

- •Contents
- •Preface to the Third Edition
- •About the Authors
- •How to Use Herbal Medicines
- •Introduction
- •General References
- •Agnus Castus
- •Agrimony
- •Alfalfa
- •Aloe Vera
- •Aloes
- •Angelica
- •Aniseed
- •Apricot
- •Arnica
- •Artichoke
- •Asafoetida
- •Avens
- •Bayberry
- •Bilberry
- •Bloodroot
- •Blue Flag
- •Bogbean
- •Boldo
- •Boneset
- •Borage
- •Broom
- •Buchu
- •Burdock
- •Burnet
- •Butterbur
- •Calamus
- •Calendula
- •Capsicum
- •Cascara
- •Cassia
- •Cat’s Claw
- •Celandine, Greater
- •Celery
- •Centaury
- •Cereus
- •Chamomile, German
- •Chamomile, Roman
- •Chaparral
- •Cinnamon
- •Clivers
- •Clove
- •Cohosh, Black
- •Cohosh, Blue
- •Cola
- •Coltsfoot
- •Comfrey
- •Corn Silk
- •Couchgrass
- •Cowslip
- •Cranberry
- •Damiana
- •Dandelion
- •Devil’s Claw
- •Drosera
- •Echinacea
- •Elder
- •Elecampane
- •Ephedra
- •Eucalyptus
- •Euphorbia
- •Evening Primrose
- •Eyebright
- •False Unicorn
- •Fenugreek
- •Feverfew
- •Figwort
- •Frangula
- •Fucus
- •Fumitory
- •Garlic
- •Gentian
- •Ginger
- •Ginkgo
- •Ginseng, Eleutherococcus
- •Ginseng, Panax
- •Golden Seal
- •Gravel Root
- •Ground Ivy
- •Guaiacum
- •Hawthorn
- •Holy Thistle
- •Hops
- •Horehound, Black
- •Horehound, White
- •Horse-chestnut
- •Horseradish
- •Hydrangea
- •Hydrocotyle
- •Ispaghula
- •Jamaica Dogwood
- •Java Tea
- •Juniper
- •Kava
- •Lady’s Slipper
- •Lemon Verbena
- •Liferoot
- •Lime Flower
- •Liquorice
- •Lobelia
- •Marshmallow
- •Meadowsweet
- •Melissa
- •Milk Thistle
- •Mistletoe
- •Motherwort
- •Myrrh
- •Nettle
- •Parsley
- •Parsley Piert
- •Passionflower
- •Pennyroyal
- •Pilewort
- •Plantain
- •Pleurisy Root
- •Pokeroot
- •Poplar
- •Prickly Ash, Northern
- •Prickly Ash, Southern
- •Pulsatilla
- •Quassia
- •Queen’s Delight
- •Raspberry
- •Red Clover
- •Rhodiola
- •Rhubarb
- •Rosemary
- •Sage
- •Sarsaparilla
- •Sassafras
- •Saw Palmetto
- •Scullcap
- •Senega
- •Senna
- •Shepherd’s Purse
- •Skunk Cabbage
- •Slippery Elm
- •Squill
- •St John’s Wort
- •Stone Root
- •Tansy
- •Thyme
- •Uva-Ursi
- •Valerian
- •Vervain
- •Wild Carrot
- •Wild Lettuce
- •Willow
- •Witch Hazel
- •Yarrow
- •Yellow Dock
- •Yucca
- •1 Potential Drug–Herb Interactions
- •4 Preparations Directory
- •5 Suppliers Directory
- •Index
Hawthorn
Summary and Pharmaceutical Comment
Hawthorn is characterised by its phenolic constituents, in particular the flavonoid components to which many of the pharmacological properties associated with hawthorn have been attributed. The phytochemistry of hawthorn fruit and hawthorn leaf with flower are, in general, qualitatively similar, although separate monographs for the fruit (berries) and leaf with flowers appear in the British Pharmacopoeia and European Pharmacopoeia.(G81, G84) Pharmacological actions documented following preclinical and clinical studies support
Hevidence is limited to preparations containing hawthorn leaf with flower.
A systematic review and meta-analysis of 13 randomised, double-blind, placebo-controlled trials of standardised extracts of hawthorn leaf and flower in patients with chronic heart failure found that the products assessed were beneficial as adjunctive treatments in patients with chronic heart failure, but there is insufficient evidence to support the use of hawthorn extract alone in the treatment of chronic heart failure. Further well-designed randomised controlled trials are necessary to confirm the findings.
Data from randomised controlled trials and post-marketing surveillance studies suggest that the hawthorn preparations assessed are well-tolerated when taken at recommended dosages. However, results cannot necessarily be extrapolated to other hawthorn products, which may differ qualitatively and quantitatively in their chemical content. Further welldesigned post-marketing surveillance studies are required to assess the safety of hawthorn extracts, including with longterm use. In view of the documented pharmacological actions of hawthorn the potential for preparations of hawthorn to interfere with other medicines administered concurrently, particularly those with similar or opposing effects, including antihypertensive, antihypotensive, and inotropic agents, should be considered. Hawthorn fruit or hawthorn leaf and
flower are contraindicated during pregnancy and breastfeeding.some of the traditional uses of hawthorn, although clinical
Species (Family)
*Crataegus laevigata (Poir.) DC. (Rosaceae)
†Crataegus monogyna Jacq.
Synonym(s)
*C. oxyacanthoides Thuill., C. oxyacantha auct.
†Crataegus oxyacantha L., nom. ambig.
Part(s) Used
Fruit, leaf, flower
Pharmacopoeial and Other Monographs
American Herbal Pharmacopoeia(G1)
BHP 1996(G9)
BP 2007(G84)
BHMA 2003(G66)
Complete German Commission E(G3)
ESCOP 2003(G76)
Martindale 35th edition(G85)
Ph Eur 2007(G81)
WHO volume 2(G70)
Legal Category (Licensed Products)
Hawthorn is not included in the GSL.(G37)
Constituents
The following is compiled from several sources, including General References G1 and G2.
Amines Phenylethylamine, O-methoxyphenethylamine and tyramine.(1)
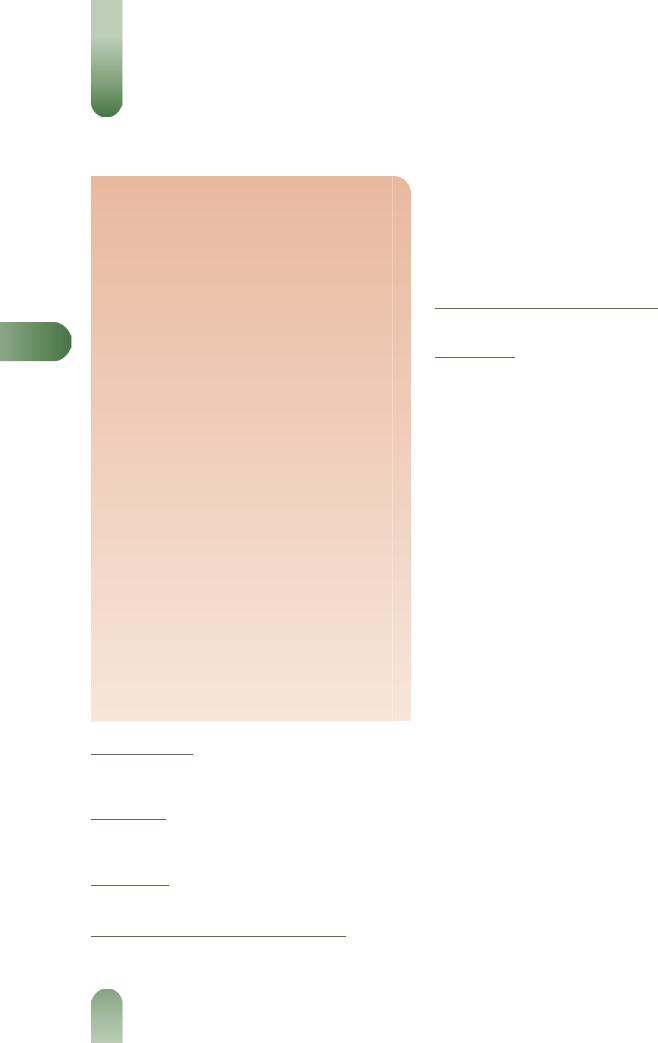
Flavonoids Up to 1%.(G81) Flavonol (e.g. kaempferol, quercetin) and flavone (e.g. apigenin, luteolin) derivatives, rutin, hyperoside, vitexin glycosides, orientin glycosides.(2–5) The fruits contain relatively more hyperoside and the leaves relatively more vitexin glycosides.(G75)
Tannins Proanthocyanins (catechin-type oligomers).(6, 7)
Other constituents Cyanogenetic glycosides and saponins.
Quality of plant material and commercial products
As with other herbal medicinal products, there can be variation in the qualitative and quantitative composition of hawthorn crude plant material and commercial preparations of hawthorn fruit and/or leaf with flower. According to the British and European Pharmacopoeias, hawthorn leaf with flower consists of the whole or cut, dried flower-bearing tops of C. laevigata or C. monogyna (or rarely certain other Crataegus species), and contains not less
than 1.5% of flavonoids, expressed as hyperoside and calculated with reference to the dried drug.(G81, G84) Detailed descriptions of
hawthorn berry and leaf with flower for use in botanical, microscopic and macroscopic identification have been published,
along with qualitative and quantitative methods for the assessment of hawthorn berry and leaf with flower raw material.(G1)
Aqueous-alcoholic (40–70% ethanol or methanol) extracts of hawthorn leaf with flower obtained from several different manufacturers were reported to have a similar profile of constituents (procyanidins, flavonoids, total vitexin and total phenols) both qualitatively and quantitatively, whereas an aqueous extract was stated to have a lower concentration of procyanidins, flavonoids and total phenols, and a similar total vitexin content.(8) However, no statistical analyses were described to support these findings and there were in fact also substantial quantitative variations between aqueous-alcoholic extracts in content of procyanidins (8.7–13.5%), flavonoids calculated as hyperoside (1.1–3.4%), vitexin-2''-O-rhamnoside and hyperoside (5.7–7.9%), total vitexins (4.1–4.9%) and total phenols (19.5–25.6%); values for these constituents for the aqueous extract were 8.0%, 0.7%, 5.6%, 4.1% and 14.0%, respectively. Further work showed that all
346
the extracts had a relaxant effect on norepinephrine (noradrena- line)-induced contractions of guineapig aortic rings in vitro, achieving relaxations of 29–44% of baseline values. EC50 (effective concentration) values were between 4.2–9.8 mg/mL for the aqueous-alcoholic extracts and 22.4 mg/mL for the aqueous extract, although maximum effects were similar for all extracts.(8) The positive control milrinone had a significantly greater effect than any of the extracts (EC50 1.3 mg/mL). Basic statistical analyses indicated that there were no statistically significant differences between the aqueous-alcoholic extracts in terms of their relaxant effects, indicating pharmacological equivalence. However, more sophisticated analysis allowing for multiple analyses indicated that the effects of the 40% ethanol and 55% methanol extracts differed significantly from those of the other aqueous-alcoholic extracts. These findings provide some support for the equivalence of 40–70% ethanol or methanol extracts of hawthorn leaf with flower,(8) although this would be strengthened by more consistent results in further studies. The equivalence of preparations of hawthorn fruit also requires investigation.
Food Use
Hawthorn is not commonly used in foods. It is listed by the Council of Europe as a natural source of food flavouring (category N2). This category indicates that hawthorn can be added to foodstuffs in small quantities, with a possible limitation of an active principle (as yet unspecified) in the final product.(G16)
Herbal Use
Hawthorn fruit is stated to possess cardiotonic, coronary vasodilator and hypotensive properties. Traditionally, it has been used for cardiac failure, myocardial weakness, paroxysmal tachycardia, hypertension, arteriosclerosis and Buerger's disea-
se.(G3, G7) The German Commission E did not approve therapeutic use of the fruit.(G3) Modern interest in hawthorn is focused on the
use of hawthorn leaf with flower in reduced cardiac performan-
ce.(G3)
Hawthorn |
347 |
Dosage
Dosages for oral administration (adults) for traditional uses recommended in older standard herbal reference texts are given below.
Fruit |
|
|
Dried fruit 0.3–1.0 g as an infusion three times daily.(G7) |
|
|
Liquid extract |
0.5–1.0 mL (1 : 1 in 25% alcohol) three times |
|
daily.(G7) |
|
|
Tincture 1–2 mL (1 : 5 in 45% alcohol) three times daily.(G7) |
|
|
Leaf with flower For the treatment of decreasing cardiac |
|
|
efficiency corresponding to functional stage II of the New York |
|
|
Heart Association 160–900 mg aqueous-alcoholic extract (ethanol |
|
|
45% v/v or methanol 70% v/v; drug to extract ratio 4–7 : 1, with |
H |
|
defined flavonoid |
and/or procyanidin content corresponding to |
|
3.5–19.8 mg flavonoids, calculated as hyperoside, and 30–168.7 mg
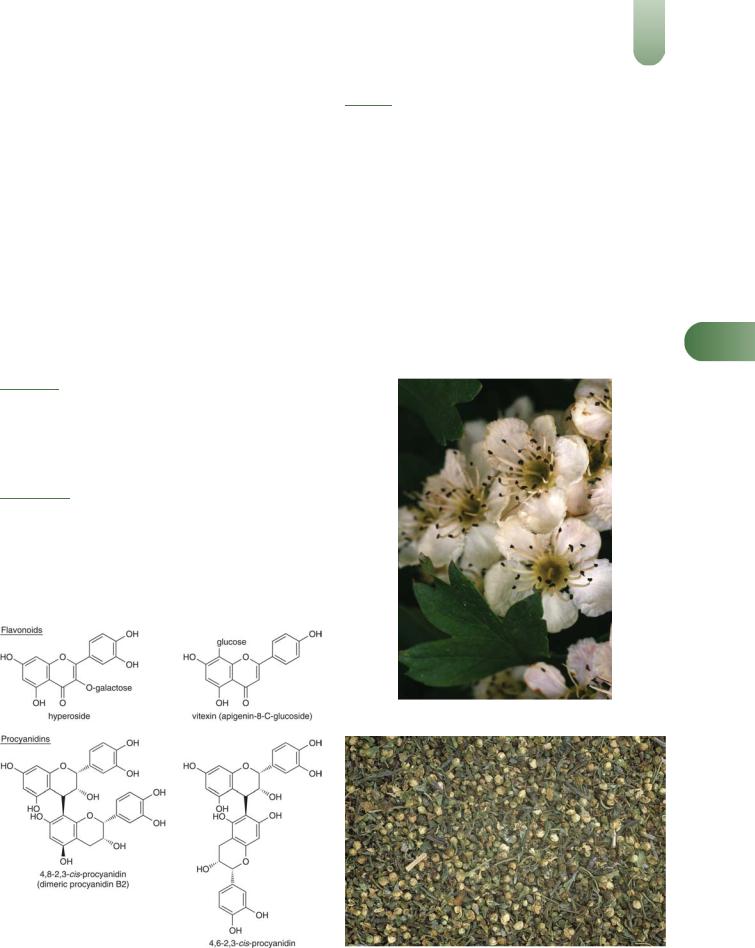
Figure 2 Hawthorn (Crataegus laevigata).
Figure 1 Selected constituents of hawthorn.
Figure 3 Hawthorn – dried drug substance (fruit and leaf).

348 Hawthorn
procyanidins, calculated as epicatechin) daily, in two to three divided doses.(G3)
Clinical trials of hawthorn leaf with flower in patients with different stages of heart failure (according to the NYHA classification) mainly have assessed the effects of a standardised extract (WS-1442, containing 18.8% oligomeric procyanidins) administered orally at doses ranging from 160–1800 mg daily for up to 16 weeks.
Pharmacological Actions
In vitro and animal studies
Pharmacokinetics There are only limited data available on the pharmacokinetics of constituents of hawthorn preparations. In male rats given an 80% ethanol extract of the fruits of C. pinnatifida Bge. var major N.E.Br. containing ( )-epicate-
Hchin15.8%, chlorogenic acid 3.4%, hyperoside 2.7% and isoquercitrin 2.0% at a dose of 220 mg/kg by intravenous injection, pharmacokinetic parameters for these compounds were (expressed as mean (standard deviation)): plasma drug concentration, 142.8 (16.2), 33.1 (6.1), 38.8 (6.0) and 26.7 (4.9), respectively;
elimination half-life (t1/2), 74.2 (10.0), 18.9 (1.8), 18.1 (1.1) and 11.1 (2.2) minutes, respectively; area under the plasma-concentra-
tion time curve (AUC), 2204.5 (261.0), 526.1 (37.4), 358.8 (18.0) and 216.0 (11.5) mg/min/mL, respectively; clearance, 16.0 (2.0), 14.3 (1.0), 16.7 (0.8) and 20.9 (1.1) mL/min/kg, respectively.(9) The plasma drug concentration, t1/2, AUC and urinary excretion were significantly higher, and the volume of distribution and total body clearance were significantly lower, following intravenous injection of the extract than following intravenous injection of the individual four compounds at doses matching those in the extract (p < 0.05 for all). Following oral administration of a similar dose of the extract and the individual compounds, only epicatechin was absorbed, and there were no statistically significant differences in its pharmacokinetic parameters after administration as part of an extract or as the pure compound. A possible explanation for these findings is that other constituents of hawthorn extract may influence the pharmacokinetics of the constituents studied.(9)
Cardiovascular activity Cardiovascular activity has been documented for hawthorn and attributed to the flavonoid components, in particular the procyanidins.
A dry ethanol (45%) extract of hawthorn leaf with flower (drug- to-extract ratio 4–6.6 : 1, standardised for oligomeric procyanidins 18.75%; WS-1442) at a dose 100 mg/kg orally by gavage daily for seven days significantly improved cardiac function and reduced infarct size in a rat model of prolonged ischaemia and reperfusion, compared with control (p < 0.05).(10) In other experiments, hawthorn extracts and/or isolated constituents increased coronary blood flow both in vitro (in the guinea-pig heart) and in vivo (in the cat, dog and rabbit), reduced blood pressure in vivo (in cat, dog, rabbit and rat models), increased (head, skeletal muscle and kidney) and reduced (skin, gastrointestinal tract) peripheral blood flow in vivo (in the dog) and reduce peripheral resistance in vivo (in the dog).(6, 11–16) The hypotensive activity of hawthorn has been attributed to a vasodilation action rather than via adrenergic, muscarinic or histaminergic receptors.(15) Beta-adrenoceptor blocking activity (versus adrenaline-induced tachycardia) has been exhibited in vivo in the dog and in vitro in the frog heart using flower, leaf and fruit extracts standardised for their procyanidin content.(6) A direct relationship was found between the concentration of procyanidin and observed actions.
Negative chronotropic and positive inotropic actions have been observed in vitro using the guinea-pig heart and attributed to flavonoid and proanthocyanidin fractions.(17) A positive inotropic effect has also been exhibited by amine constituents in vitro using guinea-pig papillary muscle.(1)
Hawthorn extracts have also been reported to lack any effect on
the heart rate and muscle contractility in studies that have observed an effect on blood pressure in the dog and rat.(14, 15)
Hawthorn extracts have exhibited some prophylactic antiarrhythmic activity in rabbits administered intravenous aconitine.(18) Extracts infused after aconitine did not affect the induced arrhythmias. In vitro, vitexin rhamnoside has been reported to have no effect on the action of ouabain and aconitine.(18) A crude extract of Crataegus pinnatifidia Bge. var major N.E.Br. and the flavonoid vitexin rhamnoside have been reported to exert a protective action on experimental ischaemic myocardium in anaesthetised dogs.(19) The extracts were observed to decrease left ventricular work, decrease the consumption of oxygen index, and increase coronary sinus blood oxygen concentrations, resulting in a decrease in oxygen consumption and balance of oxygen metabolism. In contrast to other studies, an increase in coronary blood flow was not observed. The authors attributed these opposing results to the variation in concentrations of active constituents between the different plant parts. In vitro, vitexin rhamnoside has been reported to exert a protective action towards cardiac cells deprived of oxygen and glucose.(20)
Other activities A mild CNS-depressant effect has been documented in mice that received oral administration of hawthorn flower extracts.(21) An increase in barbiturate sleeping time and a decrease in spontaneous basal motility were the most noticeable effects.
Free radicals have been linked with the ageing process. When fed to mice, a hawthorn fruit (C. pinnatifidia) extract has been reported to enhance the action of superoxide dismutase (SOD), which promotes the scavenging of free radicals.(22) An inhibition of lipid peroxidation, which can be caused by highly reactive free radicals, was also documented.(22) The pharmacological actions of leaf with flowers include increase in cardiac contractility, increase in coronary blood flow and myocardial circulation, protection from ischaemic damage and decrease of peripheral vascular resistance.(G52)
Clinical studies
Heart failure and other cardiovascular disorders Clinical trials of preparations of hawthorn mainly have assessed the effects of standardised extracts of the leaf and flower in patients with different stages of heart failure, according to the NYHA classification. There have been at least 13 randomised, doubleblind, placebo-controlled trials of hawthorn extracts involving patients with NYHA heart failure classes I to III. The results of at least ten other studies have been published, but these have assessed the effects of combination preparations of hawthorn or were not conducted according to a randomised, placebo-controlled design. Most randomised, double-blind, placebo-controlled trials have assessed the effects of a dry 45% ethanol extract of hawthorn leaves with flowers (WS-1442; drug-to-extract ratio 4–6 : 1, containing 18.8% oligomeric procyanidins). Several other trials have compared the effects of another extract of hawthorn leaf with flower (LI-132; standardised for 2.2% flavonoids) with those of placebo, or the angiotensin converting enzyme (ACE) inhibitor captopril.

A systematic review and meta-analysis included 13 randomised, double-blind, placebo-controlled trials of standardised extracts of hawthorn leaf and flower in patients with chronic heart failure. Ten trials tested the extract WS-1442 administered orally at doses ranging from 160 to 1800 mg daily for three to 16 weeks, whereas the other three trials assessed the extract LI-132 at doses of 300, 600 or 900 mg daily for four or eight weeks; in several trials, participants were also receiving concurrent standard treatments, such as diuretics, although a number of trials excluded patients who were already receiving diuretics, glycosides, calcium antagonists and ACE inhibitors, and in some studies it was not clear whether or not participants received concomitant medications.(23) Eight trials, involving a total of 632 participants, provided data that were suitable for meta-analysis. Data from four trials (n = 310 participants), which assessed maximal workload, showed that hawthorn extracts were superior to placebo (weighted mean difference (WMD), 95% confidence interval (CI): 7 Watt, 3 to 11 Watt; p < 0.01), and data from six trials which assessed the systolic blood pressure–heart rate product (systolic blood pressure in mmHg multiplied by heart rate per minute divided by 100) showed that this outcome was reduced to a greater extent in hawthorn recipients than placebo recipients (WMD, 95% CI: -20, -32 to -8). Of the five trials that were not included in the metaanalysis, three reported statistically significant effects for hawthorn extracts, compared with placebo, with respect to primary outcome measures, and two reported no statistically differences for hawthorn extracts, compared with placebo.(23)
The review concluded that hawthorn extracts are beneficial as adjunctive treatments in patients with chronic heart failure, but there is insufficient evidence to support the use of hawthorn extract alone in the treatment of chronic heart failure. Furthermore, as some of the trials did not score highly in an assessment of their methodological quality and as, overall, the studies involved relatively small numbers of patients, further welldesigned randomised controlled trials are necessary to confirm the findings. Also, the observed effects cannot necessarily be extrapolated to hawthorn preparations other than those tested in the trials described above.
The largest trial included in the meta-analysis was a randomised, double-blind, placebo-controlled trial initially involving 209 patients with chronic stable NYHA class III heart failure who received hawthorn extract WS-1442 900 or 1800 mg daily, or placebo, for 16 weeks. At the end of the study, for the 139 patients who were eligible for analysis, the maximum tolerated workload during bicycle exercise was significantly greater for the higher dose hawthorn group, compared with the placebo group (p < 0.05).(24)
In another randomised, double-blind, controlled trial, 40 patients with chronic heart failure (NYHA class II) received a combination preparation containing extracts of hawthorn and passionflower (standardised on flavone and proanthocyanidin content) 2 mL three times daily, or placebo, for 42 days.(25) Significant improvements were noted for the treatment group, compared with placebo, in exercise capacity, heart rate at rest, diastolic blood pressure during exercise, and concentrations of total plasma cholesterol and low-density lipids (p < 0.05 for each). There were no statistically significant differences between groups in maximum exercise capacity, breathlessness, and physical performance.
In a non-randomised, double-blind, controlled trial, the effects of a standardised extract of hawthorn leaf and flower (LI-132) 900 mg daily were compared with those of the ACE inhibitor
captopril 37.5 mg daily for |
eight weeks in |
132 patients |
with |
chronic stable NYHA class |
II heart failure. |
During the |
study, |
Hawthorn |
349 |
|
exercise tolerance increased significantly in both groups, com- |
|
|
pared with baseline values (p < 0.001), and the blood pressure– |
|
|
heart rate product and incidence and severity of symptoms |
|
|
decreased in both groups; there were no statistically significant |
|
|
differences between the groups.(26) |
|
|
The effectiveness (i.e. effects when used in general practice) of a |
|
|
hawthorn extract (WS-1442) were assessed in a prospective, non- |
|
|
interventional, cohort study involving 952 patients with heart |
|
|
failure (NYHA class II). Of these, 588 patients received the |
|
|
hawthorn extract either alone or in addition to standard |
|
|
treatment, and 364 patients received standard treatment alone. |
|
|
Interim results for 533 patients from whom 130 pairs of patients |
|
|
matched for certain cardiac and demographic characteristics at |
|
|
baseline suggested that fatigue (p = 0.036), stress dyspnoea (p = |
|
|
0.020) and, marginally, palpitations (p = 0.048) were significantly |
|
|
less marked in the hawthorn extract cohort than in the |
|
|
comparative cohort.(27) However, final results of the study are |
|
|
required before conclusions can be drawn. |
|
H |
A preliminary randomised, double-blind, placebo-controlled |
||
trial assessed the effects of a hawthorn extract 500 mg daily, alone and in combination with a magnesium supplement 600 mg daily, for ten weeks in 36 patients with mild hypertension. Reductions in systolic and diastolic blood pressure were observed in all groups, and there were no statistically significant differences between groups.(28) However, it is possible that as the study involved only small numbers of participants that it did not have adequate statistical power to detect any differences between groups.
Data pooled from two randomised, controlled, crossover studies each involving 24 participants with orthostatic dysregulation who received one of three doses of an oral combination preparation containing an ethanol extract of hawthorn berries, D- camphor and menthol on four separate days indicated a statistically significant effect for higher dose of the combination preparation, compared with placebo, with respect to mean arterial pressure, and systolic and diastolic blood pressure.(29)
Other conditions The effects of a combination preparation containing C. oxyacantha, Eschscholtzia californica and magnesium were assessed in a randomised, double-blind, placebocontrolled trial involving 264 participants with mild-to-moderate anxiety disorders with associated functional disturbances. Participants received the combination preparation (n = 130), or placebo (n = 134), two tablets twice daily for three months. At the end of the study, reductions in Hamilton anxiety scale scores were
significantly greater for the treatment group than for the placebo group.(30)
Side-effects, Toxicity
Clinical data
Data from randomised controlled trials and post-marketing surveillance studies suggest that hawthorn preparations are welltolerated when taken at recommended dosages. While these studies provide some useful data for the hawthorn products assessed, their results cannot necessarily be extrapolated to other manufacturers' hawthorn products, which may differ qualitatively and quantitatively in their chemical content. In addition, clinical trials are designed primarily to assess efficacy, not safety, and have the statistical power only to detect common, acute adverse effects. Further well-designed post-marketing surveillance studies are required to assess the safety of hawthorn extracts, including with long-term use.
350 Hawthorn
A systematic review and meta-analysis included 13 randomised, double-blind, placebo-controlled trials of standardised extracts of hawthorn leaf and flower in patients with chronic heart failure (see Pharmacological Actions, Clinical studies), of which 12 trials reported data on adverse events. Of these, nine trials tested the extract WS-1442 administered orally at doses ranging from 160– 1800 mg daily for three to 16 weeks, whereas the other three trials assessed the extract LI-132 at doses of 300, 600 or 900 mg daily for four or eight weeks.(23) The systematic review reported that in five trials no adverse events occurred in the hawthorn groups and that in the seven other trials, 39 adverse events, most commonly, dizziness/vertigo (n = 8 cases), occurred among around 300 hawthorn recipients. However, the review did not state whether or not the number and type of adverse events occurring in the hawthorn groups were different to those for the placebo groups. In the largest trial included in the systematic review, the frequency of
dizziness was lower in the higher dose hawthorn group than in the
(24)
HIn two post-marketing surveillance studies involving over 4500lower dose hawthorn and placebo groups.
patients with NYHA class I or II heart failure who received hawthorn extract (WS-1442(31)) 900 mg daily for eight or 24 weeks, adverse events were reported by 1.3%(32) and 1.4%(31) of
participants. Adverse events reported included hot flushes,
stomach complaints, palpitations, dizziness, dyspnoea, headache and epistaxis.(32)
Preclinical data
General symptoms of acute toxicity observed in a number of animal models (e.g. guinea-pig, frog, tortoise, cat, rabbit, rat) have been documented as bradycardia and respiratory depression leading to cardiac arrest and respiratory paralysis.(11–13) Acute toxicity (LD50) of isolated constituents (mainly flavonoids) has been documented as 50–2600 mg/kg (by intravenous injection) and 6 g/kg (by mouth) in various animal preparations.(11–13) The documented acute toxicity of commercial hawthorn preparations has also been reviewed.(11–13)
Contra-indications, Warnings
In view of the nature of the actions documented for hawthorn, there is a view that preparations of hawthorn berries and leaves with flowers are not suitable for self-medication.
Drug interactions In view of the documented pharmacological actions of hawthorn, the potential for preparations of hawthorn to interfere with other medicines administered concurrently, particularly those with similar or opposing effects, including antihypertensive, antihypotensive, and inotropic agents, should be considered.
In an open-label, randomised, crossover study involving healthy volunteers who received digoxin 0.25 mg for ten days and digoxin 0.25 mg in addition to an extract of hawthorn leaves and flowers (WS-1442) 450 mg twice daily (equivalent to 168.6 mg oligomeric procyanidins) for three weeks with a three-week wash-out period, there were no statistically significant differences between digoxin alone and digoxin plus hawthorn extract in any of the measured pharmacokinetic parameters.(33) Digoxin concentrations were lower in the digoxin plus hawthorn group and, although this did not reach statistical significance (p = 0.054), it is possible that the study did not have sufficient statistical power to detect a difference. Furthermore, the study involved healthy volunteers, and the effects of co-administration of digoxin and hawthorn extract in patients with heart failure requires investigation.
Pregnancy and lactation Certain hawthorn extracts exhibit activity on uterine tissue (reductions in tone and motility) in vitro and in vivo (animals).(11–13) The clinical relevance of these findings is not known. In view of the these and other pharmacological activities described for hawthorn, together with the lack of information on the use of hawthorn during pregnancy and breastfeeding, preparations containing hawthorn fruit or hawthorn leaf and flower are contra-indicated during these periods.
Preparations
Proprietary single-ingredient preparations
Austria: Bericard; Crataegan; Crataegutt. Brazil: Dekatin. Chile: Cratenox. Czech Republic: Caj z Hlohu; Cardiplant; Hloh-List S. France: Aubeline; Cardiocalm; Spasmosedine. Germany: Ardeycordal mono; Basticrat; Born; Chronocard N; Cordapur Novo; Corocrat; Craegium; Cratae-Loges; Crataegutt; Crataegysat F; Crataepas; Esbericard novo; Faros; Kneipp Pflanzen-Dragees Weissdorn; Koro-Nyhadin; Kytta-Cor; Lomacard; Natucor; Orthangin novo; Oxacant-mono; Reg- ulacor-POS; Senicor; Steicorton; Stenocrat mono. Hungary: Crataegutt. Russia: Novo-Passit (Ново-Пассит). Switzerland: Cardiplant; Crataegisan; Crataegitan; Faros; Vitacor.
Proprietary multi-ingredient preparations
Argentina: Hepatodirectol; Passacanthine; Sequals G. Australia: Asa Tones; Bioglan Bioage Peripheral; Coleus Complex; Dan Shen Compound; For Peripheral Circulation Herbal Plus Formula 5; Gingo A; Ginkgo Biloba Plus; Ginkgo Complex; Lifechange Circulation Aid; Lifesystem Herbal Formula 6 For Peripheral Circulation; Multi-Vitamin Day & Night. Austria: Omega; Rutiviscal; Virgilocard; Wechseltee St Severin. Belgium: Natudor; Sedinal; Seneuval. Brazil: Calman; Calmazin; Calmiplan; Floriny; Pasalix; Passi Catha; Passiflora Composta; Passiflorine; Sedalin; Serenus; Sominex. Chile: Armonyl. Czech Republic: Alvisan Neo; Fytokliman Planta; Hertzund Kreislauftee; Hypotonicka; Novo-Passit; Valofyt Neo. France: Biocarde; Euphytose; Mediflor Tisane Calmante Troubles du Sommeil No 14; Mediflor Tisane Circulation du Sang No 12; Natudor; Neuroflorine; Nicoprive; Nocvalene; Passiflorine; Passinevryl; Quinisedine; Sedatif Tiber; Sedopal; Spasmine; Sympaneurol; Sympathyl; Sympavagol; Tranquital; Vagostabyl. Germany: Antihypertonicum S; Biovital Aktiv; Biovital Aktiv; Biovital Classic; Bomacorin; Cardio-Longoral; Chlorophyl liquid "Schuh"; Convallocor-SL; Convastabil; Fovysat; Gin- seng-Complex "Schuh"; Ilja Rogoff; Korodin; Oxacant-sedativ; Passin; Protecor; Salus Herz-Schutz-Kapseln; Septacord; Tornix. Hungary: Biovital; Biovital. Israel: Nerven-Dragees; Passiflora. Italy: Anevrasi; Lenicalm; Noctis; Parvisedil; Passiflorine; Sedatol; Sedatol; Sedofit; Sedopuer F. Mexico: Ifupasil. Monaco: Neuropax. Portugal: Neurocardol. Russia: Doppelherz Vitalotonik (Доппельгерц Виталотоник); Herbion Drops for the Heart (Гербион Сердечные Капли). Spain:
Natusor High Blood Pressure; Natusor Somnisedan; Passiflorine; Sedasor; Sedonat; Tensiben. Switzerland: Arterosan Plus; Cardiaforce; Circulan; Dragees pour le coeur et les nerfs; Dragees sedatives Dr Welti; Ipasin; Phytomed Cardio; Strath Gouttes pour le coeur; Tisane pour le coeur et la circulation; Triallin; Valverde Coeur. UK: Tranquil. Venezuela: Cratex; Equaliv; Eufytose; Pasidor; Pasifluidina; Passiflorum. USA: Heart Health; My Favorite Multiple.

References
1 Wagner H, Grevel J. Cardioactive drugs IV. Cardiotonic amines from
Crataegus oxyacantha. Plant Med 1982; 45: 99–101.
2Nikolov N et al. New flavonoid glycosides from Crataegus monogyna and Crataegus pentagyna. Planta Med 1982; 44: 50–53.
3 Ficarra P et al. High-performance liquid chromatography of flavonoids in Crataegus oxyacantha L. Il Farmaco Ed Pr 1984; 39: 148–157.
4Ficcara P et al. Analysis of 2-phenyl-chromon derivatives and chlorogenic acid. II – High-performance thin layer chromatography and high-performance liquid chromatography in flowers, leaves and buds extractives of Crataegus oxyacantha L. Il Farmaco Ed Pr 1984;
39: 342–354.
5Pietta P et al. Isocratic liquid chormatographic method for the simultaneous determination of Passiflora incarnata L. and Crataegus
monogyna flavonoids in drugs. J Chromatogr 1986; 357: 233–238.
6Rácz-Kotilla E et al. Hypotensive and beta-blocking effect of procyanidins of Crataegus monogyna. Planta Med 1980; 39: 239.
7Vanhaelen M, Vanhaelen-Fastre R. TLC-densitometric determination of 2,3-cis-procyanidin monomer and oligomers from hawthorn (Crataegus laevigata and C. monogyna). J Pharm Biomed Anal 1989;
7: 1871–1875.
8Vierling W et al. Investigation of the pharmaceutical and pharmacological equivalence of different hawthorn extracts.
Phytomedicine 2003; 10: 8–16.
9Chang Q et al. Comparison of the pharmacokinetics of hawthorn phenolics in extract versus individual pure compound. J Clin
Pharmacol 2005; 45: 106–112.
10Veveris M et al. Crataegus special extract WS1 1442 improves cardiac function and reduces infarct size in a rat model of prolonged coronary ischemia and reperfusion. Life Sci 2004; 74: 1945–1955.
11Ammon HPT, Händel M. Crataegus, toxicology and pharmacology. Part I: Toxicity. Planta Med 1981; 43: 105–120.
12Ammon HPT, Händel M. Crataegus, toxicology and pharmacology. Part II: Pharmacodynamics. Planta Med 1981; 43: 209–239.
13Ammon HPT, Händel M. Crataegus, toxicology and pharmacology. Part III: Pharmacodynamics and pharmacokinetics. Planta Med 1981; 43: 313–322.
14Lièvre M et al. Assessment in the anesthetized dog of the cardiovascular effects of a pure extract (hyperoside) from hawthorn. Ann Pharm Fr 1985; 43: 471–477.
15Abdul-Ghani A-S et al. Hypotensive effect of Crateagus oxyacantha.
Int J Crude Drug Res 1987; 25: 216–220.
16Petkov V. Plants with hypotensive, antiatheromatous and coronarodilatating action. Am J Chin Med 1979; 7: 197–236.
17Leukel A et al. Studies on the activity of Crataegus compounds upon the isolated guinea pig heart. Planta Med 1986; 52: 65.
18Thompson EB et al. Preliminary study of potential antiarrhythmic effects of Crataegus monogyna. J Pharm Sci 1974; 63: 1936–1937.
|
Hawthorn |
351 |
19 |
Lianda L et al. Studies on hawthorn and its active principle. I. Effect |
|
|
on myocardial ischemia and hemodynamics in dogs. J Trad Chin Med |
|
|
1984; 4: 283–288. |
|
20 |
Lianda L et al. Studies on hawthorn and its active principle. II. Effects |
|
|
on cultured rat heart cells deprived of oxygen and glucose. J Trad Chin |
|
|
Med 1984; 4: 289–292. |
|
21 |
Della Loggia R et al. Depressive effect of Crataegus oxyacantha L. on |
|
|
central nervous system in mice. Sci Pharm 1983; 51: 319–324. |
|
22 |
Dai Y-R et al. Effect of extracts of some medicinal plants on |
|
|
superoxide dismutase activity in mice. Planta Med 1987; 53: 309–310. |
|
23 |
Pittler MH, et al. Hawthorn extract for treating chronic heart failure: |
|
|
meta-analysis of randomized trials. Am J Med 2003; 114: 665–674. |
|
24 |
Tauchert M. Efficacy and safety of crataegus extract WS1 1442 in |
|
|
comparison with placebo in patients with chronic stable New York |
|
|
Heart Association class-III heart failure. Am Heart J 2002; 143: 910– |
|
|
915. |
|
25 |
von Eiff M et al. Hawthorn/Passionflower extract and improvement in |
|
|
physical exercise capacity of patients with dyspnoea Class II of the |
|
|
NYHM functional classification. Acta Ther 1994; 20: 47–66. |
|
26 |
Tauchert M et al. [Effectiveness of the hawthorn extract LI 132 |
|
|
compared with the ACE inhibitor captopril. Multicentre, double-blind |
|
study in 132 patients with NYHA stage II cardiac insufficiency]. |
H |
|
Münch Med Wochenschr 1994; 136 (Suppl. Suppl.1):S27–S33 |
||
|
||
[German]. |
|
27Habs M. Prospective, comparative cohort studies and their
contribution to the benefit assessments of therapeutic options: heart failure treatment with and without hawthorn special extract WS1
1442. Forsch Komplementärmed Klass Naturheilkd 2004; 11 (Suppl. Suppl.1): 36–39.
28Walker AF Promising hypotensive effect of hawthorn extract: a randomized, double-blind, pilot study of mild essential hypertension.
Phytotherapy Res 2002; 16: 48–54.
29Belz GG et al. Camphor-Crataegus berry extract combination dosedependently reduces tilt induced fall in blood pressure in orthostatic hypotension. Phytomedicine 2002; 9: 581–588.
30Hanus M, et al. Double-blind, randomised, placebo-controlled study to evaluate the efficacy and safety of a fixed combination containing two plant extracts (Crataegus oxyacantha and Eschscholtzia californica) and magnesium in mild-to-moderate anxiety disorders.
Curr Med Res Opinion 2004; 20(1): 63–71.
31Tauchert M et al.. High-dose crataegus (hawthorn) extract WS1 1442 in the treatment of NYHA stage II heart failure. Herz 1999; 24: 465– 474.
32Schmidt U, et al. High dosed therapy with crataegus extract in patients suffering from heart failure NYHA stage I and II. Z Phytother 1998; 19: 22–30.
33Tankanow R, et al. Interaction study between digoxin and a preparation of hawthorn (Crataegus oxyacantha). J Clin Pharmacol
2003; 43: 637–642.