

204 |
20 Ground-Glass Opacity with Reticulation |
|
|
spicuous or absent. Alveolar spaces often contain mucin. When stromal invasion is seen, the malignant cells may show less cytoplasmic mucin and more atypia. These tumors differ from mucinous adenocarcinoma in situ and minimally invasive adenocarcinoma by one or more of the following criteria: size (>3 cm in diameter), amount of invasion (>0.5 cm in thickness), multiple nodules, or lack of a circumscribed border with military spread into adjacent lung parenchyma. There is a strong tendency for multicentric, multilobar, and bilateral lung involvement, which may reßect aerogenous spread [23].
Symptoms and Signs
Most patients are asymptomatic. Cough and exertional dyspnea are the most common respiratory symptoms when it progresses diffusely to bilateral lung. Due to abundant mucin production of the cancer cells, patients with invasive mucinous adenocarcinoma can complain of copious amount of sputum, so-called bronchorrhea. Constitutional symptoms including anorexia, weight loss, and malaise may be present.
CT Findings
Diffuse nonmucinous or mucinous adenocarcinoma or AIS may be seen as three predominant patterns: GGO (4 of 38, 10 %) (Fig. 20.9), consolidation (22 of 38, 58 %), and multiple nodules (12 of 38, 32 %) [24]. When reticular attenuation is superimposed on GGO lesions, the tumor may manifest crazy-paving pattern.
CT–Pathology Comparisons
The GGO reßects the low-density intra-alveolar material (glycoprotein), whereas the superimposed reticular attenuation is due to inÞltration of the interstitium by inßammatory or tumor cells [24, 25].
Patient Prognosis
The overall prognosis for patients with invasive mucinous adenocarcinoma is worse than for those with the nonmucinous adenocarcinoma. Invasive mucinous adenocarcinoma has a strong tendency for multifocal, multilobar, and bilateral lung involvement, which may reßect aerogenous spread. Even if surgically resected in the localized stage, it frequently recurs in the remaining lung.
References
1. Remy-Jardin M, Giraud F, Remy J, Copin MC, Gosselin B, Duhamel A. Importance of ground-glass attenuation in chronic diffuse inÞltrative lung disease: pathologic-CT correlation. Radiology. 1993;189:693Ð8.
2. Hansell DM, Bankier AA, MacMahon H, McLoud TC, Muller NL, Remy J. Fleischner Society: glossary of terms for thoracic imaging. Radiology. 2008;246:697Ð722.
3. Raghu G, Collard HR, Egan JJ, et al. An ofÞcial ATS/ERS/JRS/ ALAT statement: idiopathic pulmonary Þbrosis: evidence-based guidelines for diagnosis and management. Am J Respir Crit Care Med. 2011;183:788Ð824.
4. Silva CI, Muller NL, Lynch DA, et al. Chronic hypersensitivity pneumonitis: differentiation from idiopathic pulmonary Þbrosis and nonspeciÞc interstitial pneumonia by using thin-section CT. Radiology. 2008;246:288Ð97.
5. Shin KM, Lee KS, Chung MP, et al. Prognostic determinants among clinical, thin-section CT, and histopathologic Þndings for Þbrotic idiopathic interstitial pneumonias: tertiary hospital study. Radiology. 2008;249:328Ð37.
6. Lee HY, Lee KS, Jeong YJ, et al. High-resolution CT Þndings in Þbrotic idiopathic interstitial pneumonias with little honeycombing: serial changes and prognostic implications. AJR Am J Roentgenol. 2012;199:982Ð9.
7. Johkoh T, Itoh H, Muller NL, et al. Crazy-paving appearance at thin-section CT: spectrum of disease and pathologic Þndings. Radiology. 1999;211:155Ð60.
8. Rossi SE, Erasmus JJ, Volpacchio M, Franquet T, Castiglioni T, McAdams HP. ÒCrazy-pavingÓ pattern at thin-section CT of the lungs: radiologic-pathologic overview. Radiographics. 2003;23:1509Ð19.
9. Watts JC, Chandler FW. Pneumocystis carinii pneumonitis. The nature and diagnostic signiÞcance of the methenamine silverpositive Òintracystic bodiesÓ. Am J Surg Pathol. 1985;9:744Ð51.
10.Gilroy SA, Bennett NJ. Pneumocystis pneumonia. Semin Respir Crit Care Med. 2011;32:775Ð82.
11.Kuhlman JE, Kavuru M, Fishman EK, Siegelman SS. Pneumocystis carinii pneumonia: spectrum of parenchymal CT Þndings. Radiology. 1990;175:711Ð4.
12.Boiselle PM, Crans Jr CA, Kaplan MA. The changing face of Pneumocystis carinii pneumonia in AIDS patients. AJR Am J Roentgenol. 1999;172:1301Ð9.
13.Betancourt SL, Martinez-Jimenez S, Rossi SE, Truong MT, Carrillo J, Erasmus JJ. Lipoid pneumonia: spectrum of clinical and radiologic manifestations. AJR Am J Roentgenol. 2010;194:103Ð9.
14.Marchiori E, Zanetti G, Mano CM, Hochhegger B. Exogenous lipoid pneumonia. Clinical and radiological manifestations. Respir Med. 2011;105:659Ð66.
15.Lee KS, Muller NL, Hale V, Newell Jr JD, Lynch DA, Im JG. Lipoid pneumonia: CT Þndings. J Comput Assist Tomogr. 1995;19:48Ð51.
16. Yi MS, Kim KI, Jeong YJ, Park HK, Lee MK. CT Þndings in hydrocarbon pneumonitis after diesel fuel siphonage. AJR Am J Roentgenol. 2009;193:1118Ð21.
17.Franquet T, Gimenez A, Bordes R, Rodriguez-Arias JM, Castella J. The crazy-paving pattern in exogenous lipoid pneumonia: CT-pathologic correlation. AJR Am J Roentgenol. 1998;170: 315Ð7.
18.Khan A, Agarwal R. Pulmonary alveolar proteinosis. Respir Care. 2011;56:1016Ð28.
19.Trapnell BC, Whitsett JA, Nakata K. Pulmonary alveolar proteinosis. N Engl J Med. 2003;349:2527Ð39.
20.Murch CR, Carr DH. Computed tomography appearances of pulmonary alveolar proteinosis. Clin Radiol. 1989;40:240Ð3.
References |
205 |
|
|
21.Lee KN, Levin DL, Webb WR, Chen D, Storto ML, Golden JA. Pulmonary alveolar proteinosis: high-resolution CT, chest radiographic, and functional correlations. Chest. 1997;111:989Ð95.
22.Kang EY, Grenier P, Laurent F, Muller NL. Interlobular septal thickening: patterns at high-resolution computed tomography. J Thorac Imaging. 1996;11:260Ð4.
23.Travis WD, Brambilla E, Noguchi M, et al. International association for the study of lung cancer/American thoracic society/
European respiratory society international multidisciplinary classiÞcation of lung adenocarcinoma. J Thorac Oncol. 2011;6:244Ð85.
24.Akira M, Atagi S, Kawahara M, Iuchi K, Johkoh T. High-resolution CT Þndings of diffuse bronchioloalveolar carcinoma in 38 patients. AJR Am J Roentgenol. 1999;173:1623Ð9.
25.Tan RT, Kuzo RS. High-resolution CT Þndings of mucinous bronchioloalveolar carcinoma: a case of pseudopulmonary alveolar proteinosis. AJR Am J Roentgenol. 1997;168:99Ð100.
Ground-Glass Opacity without |
21 |
Reticulation |
Ground-Glass Opacity without Reticulation, Subpleural
and Patchy Distribution
Definition
Ground-glass opacity (GGO) is caused by partial displacement of air in lung parenchyma. The opacity is caused by partial Þlling of airspaces, interstitial thickening (due to ßuid, cells, or Þbrosis) (Figs. 21.1 and 21.2), partial collapse of alveoli, and increased capillary blood volume. Without reticulation, the GGO areas usually represent active inßammatory or reversible disease state.
Diseases Causing the Pattern
Cellular nonspecific interstitial pneumonia (NSIP) (Fig. 21.1), desquamative interstitial pneumonia (DIP) (Fig. 21.2), cryptogenic organizing pneumonia (COP), and eosinophilic pneumonia (allergic lung disease) depict GGO lesions without reticulation on thin-section CT (TSCT).
Distribution
The distribution of GGO lesions in cellular NSIP is subpleural, usually without obvious upperÐlower lung zone gradient (this gradient, overt in usual interstitial pneumonia with lower lung zone predominance) [1]. In DIP, the opacity had subpleural and lower lung zone predominance [1]. In twothirds of patients, the opacity lesions in COP are distributed along the bronchovascular bundles or subpleural lungs [2]. In chronic eosinophilic pneumonia, CT shows subpleural opacity with slight upper lung zone predominance [3].
Clinical Considerations
The presence of asthma history suggests the diagnosis of eosinophilic lung disease (approximately 40 % of patients with chronic eosinophilic lung disease have asthma) [3]. In drug-induced lung disease and lung involvements of collagen vascular diseases, lung abnormalities can be assessed with pattern approach, namely NSIP, DIP, COP, and eosinophilic lung disease-like patterns [4, 5].
Key Points for Differential Diagnosis
|
|
Distribution |
|
|
|
|
|
|
|
|
|
|
|
|
|
Zones |
|
|
|
|
|
|
|
Clinical presentations |
|
|
|
Diseases |
|
U |
M |
L |
SP |
C |
R |
BV |
R |
Acute Subacute |
Chronic |
|
Others |
|
|
||||||||||||
Cellular NSIP |
|
|
+ |
+ |
+ |
+ |
|
+ |
+ |
|
+ |
|
|
DIP |
|
|
+ |
+ |
+ |
|
|
|
+ |
+ |
+ |
|
SmokersÕ lung disease |
COP |
|
|
+ |
+ |
+ |
|
|
+ |
|
+ |
+ |
|
Consolidation predominant |
CEP |
+ |
+ |
|
+ |
|
|
|
+ |
+ |
+ |
|
Consolidation predominant; |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
asthma in 40 % of patients |
Note: NSIP nonspeciÞc interstitial pneumonia, DIP desquamative interstitial pneumonia, COP cryptogenic organizing pneumonia, CEP chronic eosinophilic pneumonia, U upper, M middle, L lower, R random, SP subpleural, C central, BV bronchovascular
K.S. Lee et al., Radiology Illustrated: Chest Radiology, Radiology Illustrated, |
207 |
DOI 10.1007/978-3-642-37096-0_21, © Springer-Verlag Berlin Heidelberg 2014 |
|
208 |
21 Ground-Glass Opacity without Reticulation |
|
|
a |
b |
c |
d |
e |
f |
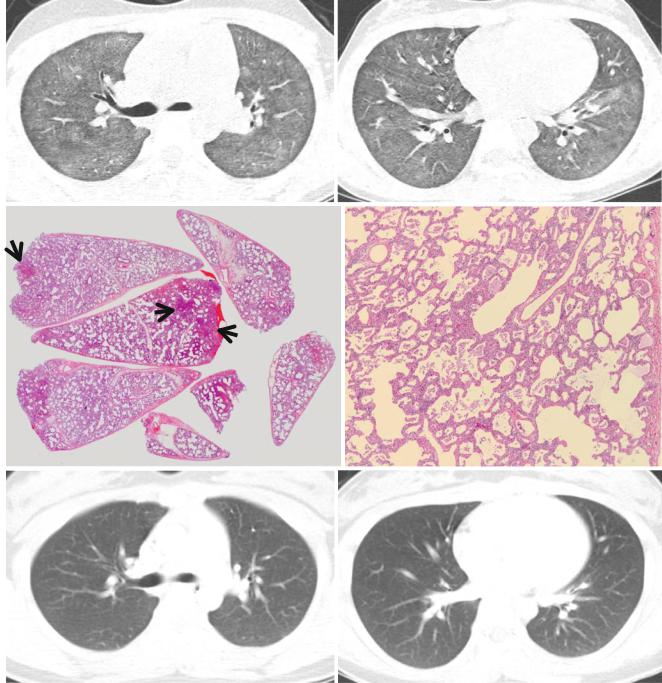
Fig. 21.1 Cellular nonspeciÞc interstitial pneumonia manifesting as diffuse ground-glass opacity without reticulation in a 10-year-old girl. (a, b) Lung window images of CT scans (2.5-mm section thickness) obtained at levels of right upper lobar bronchus (a) and inferior pulmonary veins (b), respectively, show diffuse ground-glass opacity in both lungs. (c) Low-magniÞcation (×40) photomicrograph of surgical lung biopsy specimen obtained from right lower lobe demonstrates diffuse alveolar wall thickening with inßammatory cell inÞltration. Lesions are
temporally homogeneous and uniform in alveolar wall thickening. Areas of focal organizing pneumonia (arrows) are associated. (d) HighmagniÞcation (×200) photomicrograph discloses alveolar wall thickening with chronic inßammatory cell inÞltration and mild alveolar pneumocytes hyperplasia and many intra-alveolar macrophage aggregation. (e, f) Two-year follow-up CT scans obtained at similar levels to a and b, respectively, exhibit complete disappearance of ground-glass opacity in both lungs. Patient received corticosteroid therapy
Ground-Glass Opacity without Reticulation, Subpleural and Patchy Distribution |
209 |
|
|
|
|
a |
b |
|
c |
d |
e
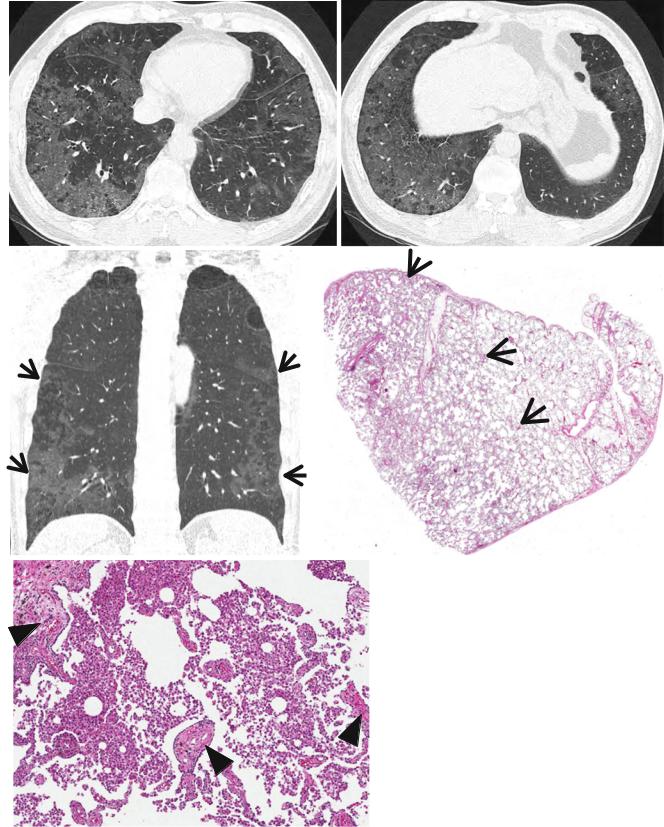
Fig. 21.2 Desquamative interstitial pneumonia presenting as patchy areas of ground-glass opacity without reticulation in a 51-year-old smoker man. (a, b) Lung window images of CT scans (1.5-mm section thickness) obtained at levels of suprahepatic inferior vena cava (a) and liver dome (b), respectively, show patchy and extensive but subpleural areas of ground-glass opacity in both lungs. (c) Coronal reformatted CT image (2.0-mm section thickness) demonstrates subpleural patchy
areas of ground-glass opacity (arrows) in both lungs. Also note bullae in upper lung zones. (d) Low-magniÞcation (×40) photomicrograph of surgical lung biopsy specimen obtained from right lower lobe exhibits areas of uniform accumulation of inßammatory cells in intra-alveolar spaces and mildly in interstitium (alveolar walls) (arrows). (e) HighmagniÞcation (×200) photomicrograph discloses intra-alveolar macrophage accumulation and mild interstitial Þbrosis (arrowheads)