


CHAPTER 13
Intracellular Signaling Pathways
in Parkinson’s Disease
MONICA SANCHEZ CONTRERAS AND FERNANDO CARDOZO-PELAEZ*
Dept. of Biomedical and Pharmaceutical Sciences (BMED), Skaggs School of Pharmacy, Center for Structural and Functional Neuroscience (CSFN), The University of Montana, Missoula, Montana 59812-1552, USA
13.1 Introduction
Parkinson’s disease (PD) is a neurodegenerative condition characterized by insidious onset of bradykinesia, rigidity and resting tremor that respond to a dopamine mimetic agent.1 Clinical manifestations are correlated to a progressive degeneration of dopaminergic neurons in the pars compacta region of the substantia nigra (SN) and the resulting loss of striatal dopamine.2
The etiology of PD appears to be multi-factorial involving a chronic, progressive process that ultimately leads to dopaminergic neuronal death. The initiating event or events that trigger the beginning of the disease remain unknown. However, most data support a shared role for environmental and genetic factors. The events involved throughout the initiation of the disease until the selective dopaminergic neuronal death occurs are diverse, involving damage to cell components, abnormal organelle function and activation or inhibition of signaling pathways. Research done in this area has used di erent approaches including cell tissue exposure protocols and animal models as well as human genetics. The variation in experimental conditions and inconsistent results when comparing studies adds complexity to our understanding
RSC Drug Discovery Series No. 10 Extracellular and Intracellular Signaling
Edited by James D. Adams, Jr. and Keith K. Parker r Royal Society of Chemistry 2011
Published by the Royal Society of Chemistry, www.rsc.org
247
248 |
Chapter 13 |
of the disease. The role of some signaling pathways and signaling components in the neurodegenerative process have been clearly defined and are consistently reported, while the role(s) of others are still to be clarified. Additionally, it has been suggested that some signaling pathways experience cross-talking as well as non-exclusive activation and an overlapping of functions. Studying these signaling processes involved in dopaminergic neuronal death is important in order to elucidate how PD starts and how it progresses as well as to develop therapeutic interventions.
13.2 Selective Dopaminergic Neuronal Death
Neuronal cells, particularly dopaminergic neurons, are generally at a higher risk of injury and death than cells in other tissues. Dopaminergic neurons and some other neuronal populations in the central nervous system (CNS) show a di erential sensitivity to stress.3 Some findings o er an explanation to this particular susceptibility. It has been proposed that dopaminergic neurons in the SN need to have a rigorous control of the balance between their high metabolic needs and their high production of metabolic by-products. Additional metabolic loads, genetic deficiencies and aging may a ect this balance leading to these cells becoming less tolerant and consequently premature cell death.
A significant loss of mitochondrial complex I activity is found in PD patients and it has been proposed to result in a lowered threshold for oxidative damage4 (see Figure 13.1). In support of this, animal and cellular models generated by exposure to exogenous mitochondrial complex I inhibitors such as 1-methyl- 4-phenylpyridinium (MPP1), Paraquat and Rotenone induce phenotypes resembling those of typical PD, including selective dopaminergic neuron death. Since mitochondrial complex I impacts respiratory chain function, its inhibition induces superoxide radical leakage from the mitochondria into the cytosol as well as decreases NADH and ATP production. As a mechanism for bu ering the superoxide radicals from the cytosol, superoxide dismutases catalyze the dismutation of superoxide radical to hydrogen peroxide, which can be converted to the highly reactive hydroxyl radical.5 Reactions involving transition metal ions, such as the Fenton reaction, could be facilitated in dopaminergic neurons given the high levels of free iron and copper in the SN.6 Superoxide anion, hydrogen peroxide and hydroxyl radical are all reactive oxygen species (ROS), which induce a variety of oxidative lesions when they react with cell components. Under excessive production of ROS, there is a greater chance that these species react with cell components giving rise to oxidative stress.
In addition to the impairment of complex I function, di erent processes that take place in dopaminergic cells can lead to oxidative stress. Endogenous dopamine and its oxidation may be causal factors in the pathogenesis of PD7 (see Figure 13.2). Dopamine is easily auto-oxidized at physiological pH. Therefore, oxidation is normally prevented through storage in synaptic vesicles where acidic conditions are maintained. During stressful conditions, excessive dopamine turnover can result in extravesicular pools that are oxidized or
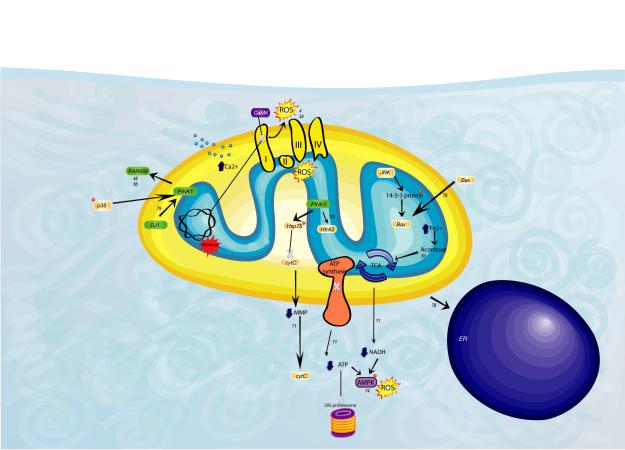
Figure 13.1 Graphic representation of pathological events in the mitochondria in PD and PD models. ROS ¼ reactive oxygen species. I, II, III, IV ¼components of the respiratory chain complex, MMP ¼mitochondrial membrane potential, CytC ¼ cytochrome C, ER ¼endoplasmic reticulum.
Disease Parkinson’s in Pathways Signaling Intracellular
249

250 |
Chapter 13 |

Intracellular Signaling Pathways in Parkinson’s Disease |
251 |
metabolized.8 Also mutations in PD-related genes interfere with normal incorporation of dopamine into synaptic vesicles.9 Oxidation of dopamine causes the production of ROS and oxidized intermediates such as 6-hydro- xydopamine (6-OHDA)10 and leukoaminochrome-o-semiquinone radical.11 Used as a PD model, exposure to 6-OHDA causes cell death of dopaminergic neurons by an increase in intracellular oxidants,7,12 while another intermediate, neuromelanin, may have a protective role in the disease.8,13 Increased extravesicular dopamine induces activity of monoamine oxidase (MAO), an enzyme important for metabolizing monoamines. The activity of MAO is coupled to the production of hydrogen peroxide at the mitochondrial outer membrane.4 Despite the evidence supporting dopamine auto-oxidation as a causal factor, dopaminergic neurons in the ventral tegmental area (VTA), also an important dopaminergic cell population in the midbrain, do not show the same vulnerability as cells in the SN. Nigral dopaminergic neurons show a di erential proteomic profiling compared to VTA dopaminergic neurons such as a higher expression of antioxidant genes, suggesting a high intrinsic oxidative stress status.3
Loss of balance in other processes in dopaminergic neurons may overwhelm normalcell function and result in cell stress and death. Abnormal protein processing is a significant observation in PD. Lewy bodies (LBs), a pathologic hallmark in PD, are intracytoplasmatic formations composed mainly of ubiquitinated proteins and a-synuclein. MPP1 and 6-OHDA can induce abnormal processing of a-synuclein, proteasomal dysfunction and cell death14 (see Figure 13.3). In a juvenile autosomal recessive form of PD, LBs are not found. Alternatively, it has been described as an accumulation of a di erent protein, Pael-R, which implicates a susceptibility to abnormal protein processing in these patients. Interestingly, there is an increased expression of Pael-R gene in dopaminergic neurons in the SN.15
Dopaminergic cells are at a higher risk of Ca21 imbalance, which results in activation of signaling pathways, increased DA synthesis and production of ROS. Increased intracellular Ca21 levels could be the result of increased extracellular Ca21 influx, decreased Ca21 excretion from the cell or deregulated Ca21 transport through organelle membranes. Evidence has been presented showing that Ca21 influx into the neuron can be responsible for their high susceptibility to cell death. Two Ca21 channels have been associated with high
Figure 13.2 Graphic representation of pathological events in PD. Findings from PD a ected individuals and from in vitro and in vivo studies on PD-related genes are included. ROS ¼ reactive oxygen species, NMDA receptor ¼N-methyl D-aspartate glutamate receptor, Nrf2 ¼nuclear factor erythroid 2-related factor, HO-1 ¼hemeoxygenase, Pael-R ¼ Parkin-associated endothelin- receptor-like receptor, CaM ¼calmodulin, CaMK ¼Ca21-calmodulin- dependent protein kinase, PKC ¼protein kinase C, PLC ¼phospholipase C, DAG ¼diacylglycerol, PIP2 ¼phosphatidyl inositol-bisphosphate, PI3K ¼ phosphatidylinositol 3-kinase, Akt ¼ v-akt murine thymoma viral oncogene homologue or protein kinase B, PDK1 ¼phosphoinositidedependent kinase 1, TH ¼tyrosine hydroxylase, DA ¼dopamine, 6OHDA ¼6-hydroxy-dopamine, PKA ¼protein kinase A, cdk ¼ cyclindependent kinases, pRb ¼retinoblastoma protein, ER ¼endoplasmic reticulum, LB ¼Lewy body.

252 |
Chapter 13 |

Intracellular Signaling Pathways in Parkinson’s Disease |
253 |
dopaminergic susceptibility, L-type Ca21 channels and glutamate receptors. L-type Ca21 channels are voltage-gated ion channels involved in the autonomous pacemaker activity in dopaminergic neurons in the SN.16 Even though this pacemaker activity involves the function of multiple ion channels, it is the L-type Ca21 channel activation that involves frequently elevated intracellular Ca21 levels17–19 (Figure 13.1). N-methyl D-aspartate (NMDA) glutamate receptors are both ligand-gated and voltage-gated receptors. NMDA receptors are non-specific cationic channels that allow the passage of Ca21 into the cell in response to glutamate binding. Dopaminergic neurons in the SN could be more vulnerable to glutamate stimulation through NMDA receptors as their subunit composition is predominantly NR1/NR2B/NR2D.20,21 NR2D subunits are characteristic of dopaminergic neurons of the SN pars compacta and mainly determine the functional diversity of NMDA receptors.22 Upon glutamate stimulation, individual NR2D subunits activate intracellular pathways that are not activated in non-dopaminergic neurons. Additionally, during the course of PD, decreased inhibition from nigral inputs to the striatum may induce an overstimulating striatal feedback on nigral dopaminergic cells. Continuous exposure to low concentrations of glutamate through striatal inputs decreases the number of viable dopaminergic neurons in rat-derived mesencephalic neurons.7 The finding that inhibition of glutamate transporters and the resulting increase in extracellular glutamate have toxic e ects on dopaminergic neurons23 and the protective e ects of NMDA receptor antagonists to MPTP and 6-OHDA24 further supports the role of glutamate in selective dopaminergic neuronal toxicity.
The previously described mechanisms account in part for the inherent susceptibility of dopaminergic cells to death; however, genetic and epigenetic factors may explain inter-individual and phenotypic variations of the disease. Genetic mutations associated to familiar PD could mediate the susceptibility of these cells to damage. Mutations and gene variations are the cause of familial PD and explain up to 10% of the cases.25 Mutations in a-synuclein gene (PARK1) have been linked to autosomal dominant PD26,27 and are associated with abnormal a- synuclein processing (Figure 13.2). Mutations in parkin gene (PARK2) result in loss of proteasomal function and are found in autosomal recessive early-onset cases.28 Mutations in DJ1 (PARK7) and PINK1 (PARK6) genes are associated with early-onset familial PD and have been linked to a higher susceptibility to
Figure 13.3 Graphic representation of pathological events in toxicant-based PD models. Findings from in vitro and in vivo PD models using MPTP, Paraquat, Rotenone and 6OH-DA are included. ROS ¼ reactive oxygen species, NMDA receptor ¼N-methyl D-aspartate glutamate receptor,
Nrf2 ¼nuclear |
factor |
erythroid |
2-related factor, GCL ¼glutamate |
|
cysteine ligase, |
PKC ¼ protein |
kinase C, |
PLC ¼ phospholipase C, |
|
DAG ¼diacylglycerol, |
PIP2 ¼ phosphatidyl |
inositol-bisphosphate, |
||
PI3K ¼phosphatidylinositol 3-kinase, Akt ¼ v-akt murine thymoma viral oncogene homologue or protein kinase B, PDK1 ¼ phosphoinositidedependent kinase 1, DA ¼dopamine, 6OH-DA ¼ 6-hydroxy-dopamine, PKA ¼ protein kinase A, cdk ¼cyclin-dependent kinases, pRb ¼retinoblastoma protein, ER ¼ endoplasmic reticulum, LB ¼Lewy body.