

Полезные материалы за все 6 курсов / Учебники, методички, pdf / Kaplan Pediatrics USMLE 2CK 2021
.pdfUSMLE Step 2 CK λ Pediatrics
Developmental Evaluation
•Thorough history and physical
•Developmental testing—age-appropriate motor, visual, cognitive, language, behavioral and learning
•Denver II Developmental Assessment
–Tool for screening the apparently normal child between ages 0–6
–Suggested at every well-child care visit
–Allows generalist to identify possible delay → need further evaluation for definitive diagnosis
–Screens in gross motor, fine motor, language, personal-social
–For infants born <38 weeks’ gestation, correct age for prematurity up to age 2 years
–Failure is at least 2 delays
PRIMITIVE REFLEXES AND DEVELOPMENTAL MILESTONES
An infant can sit up with its back straight, has started crawling, has a pincer grasp, and plays peek-a-boo. What age is most appropriate for this baby?
•Appear and disappear in sequence during specific periods of development
•Absence or persistence beyond a given time frame signifies CNS dysfunction
Included here are the major milestones indicative of specific ages. Exam questions typically describe an infant’s/child’s skills and ask for the corresponding age.
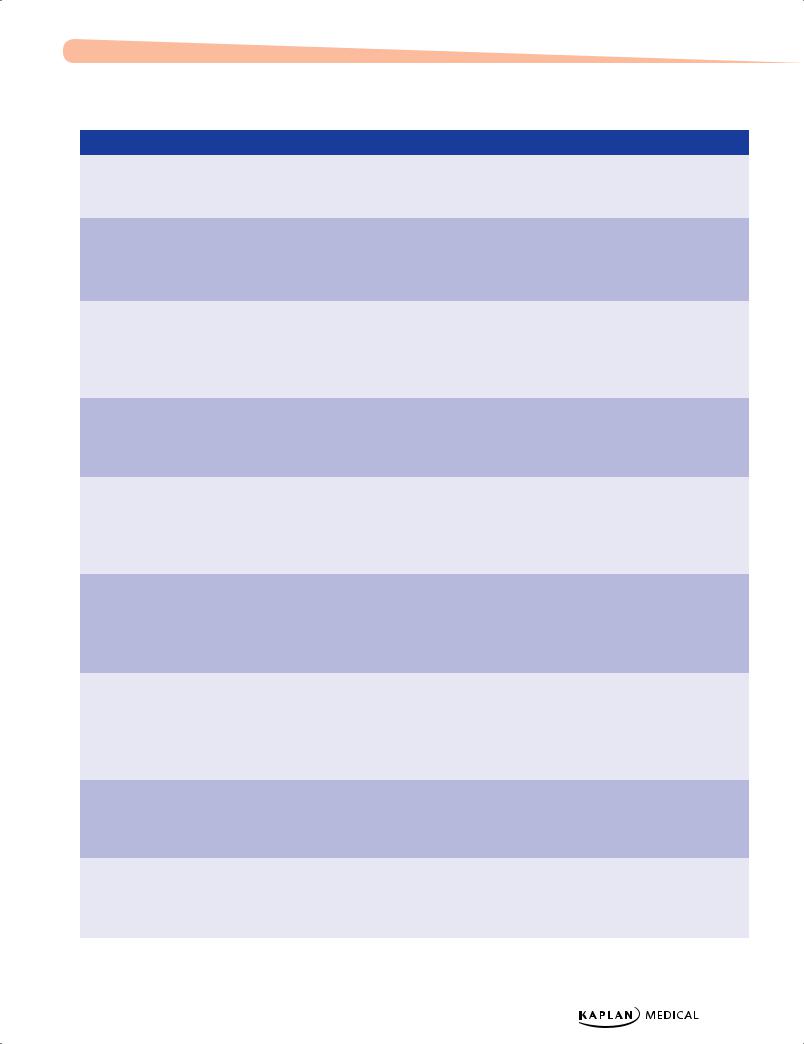
Table 4-1. Newborn Reflexes
|
Reflex |
|
|
Description |
|
|
Appears |
|
|
Disappears |
|
|
CNS Origin |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Moro |
Extend head → extension, |
Birth |
4–6 mo |
Brain stem |
|||||||||
|
|
|
flexion of arms, legs |
|
|
|
|
|
|
vestibular nuclei |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Grasp |
Finger in palm → hand, |
Birth |
4–6 mo |
Brain stem |
||||||||||
|
|
|
elbow, shoulder flexion |
|
|
|
|
|
|
vestibular nuclei |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Rooting |
Cheek stimulus → turns |
Birth |
4–6 mo |
Brain stem |
||||||||||
|
|
|
mouth to that side |
|
|
|
|
|
|
trigeminal system |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Trunk incurvation |
Withdrawal from stroking |
Birth |
6–9 mo |
Spinal cord |
||||||||||
|
|
|
along ventral surface |
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Placing |
Steps up when dorsum of |
Birth |
4–6 mo |
Cerebral cortex |
||||||||||
|
|
|
foot stimulated |
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Asymmetric |
Fencing posture when |
Birth to 1 |
4–6 mo |
Brain stem |
||||||||||
tonic neck (ATNR) |
supine |
month |
|
|
|
vestibular nuclei |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Parachute |
Simulate fall → extends |
6–8 mo |
Never |
Brain stem |
||||||||||
|
|
|
arms |
|
|
|
|
|
|
vestibular |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
44
Chapter 4 λ Development
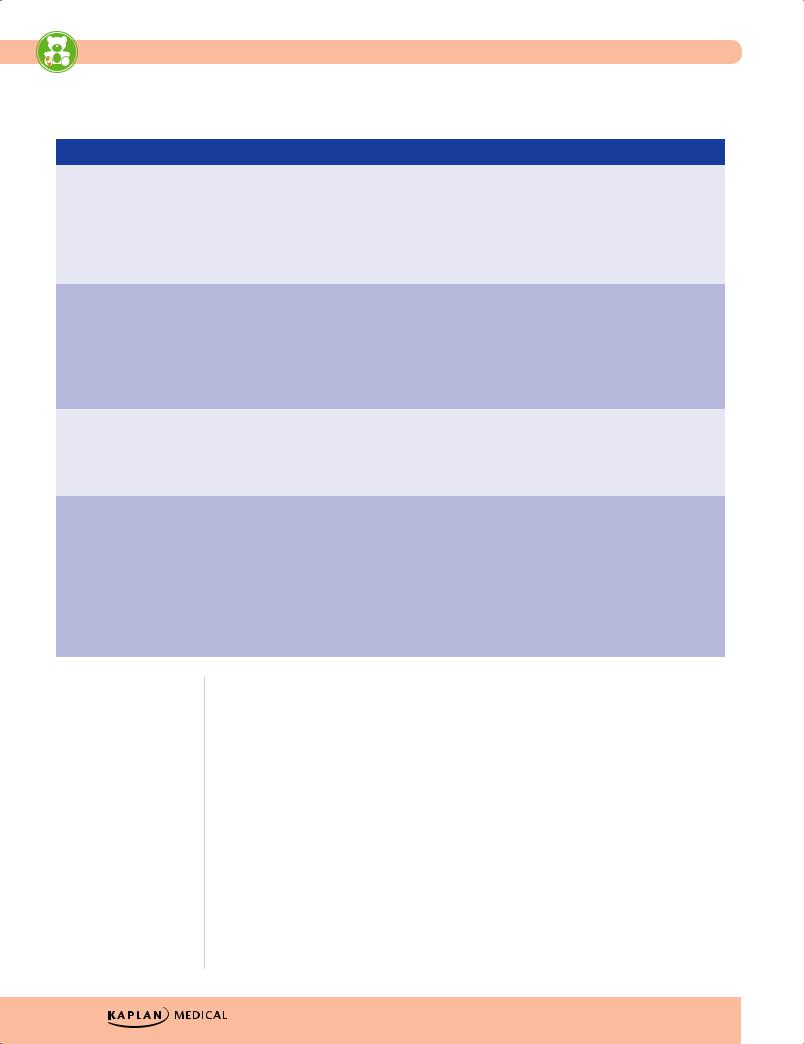
Table 4-2. Developmental Milestones
|
|
Gross Motor |
|
|
Visual Motor |
|
|
Language |
|
|
Social Adaptive |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Birth |
|
• Symmetric |
|
• Visually fixes on an |
|
• Alerts to sound |
|
• Regards face |
||||
|
|
movements in supine |
|
object |
|
|
|
|
|
|
||
|
|
• Head flat in prone |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2 months |
|
• Head in midline while |
|
• Follows past midline |
|
• Smiles in response to |
|
• Recognizes parent |
||||
|
|
held sitting |
|
|
|
|
touch and voice |
|
|
|
||
|
|
• Raises head in prone |
|
|
|
|
|
|
|
|
|
|
|
|
• Begins to lift chest |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4 months |
|
• Holds head steadily |
|
• Reaches with both |
|
• Laughs |
|
• Likes to look around |
||||
|
|
• Supports on forearms |
|
arms together |
|
• Orients to voice |
|
|
|
|||
|
|
|
|
|
|
|
|
|
||||
|
|
in prone |
|
• Hands to midline |
|
• Coos |
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
||
|
|
• Rolls from prone to |
|
|
|
|
|
|
|
|
|
|
|
|
supine |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
6 months |
|
• Sits with support |
|
• Unilateral reach |
|
• Babbles |
|
• Recognizes that |
||||
|
|
(tripod) |
|
• Raking grasp |
|
|
|
|
someone is a |
|||
|
|
|
|
|
|
|
|
|
stranger |
|||
|
|
• Feet in mouth in |
|
• Transfers object |
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
||||
|
|
supine |
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
7 months |
|
• Rolls from supine to |
|
|
|
|
|
|
|
|
|
|
|
|
prone |
|
|
|
|
|
|
|
|
|
|
|
|
• May crawl |
|
|
|
|
|
|
|
|
|
|
|
|
• Starts to sit without |
|
|
|
|
|
|
|
|
|
|
|
|
support |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
9 months |
|
• Crawls well |
|
• Immature pincer |
|
• “Mama,” “dada,” |
|
• Plays gesture games |
||||
|
|
• Pulls to stand |
|
grasp |
|
indiscriminately |
|
• Explores environment |
||||
|
|
|
|
|
|
|
|
|
||||
|
|
• Starting to cruise |
|
• Holds bottle |
|
• Understands “no” |
|
(crawling and |
||||
|
|
|
|
|
|
|
|
|
cruising) |
|||
|
|
|
|
|
• Throws object (not |
|
• Understands gestures |
|
||||
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
overhand) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
12 months |
|
• May walk alone (must |
|
• Mature pincer grasp |
|
• 1-2 words other than |
|
• Imitates actions |
||||
|
|
by 18 months) |
|
• Crayon marks |
|
“mama” and “dada” |
|
• Comes when called |
||||
|
|
|
|
|
|
(used appropriately) |
|
|||||
|
|
|
|
|
• Object permanence |
|
|
• Cooperates with |
||||
|
|
|
|
|
|
• Follows 1-step |
|
|||||
|
|
|
|
|
(from 10 months) |
|
|
dressing |
||||
|
|
|
|
|
|
command with |
|
|||||
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
gesture |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
15 months |
|
• Creeps up stairs |
|
• Scribbles and builds |
|
• 4-6 words |
|
• Uses cup and spoon |
||||
|
|
• Walks backward |
|
towers of 2 blocks in |
|
• Follows 1-step |
|
(variable until 18 |
||||
|
|
|
imitation |
|
|
months) |
||||||
|
|
|
|
|
|
command without |
|
|||||
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
gesture |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
18 months |
|
• Runs |
|
• Scribbles |
|
• 15-25 words |
|
• Imitates parents in |
||||
|
|
• Throws objects |
|
spontaneously |
|
• Knows 5 body parts |
|
tasks |
||||
|
|
|
|
|
|
|
|
|
||||
|
|
overhand while |
|
• Builds tower of 3 |
|
|
|
|
• Plays in company of |
|||
|
|
standing |
|
blocks |
|
|
|
|
other children |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(Continued) |
|
Published by dr-notes.com |
45 |
|
|
|
|
USMLE Step 2 CK λ Pediatrics
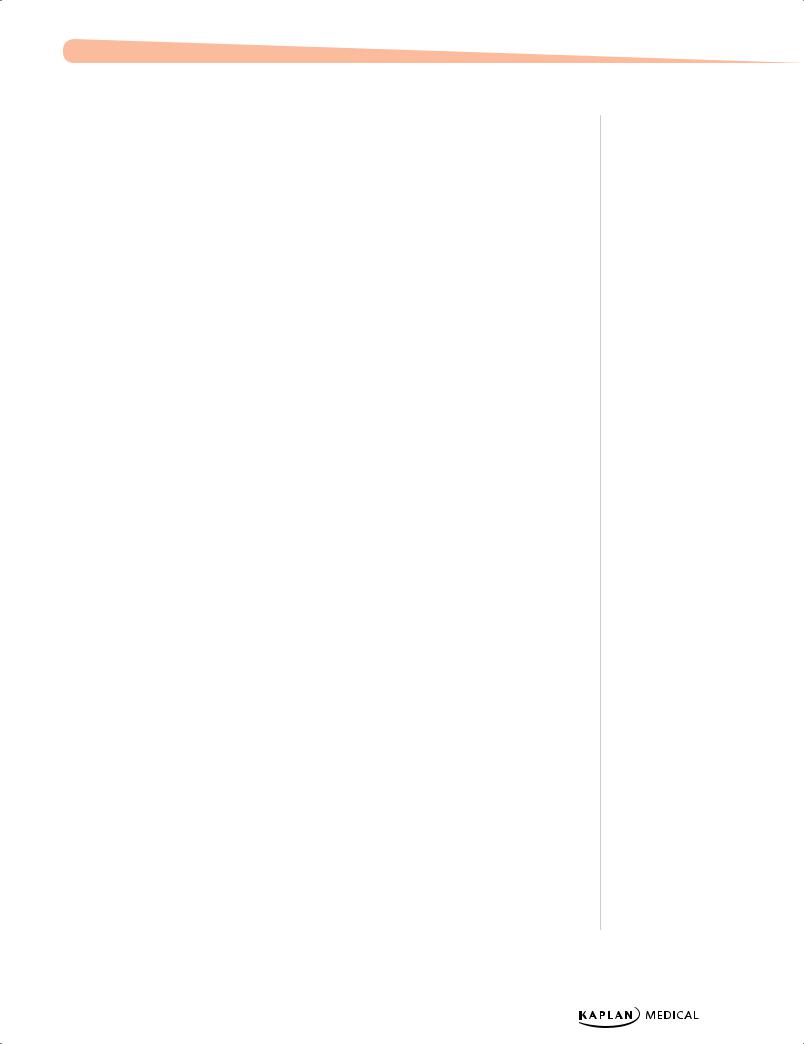
Table 4-2. Developmental Milestones (Cont’d)
|
|
Gross Motor |
|
|
Visual Motor |
|
|
Language |
|
|
Social Adaptive |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
24 months |
|
• Walks up and down |
|
• Imitates stroke (up or |
|
• 50 words |
|
• Parallel play |
||||
|
|
stairs one foot at a |
|
down) with pencil |
|
• 2-word sentences |
|
|
|
|||
|
|
time |
|
|
|
|
|
|
|
|||
|
|
|
• Builds tower of |
|
• Follows 2-step |
|
|
|
||||
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
7 blocks |
|
|
|
|
|||
|
|
|
|
|
|
commands |
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
• Removes clothing |
|
• Uses pronouns |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
inappropriately |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3 years |
|
• Alternates feet going |
|
• Copies a circle |
|
• ≥250 words |
|
• Group play |
||||
|
|
up the stairs |
|
• Undresses |
|
• 3-word sentences |
|
• Shares |
||||
|
|
|
|
|
|
|
||||||
|
|
• Pedals tricycle |
|
completely |
|
• Plurals |
|
• Takes turns |
||||
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
• Dresses partially |
|
• All pronouns |
|
• Knows full name, age |
|||
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
• Unbuttons |
|
|
|
|
and gender |
||
|
|
|
|
|
• Dries hands |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4 years |
|
• Alternates feet going |
|
• Copies a square |
|
• Knows colors |
|
• Plays cooperatively |
||||
|
|
downstairs |
|
• Buttons clothing |
|
• Recites songs from |
|
• Tells “tall tales” |
||||
|
|
|
|
|
|
|
||||||
|
|
• Hops and skips |
|
• Dresses completely |
|
memory |
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
• Catches ball |
|
• Asks questions |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
5 years |
|
• Skips alternating feet |
|
• Copies triangle |
|
• Prints first name |
|
• Plays cooperative |
||||
|
|
• Jumps over lower |
|
• Ties shoes |
|
• Asks what a word |
|
games |
||||
|
|
|
|
|
|
|
||||||
|
|
obstacles |
|
• Spreads with knife |
|
means |
|
• Abides by rules |
||||
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
• Answers all “wh-” |
|
• Likes to help in |
||
|
|
|
|
|
|
|
|
questions |
|
household tasks |
||
|
|
|
|
|
|
|
|
• Tells a story |
|
|
|
|
|
|
|
|
|
|
|
|
• Plays pretend |
|
|
|
|
|
|
|
|
|
|
|
|
• Knows alphabet |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Clinical Recall
A young boy is able to walk and build a tower with 7 blocks. He plays well alongside other children and can say “my toy” or “my turn,” with an inventory of about 50 words. What is the most likely age of the child?
A.12 months
B.15 months
C.18 months
D.24 months
E.36 months
Answer: D
46
Chapter 4 λ Development
Possible Abnormalities
You must take into account the number of weeks of prematurity to assess development appropriately, i.e., per the preterm age, NOT chronological. For instance, a 6-month-old baby born at 32 weeks (i.e., 2 months preterm) must be assessed at 6 – 2 = 4 months CORRECTED AGE. Do this until chronological age 2 years, then consider delays to be true.
•If there appears to be a language delay, first consider conductive hearing loss. While all babies receive hearing testing within the first month of life, that is for congenital sensorineural hearing loss. Over the first year of life, conductive hearing loss may occur from repeated ear infections.
•If there is a lack of development or regression of language skills with impaired social interaction, restricted activities and interests and stereotypic behaviors, consider autistic spectrum disorder. Onset of abnormal findings must occur age <3 years.
–After a complete H and P with neurologic exam and development testing, the first step is to perform an autism screening questionnaire. If you feel the diagnosis is likely, the next step is to refer to a specialist in this area.
•Delay is defined as ≥1 skills significantly below average, i.e., developmental quotient
(developmental age/chronological age x 100) is <75. When you find this, you must first look for a possible reason, and the child will need developmental therapy in ≥1 areas.
Published by dr-notes.com |
47 |
|
|
|
|

Behavioral/Psychological Disorders |
5 |
Chapter Title |
Learning Objective
Solve problems concerning eating disorders, elimination disorders, and sleep disorders
EATING DISORDERS
Pica
•Repeated or chronic ingestion of non-nutritive substances, e.g., paint, dirt
•After year 2, needs investigation
•Predisposing factors
–Intellectual disability and lack of parental nurturing
–Also with family disorganization, poor supervision, and psychologic neglect
•More common with autism, brain-behavior disorders, and low socioeconomic status
•Increased risk for lead poisoning, iron deficiency, and parasitic infections
ELIMINATION DISORDERS
Enuresis
A 7-year-old boy has problems with bedwetting. The mother says that during the day he has no problems but is usually wet 6 of 7 mornings. He does not report dysuria or frequency, and has not had increased thirst. The mother also says that he is a deep sleeper.
•Voluntary or involuntary repeated discharge of urine after a developmental age when bladder control should be present (most by age of 5 years); there are 2 types
•Primary:
–No significant dry period; most common and usually nocturnal (nocturnal enuresis)
–Hyposecretion of ADH and/or receptor dysfunction
Published by dr-notes.com |
49 |
|
|
|
|

USMLE Step 2 CK λ Pediatrics
–Relationship of sleep architecture, diminished arousability during sleep, and abnormal bladder function; anatomic malformations
–Management—thorough history and physical, (should begin with behavioral treatment; not definitive, varying success rates):
°Enlist cooperation of child—chart dryness, reward system
°Child should void before going to sleep
°Alarm to wake once 2−3 hours after falling asleep; may use alarm that goes off when child wets a special sheet (bell and pad alarm)
°No punishment or humiliation
°Psychotherapy for traumatized children or when behavioral therapy has failed
°Pharmacotherapy for failed behavioral therapy in nocturnal enuresis— oral desmopressin (DDAVP)
•Secondary:
− After a period of dryness ≥6 months
− Causes—psychological, urinary tract infection, constipation, diabetes − More common in girls
− Evaluation—urinalysis
− Management—treat underlying disorder
•Children with both diurnal and nocturnal enuresis:
− Especially with voiding difficulties, more likely to have abnormalities of the urinary tract
− Ultrasonography or flow studies are indicated in these cases.
Encopresis
•Passage of feces into inappropriate places after a chronologic age of 4 years, or equivalent developmental level
•May be primary or secondary
•Causes—psychological (toilet phobia), early toilet training, aggressive management of constipation, painful defecation, fissures
•Types
−Retentive encopresis most common:
°2/3 of cases
°Hard stool on rectal examination is sufficient to document, but a negative exam requires a plain abdominal x-ray
°Presence of fecal retention is evidence of chronic constipation, and thus treatment will require active constipation management
°May have abnormal anal sphincter function
•Associations
−Primary encopresis—especially in boys, associated with global developmental delays and enuresis
−Secondary encopresis—high levels of psychosocial stressors and conduct disorder
50
Chapter 5 λ Behavioral/Psychological Disorders
•Management
−Clear impacted fecal material (with mineral oil or laxative) but avoid long-term laxative use
−Concomitant behavioral management
−Regular postprandial toilet-sitting
−High-fiber diet
−Familial support for behavior modification
−Group or individual psychotherapy
Clinical Recall
A concerned mother brings her 4-year-old son to the physician for evaluation of nocturnal enuresis. The boy has never had a significant dry period. He has regular bowel movements without constipation or encopresis. What is the most appropriate next step?
A.Encourage the mother to use a bell and pad alarm system
B.Order a urinalysis to assess for infection
C.Punish the child whenever he wets the bed
D.Refer the mother and child to psychotherapy
E.Reassure the mother that this is normal for the boy’s age
Answer: E
SLEEP DISORDERS
Parasomnias
Parasomnias are episodic nocturnal behaviors that often involve cognitive disorientation and autonomic and skeletal muscle disturbance
•Associated with relative CNS immaturity
•More common in children than adults; abate with age
Published by dr-notes.com |
51 |
|
|
|
|
USMLE Step 2 CK λ Pediatrics
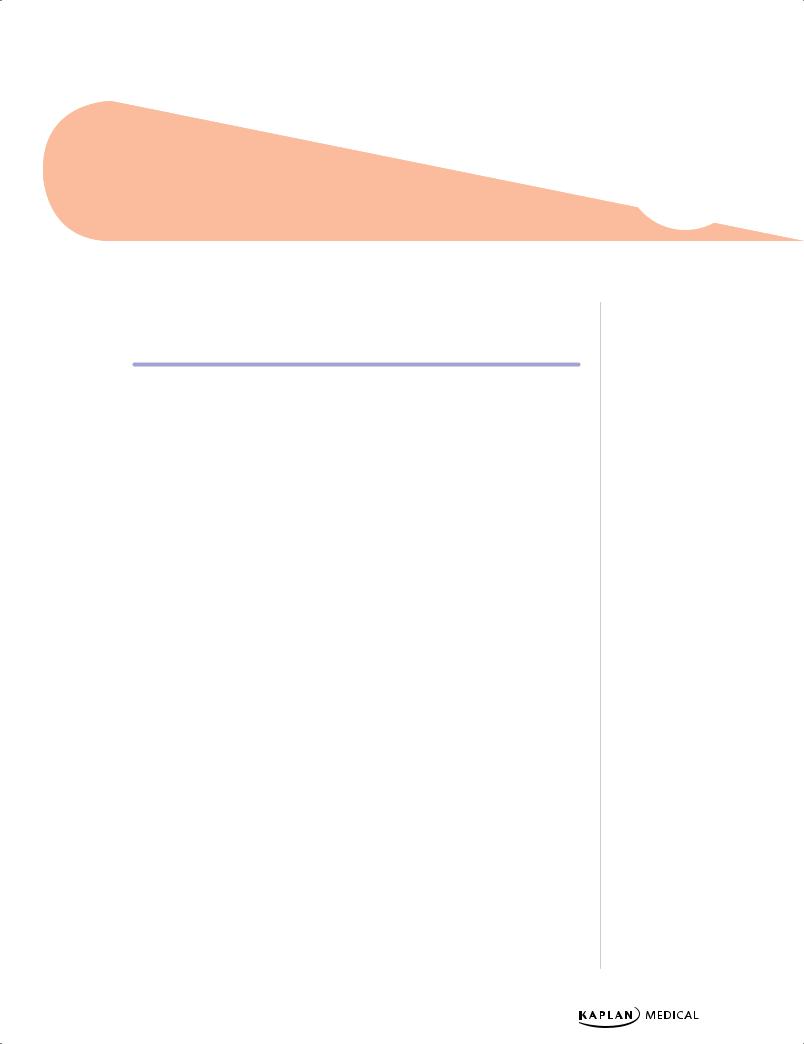
Table 5-1. Parasomnias
|
Sleepwalking and Sleep Terrors |
|
|
Nightmares |
|
|
(Partial Arousal) |
|
|
|
|
|
|
|
|
|
|
|
• First third of night |
|
• Last third of night |
||
|
|
|
|
|
|
|
• During slow-wave sleep |
|
• REM sleep |
||
|
|
|
|
|
|
|
• No daytime sleepiness or recall |
|
• Daytime sleepiness (if prolonged waking) |
||
|
|
|
|
and vivid recall |
|
|
|
|
|
|
|
|
• High arousal threshold (agitated if |
|
• Low arousal threshold (easily awakened) |
||
|
• awakened) |
|
|
|
|
|
|
|
|
|
|
|
• Common family history |
|
• No family history |
||
|
|
|
|
|
|
|
• Displaced from bed |
|
• May be displaced from bed |
||
|
|
|
|
|
|
|
• Sleepwalking relatively common; |
|
• Very common |
||
|
night terrors rare |
|
|
|
|
|
|
|
|
|
|
|
• Treatment: parental education, |
|
• No required treatment unless persistent/ |
||
|
reassurance, avoid exacerbating |
|
frequent, in which case possible abuse or |
||
|
factors, i.e., sleep deprivation, safety |
|
anxiety disorder should be investigated. |
||
|
precautions |
|
|
|
|
|
|
|
|
|
|
52
Immunizations 6
Chapter Title
Learning Objectives
Define active immunization
Describe different routes of immunization for specific routine vaccines
A 6-month-old patient is being seen for routine care. The baby is doing well, and physical examination, growth, and development are normal. The mother states that after the last set of immunizations the baby had a temperature of 39.4 C (103 F) and cried for 2 hours but was consolable. What is your advice to this mother before administering the next set of immunizations?
ACTIVE IMMUNIZATIONS
Table 6-1. Classification of Vaccines
|
|
|
Live Attenuated |
|
|
|
|
|
|
|
|
|
|
• Viral |
|
MMR, varicella, yellow fever, nasal influenza, |
|
|
|
|
|
smallpox, oral rotavirus |
|
|
|
• Bacterial |
|
BCG, oral typhoid |
|
|
|
|
|
|
|
|
|
|
|
Inactivated |
|
|
|
|
|
|
|
Whole |
• Virus |
Fractional |
• Protein-based |
|
• Polysaccharide |
|
based |
|
|
Polio, rabies, hepatitis A
Subunit: hepatitis B, parenteral influenza, acellular pertussis
Toxoid: diphtheria, tetanus
Pure: pneumococcal, Hib, meningococcal Conjugate: Hib, pneumococcal, meningococcal
Vaccine Rules
For stimulation of an adequate and persisting antibody response, 2 or more doses are usually required. In general, vaccines from different manufacturers are interchangeable.
Published by dr-notes.com |
53 |
|
|
|
|