

Chapter 12
Other Indications for Biopsy of Kidneys
Introduction
Renal biopsy is hardly ever done other than to investigate the nephrotic syndrome, acute renal failure, chronic renal failure, hematuria, and proteinuria, and in various circumstances related to grafts.
Investigation of the Kidney in Systemic Disease
Rarely, a renal biopsy is taken in vasculitis or in systemic lupus erythematosus, even though there are no clinical or chemical indications of renal abnormalities to see whether the disease has affected the kidney. Even a minor abnormality, such as microscopic hematuria, increases the chance that significant disease will be found in the kidney. In vasculitis, only one glomerulus with a vasculitic lesion has to be seen to give the diagnosis (Fig. 7.12).
Investigation of Metabolic or Other Familial Disorders, and Disorders of Tubular Function
Especially in children, renal biopsy may be done to investigate suspected or known metabolic disorders or other familial disorders. Such disorders include cystic diseases, nail patella syndrome, hypokalemic conditions, and abnormalities of calcium or magnesium, or other minerals. Disorders of tubular function may be investigated by renal biopsy, such as those associated with tubular proteinuria and other features of Fanconi syndrome (Fig. 8.21) or renal tubular acidosis (Figs 7.39 and 8.19).
Biopsy specimens in most of these conditions show structural abnormalities to different extents, but generally they require investigation in specialised centres.
A. J. Howie, Handbook of Renal Biopsy Pathology. |
305 |
C Springer 2008 |
|
306 |
12 Other Indications for Biopsy of Kidneys |
Assessment of Effects of Treatment on the Kidney
Renal biopsy may be done to determine whether a treatment has damaged the kidney, although its effects may not yet be apparent clinically. The most common example of this is in the nephrotic syndrome treated with calcineurin inhibitors, such as cyclosporine. A sign of the chronic ischemic effect of this drug on the kidney is the presence of atrophic areas, and there may be other features (Figs 2.1, 7.4, 7.9, and 11.30–11.32). If there has been a previous biopsy specimen, the pathologist can judge whether cyclosporine appears to have had a significant effect, especially in minimal change nephropathy, in which only age-related chronic damage would otherwise be expected. The pathologist may see a significant amount of chronic damage before clinical tests of excretory renal function detect renal impairment.
Cyclosporine may be the explanation of development of segmental sclerosing glomerular lesions in a person shown to have minimal change nephropathy in an earlier renal biopsy specimen.
Investigation of a Renal Mass
Biopsy may be used in investigation of a renal mass. This is not done by nephrologists, and rarely done by urologists, whose opinion is usually requested. After appropriate imaging, partial or total nephrectomy is often performed on the assumption that the mass is a primary neoplasm of the kidney. Biopsy is usually avoided, because the findings are unlikely to change management, and there is a risk of dissemination of cancer along the biopsy track.
Biopsy may be considered if there is disseminated neoplasia to see whether there is a primary malignant neoplasm in the kidney, or whether the renal mass is a metastasis. Occasionally, there may be biopsy of a solitary renal mass to help to decide on the type of operation to be done. For instance, if a transitional cell carcinoma is suspected and then confirmed by biopsy, the surgeon may remove all the ureter as well as the kidney, rather than just the kidney.
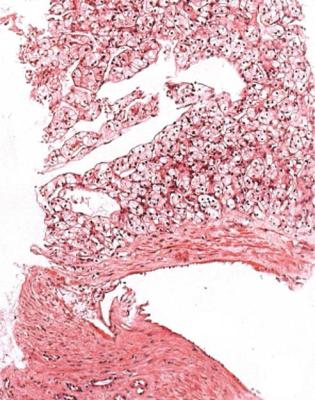
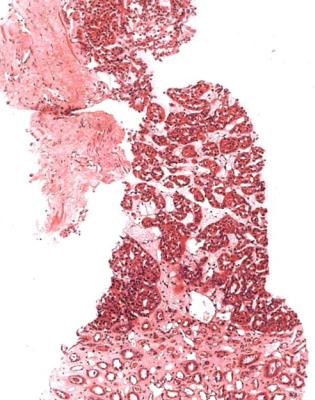
The commonest finding in biopsy specimens of renal masses is renal cell carcinoma. Usually this appears a clear cell neoplasm, although sometimes the cells may be eosinophilic, or spindle shaped, or chromophobe, or there may be a mixture of appearances (Figs 12.1 and 12.2). Usually on immunohistologic study, a chromophobe carcinoma expresses E cadherin but not vimentin, while the opposite is found in a clear cell carcinoma.
The main differential diagnoses of a clear cell carcinoma of the kidney are normal adrenal cortical tissue and an adrenocortical neoplasm (Fig. 12.3). Adrenal gland is recognised by the presence of medulla and fine vacuolation in the cytoplasm of cortical cells. Adrenal gland and adrenocortical neoplasms do not express broad spectrum cytokeratins, epithelial membrane antigen, or CD10, but a renal cell carcinoma expresses these markers.
Investigation of a Renal Mass |
307 |
Fig. 12.1 Needle biopsy specimen of a mass found incidentally in the kidney of a man of 70, during follow up after treatment of a hepatocellular carcinoma. There is a clear cell carcinoma, typical of renal cell carcinoma, with no resemblance to the hepatic neoplasm
Other renal neoplasms that may be seen include transitional cell carcinoma (Fig. 12.4), basophilic tubular neoplasms that are usually difficult to interpret in biopsy specimens (Fig. 12.5), or appearances suggestive of an oncocytoma (Fig. 12.6). An oncocytoma does not express CD10 or vimentin. An oncocytoma and some basophilic neoplasms are benign, but a sensible course for a pathologist is to remember that the biopsy specimen may not be representative of the whole mass, and that the sample may be from a renal cell carcinoma.
Biopsy may show other neoplasms, such as a lymphoma (Figs 4.2, 7.11, 11.35, and 11.36), or metastatic carcinoma (Fig. 12.7), although the kidney is an unusual site for metastasis from any malignant neoplasm. In someone with a known cancer, there may be evidence of a spread to the kidney in a renal biopsy specimen taken to investigate any of the usual indications for biopsy.

308 |
12 Other Indications for Biopsy of Kidneys |
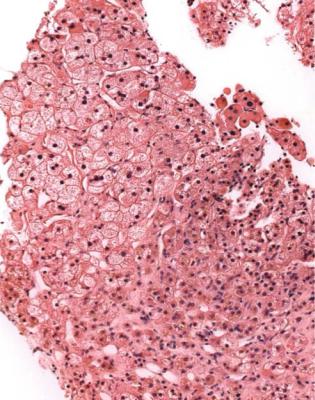
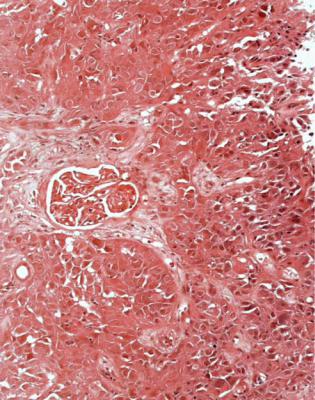
Fig. 12.2 Needle biopsy specimen of a lesion in the kidney of a man of 67 found to have a complex cyst on radiographic investigation. There is a papillary eosinophilic neoplasm consistent with a renal cell carcinoma
Chance Finding of a Neoplasm in a Renal Biopsy Specimen
Rarely a renal biopsy specimen taken for any reason may by chance contain a neoplasm, in a person not known to have cancer (Figs 4.9 and 12.8). About one specimen in 500 may show this. The lesion is likely to be no more than a few millimetres in diameter, because larger ones should be detected by investigations before the biopsy, such as intravenous urography or ultrasonography. If not metastatic (Fig. 4.9), the neoplasm may be papillary, cystic, or solid, and may have cells that are clear, eosinophilic, or basophilic. Although clear cells are a sign of a definite renal cell carcinoma (Fig. 12.1), most lesions found by chance do not consist of clear cells. Usually these are papillary adenomas, which occur with increasing frequency with age, and may be multiple and bilateral (Fig. 12.8).
After chance finding of a primary neoplasm, one course of action is for nephrologists or urologists to arrange detailed imaging of the kidney, and consider partial nephrectomy, if appropriate, if a lesion is seen. A mass under 5 mm diameter is
Summary: Other Indications for Biopsy of Kidneys |
309 |
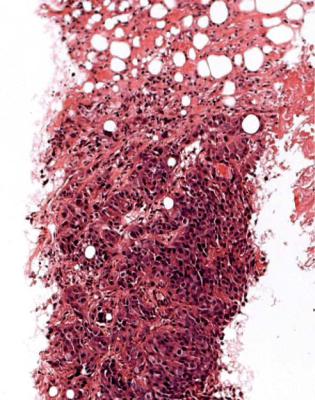
Fig. 12.3 Adrenal cortex in a specimen from an attempted needle biopsy of kidney in a man of 49
unlikely to be detectable, and in this case, a surgeon would not know which part of the kidney to resect. Surveillance by imaging at intervals may be considered, but whether this is necessary is unknown. The pathologist should be included in discussions about management, the aim of which is to avoid unnecessary surgery for a trivial lesion and to ensure that a potentially lethal neoplasm is adequately treated.
Summary: Other Indications for Biopsy of Kidneys
Renal biopsy is hardly ever done other than for the nephrotic syndrome, acute renal failure, chronic renal failure, hematuria, and proteinuria, and in renal allografts.
Renal biopsy may be used in investigation of the clinically normal kidney in systemic disease, such as vasculitis.
Some unusual metabolic or other familial or tubular disorders may be investigated by renal biopsy.
Renal biopsy may be used to investigate a renal mass. The commonest finding is renal cell carcinoma. A neoplasm may be found by chance in any biopsy specimen.
310 |
12 Other Indications for Biopsy of Kidneys |
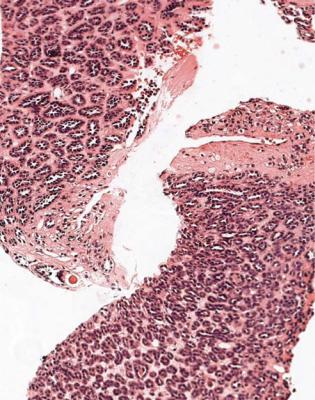
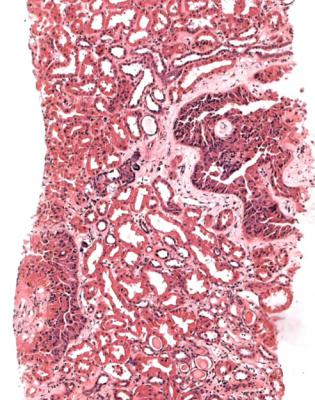
Fig. 12.4 Needle biopsy specimen of a mass found in the kidney of a man of 68, during follow up of transitional cell carcinoma of the bladder. There is a transitional cell carcinoma
Summary: Other Indications for Biopsy of Kidneys |
311 |
Fig. 12.5 Needle biopsy specimen of a mass found incidentally by computed tomography in the kidney of a woman of 69. There is a basophilic tubular neoplasm of metanephric type. Distinction between basophilic renal cell carcinoma, metanephric neoplasms, and nephroblastoma may be difficult in a needle biopsy specimen
312 |
12 Other Indications for Biopsy of Kidneys |
Fig. 12.6 Needle biopsy specimen of a mass found incidentally in the kidney of a woman of 60, during follow up after treatment of fibromatosis. There is a neoplasm consisting of small groups of uniform eosinophilic cells consistent with an oncocytoma
Summary: Other Indications for Biopsy of Kidneys |
313 |
Fig. 12.7 Needle biopsy specimen of a mass found in the kidney of a man of 51 during investigation of a lung mass. There is a squamous carcinoma, partly necrotic, consistent with a metastasis from carcinoma of the bronchus
314 |
12 Other Indications for Biopsy of Kidneys |
Fig. 12.8 Needle biopsy specimen of kidney from a man of 83 with chronic renal failure, hematuria, proteinuria, and normal kidneys on ultrasonography. As a chance finding, there are a couple of areas of neoplastic tissue, probably part of one lesion, consistent with an eosinophilic renal cell neoplasm. No mass was detected on detailed imaging, and no action was taken to treat the renal cell neoplasm. The man died 3 years after the biopsy with no evidence of carcinoma of the kidney
Further Reading: Other Indications for Biopsy of Kidneys |
315 |
Further Reading: Other Indications for Biopsy of Kidneys
Jennette JC, Olson JL, Schwartz MM, Silva FG. Heptinstall’s Pathology of the Kidney. Sixth ed. Philadelphia: Lippincott Williams and Wilkins, 2007. Chapter 29.
Murphy WM, Grignon DJ, Perlman EJ. Tumors of the kidney, bladder, and related urinary structures. AFIP Atlas of Tumor Pathology, Fourth Series, Fascicle 1. Washington, DC: Armed Forces Institute of Pathology, 2004.
Pankhurst T, Howie AJ, Adu D, Wallace DMA, Lipkin GW. Incidental neoplasms in renal biopsies.
Nephrology Dialysis Transplantation 2006; 21: 64–69.