP are subpleural and paraseptal predominance, patchy parenchymal involvement, Þbrosis leading to loss of architecture, Þbroblastic foci adjacent to the established Þbrosis indicative of progressive disease, only mild to moderate chronic interstitial inßammation, and an absence of any causal feature such as inorganic dust, granulomas, or accumulations of Langerhans cells [13].
Symptoms and Signs
IPF occurs in middle-aged and elderly adults (median age at diagnosis 66 years, range 55Ð75 years) [14]. Dry cough and slowly progressive dyspnea on exertion are the cardinal symptoms of IPF. Systemic symptoms, such as fever and weight loss, are rare. Patients may be asymptomatic at the early stage of IPF. Finger clubbing is found in more than 50 % of the patients. Bibasilar Þne inspiratory crackle, socalled Velcro-like rale, is heard on chest auscultation.
CT Findings
The characteristic HRCT Þndings of UIP consist of intralobular lines and honeycombing involving mainly the subpleural regions and lung bases [15] (Figs. 17.1 and 17.2). The intralobular interstitial thickening also results in the presence of irregular interfaces between the lung and pulmonary vessels,