

Lobar Atelectasis Sign |
11 |
|
Definition
Atelectasis is derived from the Greek words ateles and ektasis meaning “incomplete expansion or stretching” [1]. The terms “atelectasis,” “collapse,” and “loss of lung volume” are used synonymously implying reduced inflation of the lung. In broad sense, atelectasis denotes diminished air within the lung associated with volume decrease, and generally, it manifests as increased density. Atelectasis can be differentiated by its volume decrease from consolidation in which volume is maintained because air is replaced by liquid or cells of approximately equal volume (Figs. 11.1, 11.2, 11.3, 11.4, 11.5, 11.6, and 11.7).
Disease Causing the Sign
Various causes of lobar atelectasis are enlisted in Table 11.1.
Distribution
All five lobes of both lungs can be involved with lobar atelectasis process. Because the right lung has three lobes, three kinds (middle and lower lobes, upper and middle lobes, and upper and lower lobes) of combined lobar atelectasis may occur in the right lung [2].
Clinical Considerations
According to its pathophysiologic mechanisms, atelectasis is classified as follows:
(1) resorption (obstructive) atelectasis by central obstruction; (2) adhesive atelectasis from surfactant deficiency, as in hyaline membrane disease of newborn; (3) passive atelectasis associated with pneumothorax and pleural effusion; (4) compressive atelectasis by adjacent masses or
elevated diaphragm; (5) cicatrization atelectasis by pulmonary fibrosis; and (6) gravity-dependent atelectasis [3, 4] (Table 11.1). Atelectasis is one of the most important radiologic findings, which should not be missed on chest radiograph, because it may suggest a hidden central malignancy. There are other peculiar entities of atelectasis, which are peripheral lobar atelectasis, migrating lobar atelectasis, platelike atelectasis, and rounded atelectasis.
Key Points for Differential Diagnosis
1.As a cause of resorption (obstructive) atelectasis, bronchogenic carcinoma is the most important one (Figs. 11.1, 11.2, 11.3, and 11.5). In a middle-aged or elderly smoker with unexplained lobar atelectasis or recurrent pneumonia, the diagnosis of bronchogenic carcinoma should be strongly suggested. The other various kinds of malignant endobronchial tumors can also obstruct the bronchi, resulting in resorption (obstructive) atelectasis, and these are bronchial carcinoid, adenoid cystic carcinoma, mucoepidermoid carcinoma, and endobronchial metastasis (breast cancer, renal cell carcinoma, melanoma, colon cancer). Rarely, benign endobronchial tumors (hamartoma, lipoma, leiomyoma, papilloma, neurogenic tumor, fibroma) can also be found as an obstructing mass.
2.Resorption (obstructive) atelectasis takes place also from obstruction of the peripheral small airways by mucus plugging. For example, postoperative patients with thoracic or abdominal trauma receiving intensive care frequently develop left lower lobe atelectasis. This results partly from impaired mucociliary clearance of secretions, which are retained in the peripheral airways with distal resorption (obstructive) atelectasis [5].
K.S. Lee et al., Radiology Illustrated: Chest Radiology, Radiology Illustrated, |
85 |
DOI 10.1007/978-3-642-37096-0_11, © Springer-Verlag Berlin Heidelberg 2014 |
|
86 11 Lobar Atelectasis Sign
3. Although bronchial neoplasm, mucus plug, and occa- |
ways which are smaller and more vulnerable to mucus |
sionally inflammatory bronchostenosis are the most |
obstruction than in adults (Figs. 11.4 and 11.6). Mucus |
frequent causes of lobar atelectasis in adults, bronchial |
plugging can also develop in other conditions such as |
tumors are uncommon in children. Instead, pneumonia |
bronchial asthma or cystic fibrosis. Aspirated foreign |
is the most common cause of atelectasis, in which the |
body (such as peanut) is another important cause of |
inflammatory exudate and secretion obstruct the air- |
lobar atelectasis in children (Fig. 11.6). |
|
|
a |
b |
|
RUL |
RUL |
|
|
RML |
|
RLL |
c |
|
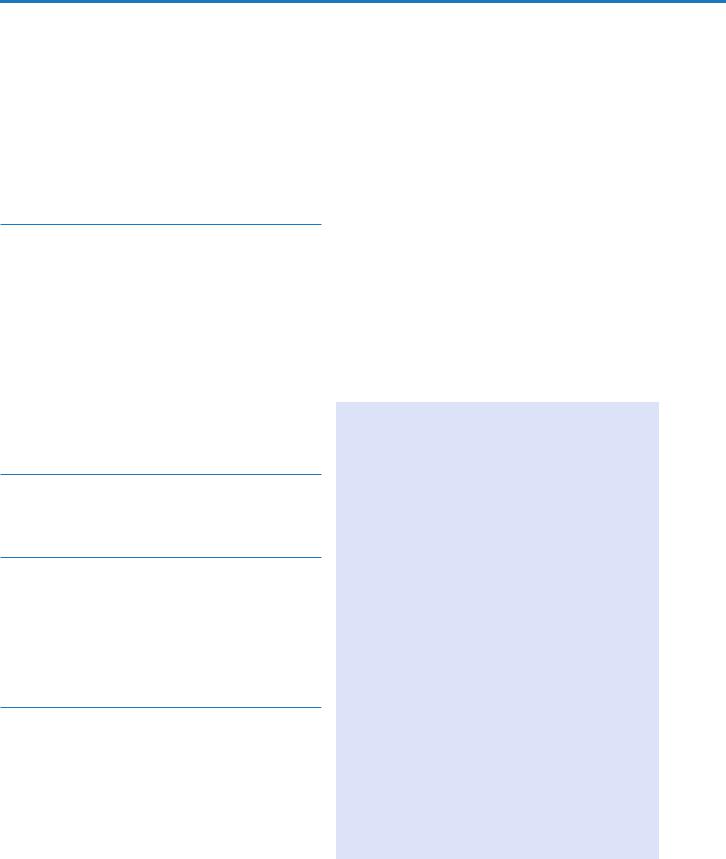
Fig. 11.1 Right upper lobar atelectasis associated central squamous cell carcinoma in a 53-year-old man. (a, b) Lung window images of CT scans (5.0-mm section thickness) obtained at levels of the aortic (a) and azygos (b) arches, respectively, show the atelectatic right upper lobe. Also note the atelectatic right upper lobe marginated posteriorly by the right major fissure (arrowheads) and superiorly elevated right middle
lobe marginated by right minor fissure (arrows). RUL right upper lobe, RML right middle lobe, RLL right lower lobe. (c) 18Fluorine fluorodeoxyglucose (FDG) PET demonstrates increased FDG uptake (arrows) within central bronchogenic carcinoma. The atelectatic right upper lobe surrounds the tumor
Combined Atelectasis of the Right Upper and Middle Lobes |
87 |
|
|
a |
b |
RUL
RUL |
RLL |
c
d
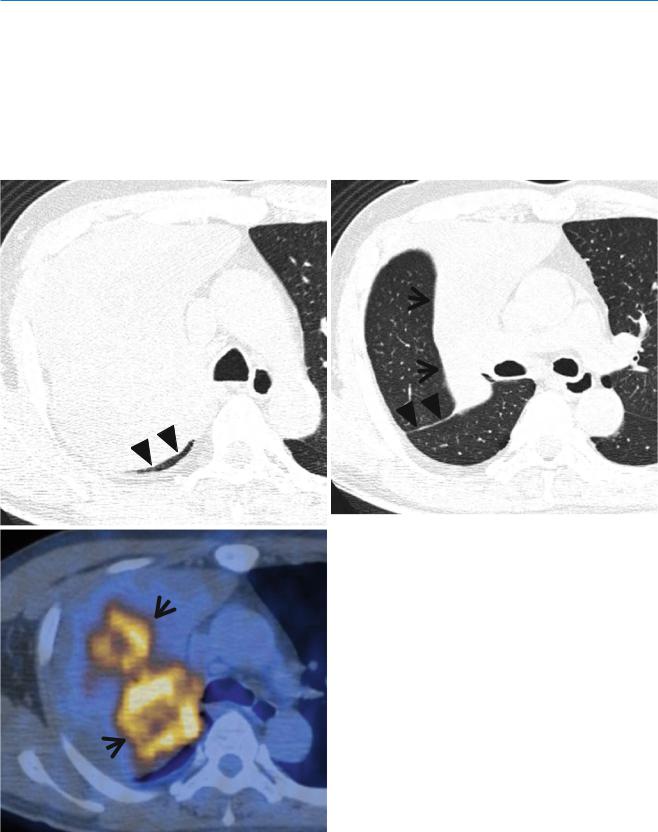
Fig. 11.2 Right upper lobe atelectasis due to bronchial aspergillosis in a 62-year-old woman who has diffuse large B-cell lymphoma. (a) Lung window image of CT scan (2.5-mm section thickness) obtained at level of the main bronchi shows the atelectatic right upper lobe bounded anteriorly by right minor fissure (arrows) and posteriorly by right major fissure (arrowheads). A central venous line (open arrow) is inserted for chemotherapy. RUL right upper lobe. (b) Coronal reformatted image (2.0-mm section thickness) demonstrates the obliterated right upper lobar bronchus (arrow) with intraluminal soft tissue, causing right
upper lobar atelectasis. Also note diffuse calcification in airway walls. RUL right upper lobe, RLL right lower lobe. (c) Bronchoscopy displays obliterated the right upper lobar bronchus (arrows) with white necrotic tissue and surrounding mucosal inflammation and edema. The right bronchus intermedius also demonstrates 50 % luminal narrowing (open arrows) with edema and inflammation. (d) High-magnification (×200) photomicrograph of pathologic specimen obtained with bronchoscopic biopsy discloses numerous fungal hyphae (arrows) infiltrating bronchial wall
88 11 Lobar Atelectasis Sign
4. The essential signs of lobar atelectasis are increased |
and (2) indirect signs, pulmonary opacification; eleva- |
opacity of the involved lobe and the evidences of vol- |
tion of the diaphragm; shift of the trachea, heart, medi- |
ume decrease. The signs can be divided into (1) direct |
astinum, and hilum; compensatory hyperexpansion of |
signs, displacement of interlobar fissures and crowd- |
the adjacent lung; approximation of the ribs; and jux- |
ing of pulmonary blood vessels and major bronchi, |
taphrenic peak. |
a |
b |
c
d
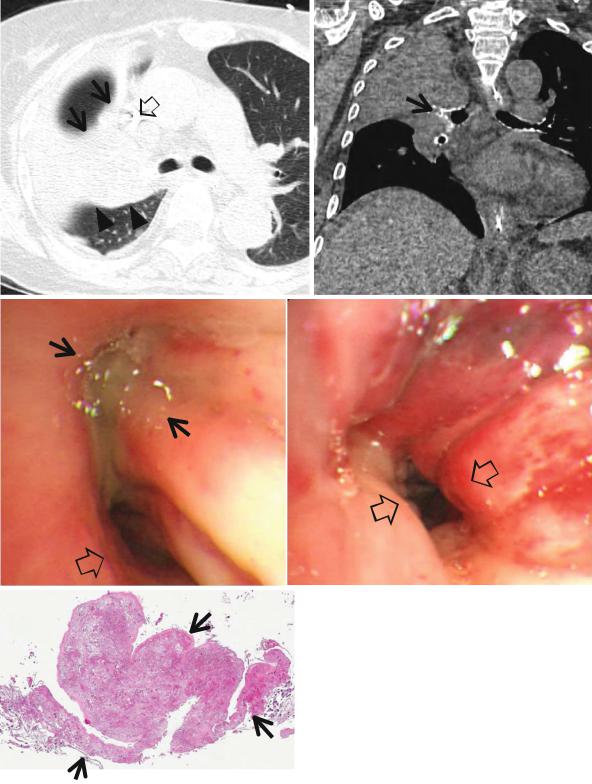
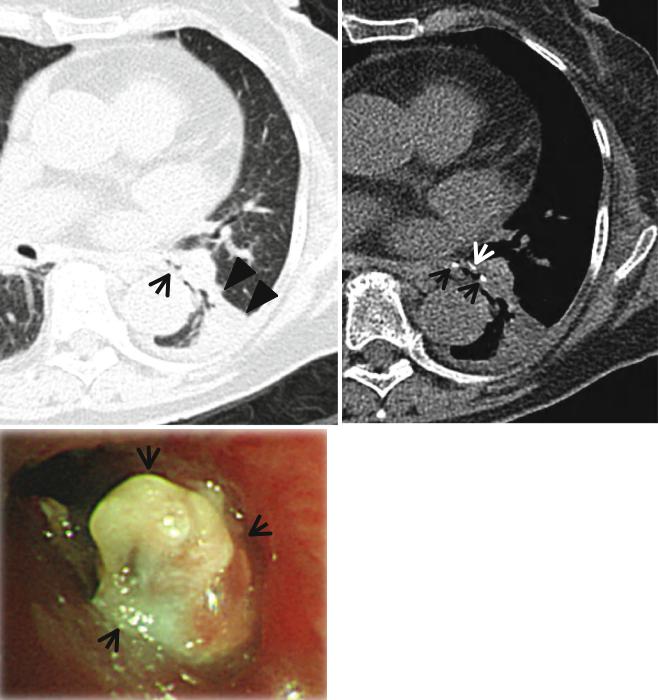
Fig. 11.3 Left upper lobar atelectasis owing to mucoepidermoid carcinoma arising from the left upper lobar bronchus in a 69-year-old woman. (a) Enhanced CT scan (2.5-mm section thickness) obtained at level of the distal left main bronchus shows an endobronchial nodule (arrow) obstructing the left upper lobar bronchus. Also note the atelectatic left upper lobe (arrowheads). (b) Coronal reformatted (2.0-mm section thickness) CT scan demonstrates endobronchial nodule (arrow)
and the atelectatic left upper lobe (arrowheads). (c) Bronchoscopy displays whitish-yellow nodule (arrows) obstructing the left upper lobar bronchus. (d) High-magnification (×100) photomicrograph of pathologic specimen obtained with left upper lobectomy discloses glandular spaces containing mucus (arrows) admixed with sheets of epidermoid cells (open arrows), diagnostic of mucoepidermoid carcinoma
Combined Atelectasis of the Right Upper and Middle Lobes |
89 |
||
|
|
|
|
Fig. 11.4 Right middle lobar |
a |
b |
|
atelectasis (right middle lobe |
|||
|
|
||
syndrome) in a 72-year-old man. |
|
|
|
(a, b) Consecutive CT scans |
|
|
|
(1.5-mm section thickness) |
|
|
|
obtained at level of the right |
|
|
|
inferior pulmonary vein show |
|
|
|
the atelectatic right middle lobe |
|
|
|
marginated by right minor |
|
|
|
(arrows) and major (arrowheads) |
|
|
|
fissures. Anterior margin (right |
|
|
|
minor fissure) of the atelectatic |
|
|
|
right middle lobe is somewhat |
|
|
|
wavy, whereas posterior margin |
|
|
|
(right major fissure) of the lobe |
|
|
|
is sharp |
|
|
|
a |
b |
|
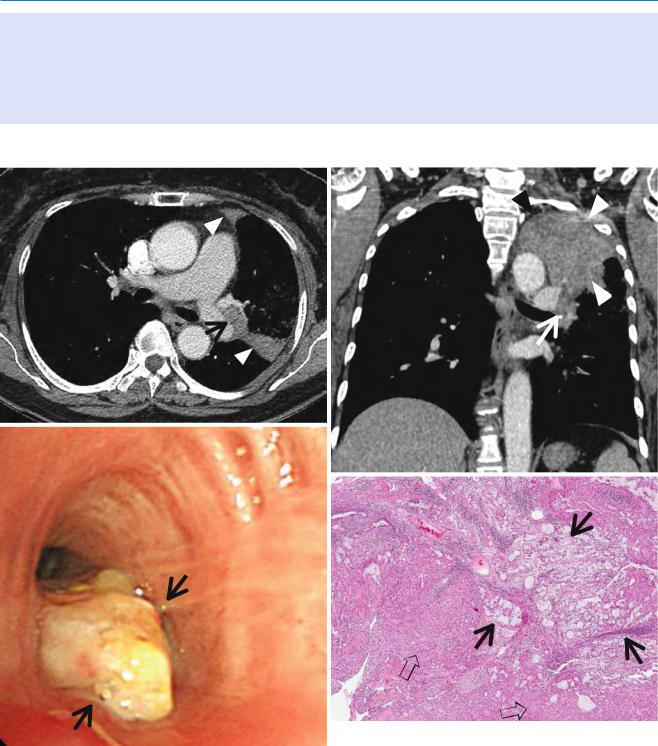
Fig. 11.5 Right lower lobar atelectasis in a 61-year-old man who has squamous cell carcinoma involving the right lower lobe. (a) Mediastinal window image of enhanced CT scan (2.5-mm section thickness) obtained at ventricular level shows low-attenuation mass (arrows) and associated right lower lobar atelectasis (enhancing area, arrowheads).
Also note right pleural effusion. (b) 18Fluorine fluorodeoxyglucose (FDG) PET demonstrates increased FDG uptake (arrows) within central bronchogenic carcinoma. The atelectatic right lower lobe surrounds the tumor
90 |
11 Lobar Atelectasis Sign |
|
|
a |
b |
c
Fig. 11.6 Left lower lobar atelectasis related to aspirated foreign body in an 82-year-old woman. (a) Lung window of CT scan (2.5-mm section thickness) obtained at the left lower lobar bronchus level shows the narrowed left lower lobar bronchus (arrow) and volume decrease of left lower lobe bounded laterally by left major fissure (arrowheads). (b) Mediastinal window image demonstrates peribronchial calcific attenuations (arrows) that are associated with left lower lobar bronchial
narrowing. (c) Bronchoscopy displays inflamed granulation tissue (arrows) obstructing the left lower lobar bronchus. (d) Lowmagnification (×4) of pathologic specimen obtained with rigid bronchoscopy discloses combination of cartilage (arrows), bone fragment (arrowhead), and necrotic tissue with bacteria (Actinomyces) (open arrows) that has caused granulation tissue obstructing left lower lobar bronchus
Combined Atelectasis of the Right Upper and Middle Lobes |
91 |
|
|
Fig. 11.6 (continued)
d
a |
b |
LUL 
RML
 RLL
RLL
d
c
RULB
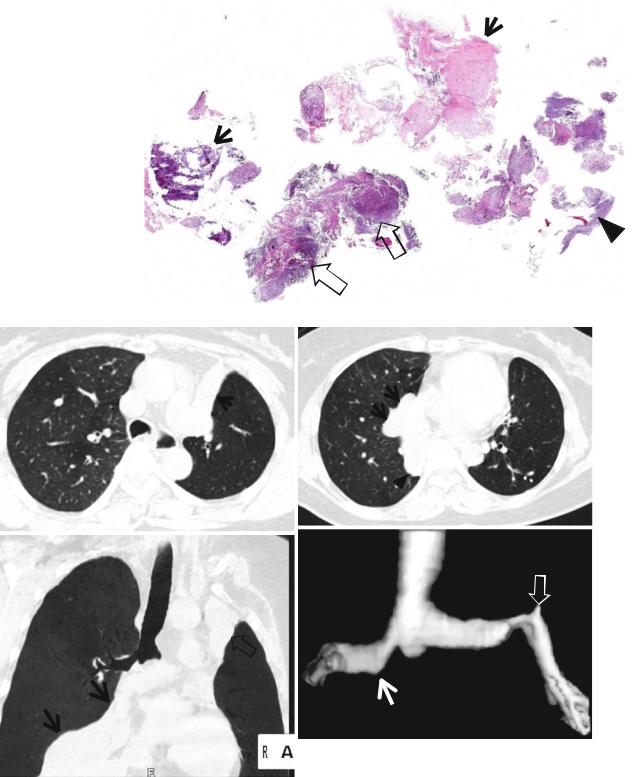
Fig. 11.7 Trilobar atelectasis involving the right middle and lower lobar bronchi and left upper lobar bronchus in a 34-year-old woman with bronchial tuberculosis, fibrotic stage. (a) Lung window of CT scan (5.0-mm section thickness) obtained at carinal level shows the atelectatic left upper lobe (arrows) marginated laterally by the elevated left lower lobe. LUL left upper lobe. (b) CT scan obtained at level of the segmental bronchi of the left lower lobe demonstrates the atelectatic right middle lobe (RML) and right lower lobe (RLL) bounded laterally by right minor (arrows) and
major (arrowheads) fissures, respectively. (c) Minimum-intensity projection (MIP) image clearly depicts the atelectatic right middle and lower lobes (arrows) and left upper lobe (open arrow). Please note the patent right upper lobar bronchus (RULB) and aerated right upper lobe filling entire right hemothorax. (d) Three-dimensional image made with shaded-surface display (SSD) technique discloses clearly obliterated bronchus intermedius (arrow) and left upper lobar bronchus (open arrow). Also note irregular narrowing of both main bronchi