

Gale Encyclopedia of Genetic Disorder / Gale Encyclopedia of Genetic Disorders, Two Volume Set - Volume 2 - M-Z - I
.pdfTrisomy 18
however, as men and women age. For anyone who has a fetus or child diagnosed with trisomy 18, the risk for a chromosomal disorder of any type in subsequent offspring is about 1%, the exception being women over age 35, who face their age-related risk.
Mosaic trisomy 18
If the body contains a mixture of cells, some with trisomy 18 and some with a normal chromosome count, the condition is called mosaic trisomy 18. A small percentage of Edwards syndrome cases are due to mosaic trisomy 18.
Mosaic trisomy 18 occurs in one of two ways. The first involves mitotic (rather than meiotic) nondisjunction of chromosomes 18, in which a cell undergoing mitosis in a chromosomally normal embryo produces one cell with trisomy 18 and another with monosomy 18. The cell with monosomy 18 cannot survive, but if the trisomic cell survives, all cells in the body derived from it will have trisomy 18. These trisomic cells, combined with the normal cells that continue to develop, result in mosaic trisomy 18. The other cause of mosaicism involves an embryo with full trisomy 18. In this case, however, one cell loses its extra chromosome during mitosis. The result is a euploid cell, which in turn produces a euploid cell line in addition to the original trisomic cell line. Since mitotic nondisjunction appears to be the cause in most cases, and is due purely to chance, the recurrence risk for subsequent offspring after the diagnosis of mosaic trisomy 18 is less than 1%.
Because they have some normal cells, individuals with mosaic trisomy 18 tend to be less severely affected than those with full trisomy 18, but not always. Much of the prognosis depends on the total percentage of trisomic cells in the body and/or the proportion of trisomic cells in specific tissues and organs. There is no way to determine exact percentages of cells, and therefore no way to provide an accurate prognosis.
Partial trisomy 18
A third cause of Edwards syndrome is a rearrangement, or translocation, of genetic material between chromosome 18 and another chromosome. An unbalanced chromosome translocation (extra and/or missing genetic material) may result in an embryo that has an extra piece of chromosome 18, known as partial trisomy 18. If cells are trisomic for a portion of chromosome 18, the result could be a form of Edwards syndrome. However, translocations between chromosomes can be complicated, and some cases of partial trisomy 18 may result in a pattern of anomalies that does not resemble Edwards syndrome.
Unbalanced translocations can occur in an embryo for the first time (de novo), or they can be inherited from a healthy parent who is a carrier of the translocation in a balanced state (no missing or extra genetic material). Normal blood chromosome tests on both parents implies the translocation was de novo, which means no increased risk for subsequent offspring. Detection of a balanced translocation in one parent, however, presents an increased risk for unbalanced translocations in subsequent offspring, as well as an increased risk for pregnancy loss. In cases of partial trisomy 18, genetic counseling is critical to help determine risks and available options. Chromosome translocations resulting in partial trisomy 18 make up a small percentage of Edwards syndrome cases.
Demographics
The incidence of Edwards syndrome is about one in 5,000 births. Two-thirds of all newborns with the condition are female, probably because males with trisomy 18 are more likely to be miscarried. The condition is not known to occur more frequently in any ethnic group or in any part of the world. Increased parental age is the only factor known to result in a greater risk for trisomy 18. In the United States, parents of babies with trisomy 18 average about 32 years of age, while 26 is the average age for parents of children without a chromosomal disorder. The risk increases with age in both sexes, but begins earlier and is more pronounced in women.
Increasing maternal age elevates the risk for chromosomal disorders due to nondisjunction in general, not just trisomy 18. For instance, a 20-year-old woman has about a 1 in 10,000 chance of having a child with trisomy 18, while the risk of having a child with any chromosomal disorder at that age is 1 in 800. By age 35, those same risks have risen to 1 in 2,000 and 1 in 200 respectively, and increase to 1 in 600 and 1 in 65 at age 40. Other common chromosomal disorders caused by nondisjunction that result in live birth include trisomy 21 (Down syndrome), trisomy 13 (Patau syndrome), and several conditions caused by aneuploidy of the sex chromosomes.
Signs and symptoms
Many physical anomalies and medical complications are associated with Edwards syndrome. In fact, well over 100 different anomalies have been reported in the medical literature. The more common findings are categorized and described below.
Prenatal anomalies
The majority of pregnancies in which the embryo/fetus has trisomy 18 will result in miscarriage or
1146 |
G A L E E N C Y C L O P E D I A O F G E N E T I C D I S O R D E R S |
stillbirth. Some physical anomalies of the heart, skeleton, brain, kidneys, and body walls have the best chance of being detected by prenatal ultrasound. Other, pregnancyrelated findings include intrauterine growth restriction (IUGR) of the fetus, a single umbilical artery (also called two vessel cord), and too much (polyhydramnios) or too little (oligohydramnios) amniotic fluid. While detection of fetal anomalies by ultrasound may lead to suspicion of Edwards syndrome, the diagnosis can only be confirmed by chromosome testing. Women carrying a fetus with Edwards syndrome sometimes report they feel little movement. Cesarean sections are more common due to abnormal fetal position or fetal distress near term.
General anomalies
Of those babies with Edwards syndrome that are live-born, two-thirds are delivered several weeks earlier or later than their expected due date. Low birth weight is common, as are low Apgar scores (measurements of a newborn’s activity just after birth). Newborns are frail, and tend to have a weak cry and difficulty feeding. Muscles may be poorly developed, and often become tight and contracted (hypertonic). Extra hair (hirsutism) on the forehead and back is sometimes seen, as is loose, redundant skin.
Abnormalities of the lungs, kidneys, pancreas, spleen, and gastrointestinal system are associated with Edwards syndrome. The thyroid, thymus, and adrenal glands may be affected. Anomalies of the breastbone, radius (bone in the forearm), ribs, pelvis, and the spine (scoliosis) are the more frequent skeletal findings. An abdominal wall defect (omphalocele) or hernia in the abdominal region may be present. Genital (sex organ) anomalies in both males and females have been described.
Heart anomalies
Ninety percent of babies with Edwards syndrome have one or more heart defects. Ventricular septal defects (VSD) and atrial septal defects (ASD), holes between the lower and upper chambers of the heart respectively, are the most common cardiac problems. Patent ductus arteriosis (open connection between the pulmonary artery and aorta) and abnormal heart valves are also typical.
Craniofacial anomalies
Small head size (microcephaly) and a prominent occiput (back of the skull) are variations in skull shape typical of Edwards syndrome. Common facial features include widely spaced and/or slanted eyes, skin folds at the inner eyelid (epicanthal folds), ptosis (drooping) of the eyelids, low-set malformed ears, a small oral opening,
narrow palate or cleft lip/palate, and a small jaw (micrognathia).
Hand and foot anomalies
A specific pattern of hand and foot anomalies is seen in most infants with Edwards syndrome. Clenched hands, with the index finger overlapping the third and the fifth finger overlapping the fourth, are a classic sign. Abnormal dermatoglyphics (finger print pattern), underdeveloped nails, outward or inward deviation of the hand, underdeveloped or absent thumbs, and a single crease across the palm are other frequent anomalies of the hands. Abnormalities affecting the feet include so-called “rocker-bottom feet” and clubfoot.
Central nervous system anomalies
Probably the most medically significant abnormal development that occurs in Edwards syndrome involves the brain. Some anomalies, such as a small cerebellum or hydrocephalus (increased fluid within the brain), can be visualized by ultrasound or other imaging techniques. However, some neurologic problems may only be noticed through their physical effects. For example, difficulties in feeding and breathing, hypertonic muscles, a diminished response to sound, seizures, and severe mental retardation all indicate serious neurologic deficits. Spina bifida (open spine) is an infrequent but serious problem affecting the spinal cord. Babies with spina bifida usually have some degree of paralysis below the point on the back where the spine failed to close.
Diagnosis
Prenatal
Two screening and two diagnostic procedures for trisomy 18 are available to women during pregnancy. Following are brief explanations of each of the prenatal testing alternatives.
Maternal serum alpha-fetoprotein (MSAFP)-Plus, also known as the “triple screen,” is a routine maternal blood test offered to women at 15-20 weeks of pregnancy. It screens for open defects (such as spina bifida), Down syndrome, and trisomy 18. However, the screen’s sensitivity for trisomy 18 is not as well established as it is for the other conditions. Test results provide a risk adjustment only, not a diagnosis of any condition in the fetus. Any woman who has a result showing an increased risk for trisomy 18 in the fetus is offered follow-up testing such as amniocentesis or a detailed (level II) ultrasound.
Ultrasound, also called sonography, visualizes structures inside the body using high frequency sound waves.
18 Trisomy
G A L E E N C Y C L O P E D I A O F G E N E T I C D I S O R D E R S |
1147 |

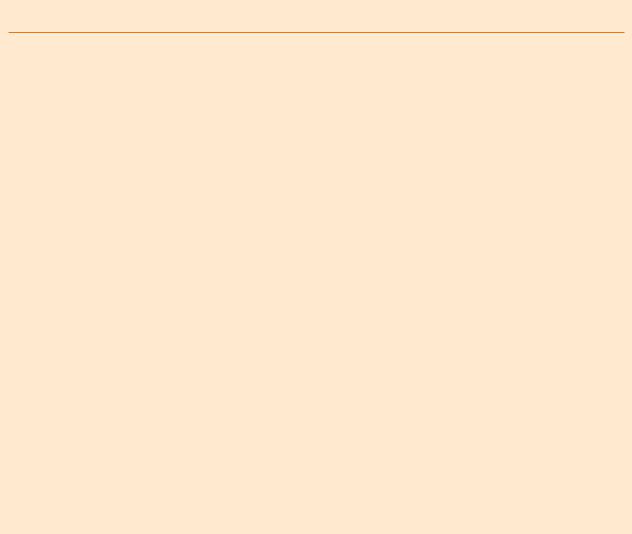
Trisomy 18
FISH (Fluorescent In Situ Hybridization) micrograph of Trisomy 18 chromosomes (green) in the nucleus of a cell (blue). In this image, the three copies of chromosome 18 are visible. (Photo Researchers, Inc.)
During a prenatal ultrasound, a technician or doctor moves an instrument (transducer) back and forth across the skin of a pregnant woman’s lower abdomen. The transducer emits and receives harmless high frequency sound waves, which the ultrasound machine then converts into images of the fetus. Today’s sophisticated ultrasound machines, used by skilled technicians and doctors, can detect a number of different physical anomalies in the fetus. An ultrasound screen for trisomy 18 has good (but not absolute) sensitivity, and presents no risk to the mother or fetus. Ultrasound becomes more sensitive for trisomy 18 the later in pregnancy it is performed. A level II ultrasound is performed after 20 weeks of pregnancy by a specialist (perinatologist). An abnormal ultrasound suggesting trisomy 18 would lead to the option of amniocentesis to confirm the diagnosis.
Chorionic villus sampling (CVS) is a method used to obtain tissue (chorionic villi) from the edge of the developing placenta. CVS is typically performed at 1012 weeks of pregnancy. Chorionic villi come from the fetal side of the placenta, and thus are chromosomally the same as cells in the fetus. Guided by ultrasound, a physician inserts a needle through either the abdomen or the cervix, into the placenta, and removes a small sample of tissue. Cells from the sample are analyzed under the microscope and a chromosome count is obtained. CVS carries a risk for miscarriage of approximately 1 in 150, and appears to have a very small risk of causing certain types of limb defects in the fetus as well. In about 3% of cases, CVS produces results that are difficult to interpret, which may lead to a follow-up amniocentesis.
Amniocentesis is the most widely used procedure to obtain fetal cells for genetic testing. The procedure can be performed anytime after about 15 weeks of pregnancy. Under ultrasound guidance, a physician passes a thin needle through the lower abdomen into the amniotic sac and removes a small amount of amniotic fluid. Fetal skin cells that normally float in the fluid are then extracted for genetic analysis. Diagnosis of chromosomal disorders by this method is highly accurate. Amniocentesis causes a miscarriage in about 1 in 300 women who have the procedure, but poses no other serious risk to the fetus.
The benefit of CVS and amniocentesis is their accuracy at detecting trisomy 18, while the drawback is their risk to the pregnancy. The procedures are typically not offered unless the risk for a chromosomal disorder in the fetus is greater than the risk of the procedure, such as in pregnant women who are 35 or older, a couple with a previous child with trisomy 18, and any woman who carries, or whose partner carries, a balanced chromosome translocation. Detection of fetal anomalies by ultrasound or an abnormal MSAFP-Plus screen would lead to the option of amniocentesis.
The benefit of ultrasound and MSAFP-Plus is their lack of risk to the pregnancy, while the drawback is that neither procedure is diagnostic. Women who wish to first modify their risk for a fetal chromosomal disorder (and spina bifida) may choose screening. In any case, prenatal testing, whether screening or diagnostic, is never mandatory. Careful consideration must always be given to what action might be taken after an abnormal result, and how reassuring a normal result might be.
Postnatal
A newborn with typical signs of Edwards syndrome can sometimes be diagnosed from a physical examination alone, especially by a physician who is familiar with the condition such as a geneticist or neonatologist. However, chromosome testing is the only method to confirm the diagnosis, and should always be performed if Edwards syndrome is suspected. Chromosome analysis helps to determine whether the underlying cause is full, mosaic, or partial trisomy 18, and may exclude other syndromes with similar signs and symptoms. Fetuses and newborns with Edwards syndrome sometimes die before chromosome analysis can be performed. In those cases, the diagnosis unfortunately cannot be confirmed, and an accurate cause and recurrence risk cannot be given.
Chromosome testing will detect full trisomy 18 with near 100% accuracy. Likewise, a translocation of chromosome 18 that produces signs of Edwards syn-
1148 |
G A L E E N C Y C L O P E D I A O F G E N E T I C D I S O R D E R S |
drome should be detected in virtually every case. Mosaic trisomy 18 presents more of a problem for chromosome analysis. The likelihood of confirming mosaic trisomy 18 depends on the percentage of trisomic cells in the particular tissue examined. Mosaicism, if present, can be confirmed by chromosome testing, and usually is. However, normal chromosome tests do not rule out the possibility of trisomic cells elsewhere in the body.
Treatment and management
Medical management of an infant with Edwards syndrome depends on the number and severity of anomalies present. In order to make the best-informed and most appropriate decisions for their child, parents must establish a close working relationship with the treating physicians.
Regardless of the medical procedures that might be performed, most babies with Edwards syndrome will not survive. Nearly all will be transferred to the neonatal intensive care unit (NICU) after birth. In some cases, parents elect not to have any life-prolonging, heroic measures taken should their child experience cardiac or respiratory failure. They may also elect not to have certain types of surgery performed if other complicating medical problems make it unwise.
A more medically stable, less severely affected infant with Edwards syndrome will likely require various medical procedures and treatments. Surgical repair of certain physical anomalies, ventilator (breathing) support, medications, and/or placement of a feeding tube into the stomach are common. A baby may go home and remain there after some length of hospital stay, or may need to be readmitted one or more times. For those children that show some possibility of longerterm survival (more than six months), a plan for their medical care, both in the hospital and at home, must be established. Parents should also be informed of the various educational and support services available to them, including the Support Organization For Trisomy 18, 13, and Related Disorders (S.O.F.T.). Genetic counseling, to discuss the cause, prognosis, and recurrence risks for their child’s type of trisomy 18, can be of great help to parents.
There is no way to prevent the occurrence of trisomy 18. The technology now exists to test multiple embryos conceived by in vitro fertilization for certain chromosome anomalies, but this is very expen-
sive and is only performed at several centers in the world.
Prognosis
The prognosis for a baby born with trisomy 18 is poor. On average, about 40% of newborns with trisomy 18 survive the first week, 20% are alive at one month, 6% at six months, and about 5% live past their first birthday. Survival rates are somewhat higher for children with mosaic or partial trisomy 18. As is the case before birth, males with trisomy 18 have a higher mortality rate than females, with about one-third as many males as females surviving infancy.
The outlook for trisomy 18 is not likely to change much in the coming years. Surgery to repair various birth defects has improved dramatically over the years. However, most babies with trisomy 18 do not die from repairable anomalies. For those parents whose babies are expected to survive some length of time, connecting them with support groups and providing them with accurate information as soon as possible is important.
Resources
PERIODICALS
Baty, Bonnie J., Brent L. Blackburn, and John C. Carey. “Natural History of Trisomy 18 and Trisomy 13: I. Growth, Physical Assessment, Medical Histories, Survival, and Recurrence Risk.” American Journal of Medical Genetics 49 (1994): 175-88.
Baty, Bonnie J., Brent L. Blackburn, and John C. Carey. “Natural History of Trisomy 18 and Trisomy 13: II. Psychomotor Development.” American Journal of Medical Genetics 49 (1994): 189-94.
Matthews, Anne L. “Chromosomal Abnormalities: Trisomy 18, Trisomy 13, Deletions, and Microdeletions.” Journal of
Perinatal and Neonatal Nursing 13 (1999): 59-75.
ORGANIZATIONS
Chromosome 18 Registry and Research Society. 6302 Fox Head, San Antonio, TX 78247. (210) 567-4968. http:// www.chromosome18.org .
National Society of Genetic Counselors. 233 Canterbury Dr., Wallingford, PA 19086-6617. (610) 872-1192. http:// www.nsgc.org/GeneticCounselingYou.asp .
Support Organization for Trisomy 18, 13 and Related Disorders (SOFT). 2982 South Union St., Rochester, NY 14624. (800) 716-SOFT. http://www.trisomy.org .
Scott J. Polzin, MS, CGC
Trisomy 21 see Down syndrome
18 Trisomy
G A L E E N C Y C L O P E D I A O F G E N E T I C D I S O R D E R S |
1149 |

Tuberous sclerosis complex
I Tuberous sclerosis complex
Definition
Tuberous sclerosis complex (TSC) is a genetic condition that affects many organ systems including the brain, skin, heart, kidneys, eyes, and lungs. Benign (noncancerous) growths or tumors called hamartomas form in various parts of the body, disrupting their normal functions.
Description
The term tuberous sclerosis refers to the small, knoblike growths in the brain of patients with TSC that were found in patients upon autopsy and, today, can be viewed using computed tomography (also called a CT scan). The condition is also referred to as tuberose sclerosis or simply tuberous sclerosis. The designation tuberous sclerosis complex is used to distinguish this condition from another genetic condition called Tourette syndrome that is abbreviated TS.
Persons with TSC have a variety of symptoms ranging from very mild to severe. Affected individuals may experience no serious health problems and, in the absence of a thorough clinical examination, may go through life without knowing that they are affected. Conversely, patients with TSC may have problems with behavioral, mental, and emotional functions as well as with their kidneys, heart, and eyes. In addition, specific skin abnormalities, often medically insignificant, are among the most common symptoms of TSC.
Genetic profile
TSC is an autosomal dominant genetic disorder caused by a single change or alteration in a gene called a mutation in either the TSC1 gene, located on chromosome 9, or the TSC2 gene, located on chromosome 16. Approximately two-thirds (66%) of patients with TSC have it as the result of a new change in one of the TSC genes; that is, it was not inherited from one of their parents. When a new change occurs, it most commonly occurs in the TSC2 gene. An individual must have a mutation in one of these two copies of a TSC-causing gene in order to develop the condition. In addition, a person who has been diagnosed with TSC and who, therefore, has a genetic mutation in one of the TSC genes, has a 50% chance of passing on the genetic mutation to his or her offspring. Laboratory testing for changes in the TSC genes is not currently available.
TSC is a condition that can be caused by a change in either one of two separate genes. In addition, people who
have the same change in the same gene may have very different medical problems and symptoms.
TSC1 is responsible for producing the protein hamartin and TSC2, tuberin. Both genes are known as tumor suppressor genes meaning that their normal function is to prevent the growth of tumors. Conversely, when gene function is altered, tumor growth results. Research on how the disruption of either protein results in the clinical condition of TSC is ongoing.
It is currently believed that every person who inherits or develops a mutation in either the TSC1 or TSC2 gene will develop some form of TSC. However, the severity of the disease, with its wide range of symptoms and complications, cannot accurately be predicted by identifying the specific gene mutation.
Germline mosaicism can explain the rare occurrence of unaffected parents having more than one child with TSC. Germline refers to the gonadal cells (sperm in males and eggs in females) and mosaicism refers to the presence of different cell lines in any given individual. A person with germline mosaicism for either the TSC1 or TSC2 gene is not affected with TSC but may have an affected child. Unaffected parents of a child with TSC are quoted a 2-3% chance of having additional affected children. Typical genetic testing methods are performed on somatic (non-germline) tissues such as blood or skin and, therefore, will not detect germline mosaicism.
Demographics
Although tuberous sclerosis complex is considered to be a rare condition, estimates of the prevalence of the disorder have increased as clinical testing methods have improved. In the United States, as many as one child in 6,000 born is affected with TSC and about 50,000 people are currently living in the U.S. with the disease. TSC is seen in all ethnic groups and populations and, worldwide, there are between one and two million cases.
Signs and symptoms
The basic underlying cause for illness and, less often, death due to tuberous sclerosis complex is the development of growths called hamartomas throughout the body. Hamartoma is a general term used to describe tumor-like growths that are not cancerous and are composed of cells usually found in that site but poorly developed. While these growths are typically benign (i.e., not cancerous), their presence often disrupts the normal functions of a particular organ system. The various hamartomas found in TSC patients can be further distinguished and classified by their location and their histo-
1150 |
G A L E E N C Y C L O P E D I A O F G E N E T I C D I S O R D E R S |
K E Y T E R M S
Bone cysts—Fluid- or air-filled space within the bones.
Cardiac rhabdomyoma—Benign (non-cancerous) tumor of the heart muscle.
Cerebral white matter migration lines—Pattern of defects found in the cerebral cortex of the brain probably caused by abnormal migration of neurons during brain formation.
Confetti skin lesions—Numerous light or white spots seen on the skin that resemble confetti.
Cortical tuber—Round (nodular) growth found in the cortex of the brain.
Dental pits—Small, shallow holes or crevices in the tooth enamel.
Facial angiofibromas—Benign (non-cancerous) tumors of the face.
Forehead plaque—Flat, fibrous skin growth on the forehead.
Gingival fibromas—Fibrous growths found on the gums.
Hamartomatous rectal polyps—Benign (non-can- cerous) growths found in the rectum.
Hypomelanotic macules—Patches of skin lighter than the surrounding skin.
Lymphangiomyomatosis—Serious lung disease characterized by the overgrowth of an unusual type
of muscle cell resulting in the blockage of air, blood, and lymph vessels to and from the lungs.
Nonrenal hamartoma—Benign (non-cancerous) tumor-like growths not found in the kidneys that often disrupt the normal function of a particular organ system.
Nontraumatic ungual or periungual fibroma—
Fibrous growth that appears around the fingernails and/or toenails
Renal angiomyolipoma—Benign (non-cancerous) tumors in the kidney that are made up of vascular tissue (angio), smooth muscle (myo), and fat (lipoma).
Renal cysts—Fluid- or air-filled spaces within the kidneys.
Retinal achromic patch—Defect in the coloration of the retina.
Retinal hamartomas—Benign (non-cancerous) tumor found on the retina.
Shagreen patch—Area of tough and dimpled skin.
Subependymal giant cell astrocytoma—Benign (non-cancerous) tumor of the brain comprised of star-shaped cells (astrocytes).
Subependymal nodule—Growth found underneath the lining of the ventricles in the brain.
logical properties—that is, their physical composition and characteristic appearance under a microscope. As each hamartoma is comprised of different cellular elements, each one has a particular name. For example, while both are hamartomas, a fibroma is comprised of connective tissue whereas a lipoma is made up of fat cells.
While the organs affected vary from person to person, most people with TSC have some type of skin irregularities called lesions. Some of the most commonly seen skin lesions are hypomelanotic macules—white or light patches sometimes in an ash-leaf shape and called Ashleaf spots. Many people in the general population have one or two light areas of skin. However, the presence of three or more such macules in any one individual is considered a major diagnostic finding of TSC. A second major diagnostic feature of the condition is the appearance of small, red bumps called fibromas, either on the
face (facial angiofibromas) or around or under the fingeror toenails (ungual fibromas). In addition, rough patches of skin termed Shagreen patches are highly specific to a diagnosis of TSC. Finally, groups of small light circles called Confetti spots are considered a minor feature of the disorder.
In contrast to skin lesions, brain lesions tend to be serious and are responsible for the neurological symptoms and cognitive impairment seen in severely affected individuals. There are four primary abnormalities that can be detected by magnetic resonance imaging (MRI) or computer tomography (CT) scanning, the first of which are cortical tubers—nodular growths found in the cortex of the brain—and give tuberous sclerosis (literally “hard growths”) its name. Subependymal nodules are growths found underneath the lining of the ventricles in the brain and may cause no problems for the patient unless they grow or begin to block the flow of the cerebral spinal
complex sclerosis Tuberous
G A L E E N C Y C L O P E D I A O F G E N E T I C D I S O R D E R S |
1151 |

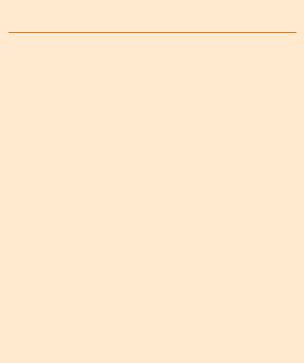
Tuberous sclerosis complex
A common sign of tuberous sclerosis is skin lesions called hypomelanotic macules. These are white or light patches of skin sometimes in an ash-leaf shape and called Ash-leaf spots. (Custom Medical Stock Photo, Inc.)
fluid. In contrast, subependymal giant cell astrocytomas, non-cancerous brain tumors comprised of star-shaped cells and found in about 5% of patients with TSC, can, if untreated, result in blindness, hydrocephalus (fluid on the brain), and even death. Finally, cerebral white matter migration lines may be seen through radiographic (x ray) studies and are considered a minor diagnostic feature of TSC.
About 85% of affected individuals will develop epileptic seizures at some point in their lifetime, most beginning by the first year of life. Research suggests that early control of epilepsy by medication will decrease the chance of a child developing serious mental complications. People with TSC have a range of mental abilities from normal to mild or moderate developmental delays and learning disabilities, to severe mental retardation.
Autism, attention deficit hyperactivity disorder (ADHD), and other behavioral problems are seen in affected individuals.
Fatty kidney tumors, known as renal angiomyolipomas, are one of the most common findings in TSC patients, affecting 70-80% of older children and adults, and often cause serious renal malfunction. In addition, the presence of multiple renal cysts (fluid filled areas within the kidneys) is suggestive of the condition. In addition to these benign growths, malignant kidney tumors may also develop.
The most common cardiac symptom is one or more tumors (cardiac rhabdomyomas) in the heart. These tumors are almost exclusively seen in infants and young children and usually spontaneously disappear by late childhood, thereby avoiding the need for surgery. About 47-67% of infants and children with TSC have heart tumors and some females develop the rhabdomyomas when they reach puberty.
Tuberous sclerosis complex affects the eyes in the form of retinal nodular hamartomas—multiple growths on the retina. A discoloration on the retina (retinal achromic patch) is also considered a minor feature of the condition.
In addition to the above, symptoms of TSC may include dental pits in the teeth, growths in the rectum (hamartomatous rectal polyps), bone cysts, growths on the gums (gingival fibromas) and other non-specific growths (nonrenal hamartomas). Women with TSC may develop lymphangiomyomatosis, a serious lung disease. Furthermore, all individuals with TSC are at a higher risk over the general population for developing specific cancers, with 2% of patients developing a malignant tumor in one of the affected body tissues such as kidney or brain.
Diagnosis
When a person exhibits signs of TSC or has a family history of the condition, an evaluation by a medical geneticist, neurologist, or other qualified professional is recommended to confirm (or rule out) the diagnosis and to recommend screening and management options for the individual. In addition, speaking with a genetic counselor may help families understand the genetics behind the disorder, their recurrence risks (chances for having another affected family member) and the practical and psychosocial implications of the disease on their personal situation.
Detection of hypomelanotic macules (light patches on the skin) can be performed quickly and easily using a special ultraviolet lamp called a Wood’s lamp. This light emphasizes the lightened areas on the skin that may otherwise be difficult to see using normal light. Other skin lesions called fibromas are easily visible and identifiable due to their characteristic smooth form, red color, and their even distribution on the face and/or their protrusions among the nails on the fingers and toes. Radiographic imaging using ultrasound, MRI, or CT technology can detect growths present in the brain, kidneys, heart, and eyes.
As basic understanding of and testing methods for tuberous sclerosis complex have improved, criteria used for confirming a diagnosis of tuberous sclerosis complex have been revised. The National Institutes of Health
1152 |
G A L E E N C Y C L O P E D I A O F G E N E T I C D I S O R D E R S |
(NIH) held a consensus conference on TSC in 1998 and published the following diagnostic criteria in 2000:
Major features:
•Facial angiofibromas or forehead plaque
•Nontraumatic ungual or periungual fibroma
•Hypomelanotic macules (more than three)
•Shagreen patch
•Multiple retinal hamartomas
•Cortical tuber
•Subependymal nodule
•Subependymal giant cell astrocytoma
•Cardiac rhabdomyoma (one or more)
•Lymphangiomyomatosis
•Renal angiomyolipoma
Minor features:
•Multiple randomly distributed dental pits
•Hamartomatous rectal polyps
•Bone cysts
•Cerebral white matter migration lines
•Gingival fibromas
•Nonrenal hamartoma
•Retinal achromic patch
•Confetti skin lesions
•Multiple renal cysts
A confirmed diagnosis of TSC requires that a patient display either two major features or one major and two minor features, a suspected diagnosis one major and one minor feature, and a possible diagnosis one major or two minor features in any one individual.
Treatment and management
Optimal treatment for TSC is dependent upon proper disease management. The following should be performed on all patients with TSC at the time of diagnosis to confirm a diagnosis of the disease as well as obtain baseline medical data for future evaluations:
•dermatologic (skin) examination
•fundoscopic (eye) examination
•renal (kidney) imaging study
•cardiac electrocardiogram (ECG) and echocardiogram (ECHO)
•brain magnetic resonance imaging (MRI)
Since the characteristic feature of tuberous sclerosis complex is the growth of benign tumors, treatments are often focused on appropriate surgical interventions to arrest tumor growth or remove tumors whose growth has resulted in or may lead to medical complications especially in the kidney or brain. Regular brain MRI studies should be performed in children and adults with previous findings as clinically indicated and every one to three years in children and, less frequently, in adults without symptoms. In addition, periodic brain electroencephalogram (EEG) studies are recommended for both children and adult patients when clinically indicated.
Children without previous kidney findings should be offered renal imaging studies using ultrasound, MRI, or CT scanning every three years until they reach adolescence and then, every one to three years as adults. Likewise, asymptomatic adults should have imaging of their kidneys every one to three years. Both children and adults who have kidney symptoms should be monitored using imaging studies every six months to one year until the tumor growth stabilizes or decreases.
Any child with cardiac rhabdomyomas should be monitored every six months to one year until the tumor stabilizes or regresses completely. Adults with previous findings of cardiac tumors should be monitored as clinically recommended by their treating physician. While monitoring is important, cardiac rhabdomyomas, as well as retinal lesions and gingival fibromas, usually do not require treatment. In contrast to these benign tumors, cancerous tumors that develop in patients with TSC should be treated by an oncologist as appropriate.
Facial angiofibromas and periand subungual fibromas on the nails are common symptoms in TSC patients. While they are generally not medically significant, they can cause skin irritations or be a cosmetic concern to the individual. Special techniques involving dermabrasion or laser therapy can be performed by a dermatologist or plastic surgeon to remove such growths.
Patients with seizure disorders are prescribed specific medications to control seizures. As of 2001, a new anti-epileptic drug (vigabatrin) has been shown to be an effective medication in infants with seizures and has been shown to improve long-term outcomes in behavioral and intellectual areas. In addition to controlling seizures, early intervention programs that include special education, behavior modification, physical and occupational therapies, and speech therapy is often recommended for individuals with learning disabilities, developmental delays, mental retardation, autism, and other mental and emotional disorders.
complex sclerosis Tuberous
G A L E E N C Y C L O P E D I A O F G E N E T I C D I S O R D E R S |
1153 |

Turner syndrome
Neurodevelopmental testing is appropriate at the time of diagnosis for all children and should be performed every three years until adolescence and for any adult diagnosed with TSC who displays signs of impairment. Subsequent evaluations should be done on both children and adults with previous findings of developmental delays or problems.
While present in only 1% of patients with TSC, almost exclusively in females, lung complications can be serious and even fatal. Symptoms may include spontaneous pneumothorax (air in the chest cavity), dyspnea (difficult breathing), cough, hemoptysis (spitting of blood), and pulmonary failure. Therefore, a computed tomography (CT) scan of the lungs is recommended for any TSC patient who has symptoms of lung disease or complications and for all female TSC patients at the age of 18. Clinical trials involving Tamoxifen and progesterone treatments have shown positive results in some patients with lung disease.
Prognosis
The lifespan of individuals with TSC varies with the severity of the condition in any one person. Many affected people have normal life expectancies and a high quality of life, relatively free of symptoms or complication of the disease. Conversely, severely affected or disabled individuals may experience a shortened lifespan and a high rate of illness and medical complications. Therefore, proper disease management, diagnostic monitoring, and follow-up are critical to achieving and maintaining optimal health in patients with TSC.
Resources
BOOKS
Gomez, Manuel R., ed. Tuberous Sclerosis. New York: Raven Press, 1988.
Gomez, Manuel R., Julian R. Sampson, and Vicky H. Whittemore, eds. Tuberous Sclerosis Complex. Oxford: Oxford University Press, 1999.
Johnson, William G., and Manuel R. Gomez, eds. Tuberous
Sclerosis and Allied Disorders: Clinical, Cellular, and Molecular Studies. New York: The New York Academy of Sciences, 1991.
PERIODICALS
Arbuckle, H. Alan, and Joseph G. Morelli. “Pigmentary Disorders: Update on Neurofibromatosis-1 and Tuberous Sclerosis.” Current Opinion in Pediatrics 12 (2000): 354358.
Hyman, Mark H., and Vicky H. Whittemore. “National Institutes of Health Consensus Conference: Tuberous Sclerosis Complex.” Archives of Neurology 57 (May 2000): 662-665.
Jambaque, I., et al. “Mental and Behavioural Outcome of Infantile Epilepsy Treated by Vigabatrin in Tuberous Sclerosis Patients.” Epilepsy Research 38 (2000): 151-160.
O’Callaghan, Finbar J., and John P. Osborne. “Advances in the Understanding of Tuberous Sclerosis.” Archives of Disease in Childhood 83 (August 2000): 140-142.
Sparagana, Steven P., and E. Steve Roach. “Tuberous Sclerosis Complex.” Current Opinion in Neurology 13 (2000):115119.
ORGANIZATIONS
Tuberous Sclerosis Alliance. 801 Roeder Rd., Suite 750, Silver Spring, MD 20910. (800) 225-6872. http://www.tsalliance.org .
WEBSITES
Australasian Tuberous Sclerosis Society.
http://www.netspace.net.au/~atss/ .
The Global Tuberous Sclerosis Information Link.
http://members.aol.com/gtsil/ts/index.htm .
Tuberous Sclerosis Alliance. http://www.tsalliance.org .
The Tuberous Sclerosis Association.
http://www.tuberous-sclerosis.org/ .
Pamela E. Cohen, MS, CGC
Turcot syndrome see Familial adenomatous polyposis
I Turner syndrome
Definition
Turner syndrome is a chromosomal disorder affecting females wherein one of the two X-chromosomes is defective or completely absent.
Description
Chromosomes are structures in the nucleus of every cell in the human body. Chromosomes contain the genetic information necessary to direct the growth and normal functioning of all cells and systems of the body. A normal individual has a total of 46 chromosomes in each cell, two of which are responsible for determining gender. Normally, females have two X chromosomes and males have one X and one Y chromosome.
In Turner syndrome, an error occurring very early in development results in an abnormal number and arrangement of chromosomes. Most commonly, an individual with Turner syndrome will be born with 45 chromosomes in each cell rather than 46. The missing chromosome is an X chromosome. The affected person is always female.
1154 |
G A L E E N C Y C L O P E D I A O F G E N E T I C D I S O R D E R S |
Genetic profile
Turner syndrome is a disorder associated with characteristic defects in the X chromosome. The most common presentation is a female with a single X chromosome and an absent X chromosome. A Greek study from 1999 reported that the intact X chromosome was as likely to come from the mother as from the father. This means that there is no parental pattern of responsibility for the missing or defective X chromosome.
Another less common genetic pattern for Turner syndrome (35%) is a mosaic. A Danish study reported that mosaicism has an effect on malformations that are associated with Turner syndrome. Research reported in 1997 noted that the karyotype can have a significant effect on the growth of children with Turner syndrome.
The exact location of the genes on the X chromosome involved in Turner syndrome has not been determined as of 2001. At present, evidence exists that there is a locus for stature on the distal portion of the short arm; there are loci for normal ovarian function on both the short and long arms; and there are loci contributing to fetal viability on the long arm of X.
K E Y T E R M S
Chromosome—A microscopic thread-like structure found within each cell of the body that consists of a complex of proteins and DNA. Humans have 46 chromosomes arranged into 23 pairs. Changes in either the total number of chromosomes or their shape and size (structure) may lead to physical or mental abnormalities.
Mosaic—A term referring to a genetic situation in which an individual’s cells do not have the exact same composition of chromosomes. In Down syndrome, this may mean that some of the individual’s cells have a normal 46 chromosomes, while other cells have an abnormal 47 chromosomes.
Ovary—The female reproductive organ that produces the reproductive cell (ovum) and female hormones.
Zygote—The cell formed by the uniting of egg and sperm.
Demographics
The prevalence of Turner syndrome is widely reported as being approximately one per 2,000 live female births although researchers have reported prevalence rates that range from one in 3,125 to one in 5,000 live female births.
About 1-2% of all female conceptions have a missing X chromosome. Of these, the majority (99%) spontaneously abort, usually during the first trimester of pregnancy. With ultrasound being used more frequently, researchers have realized that some pregnancies with a missing X chromosome that progress into the second trimester are associated with nuchal cysts, severe lymphedema, or hydrops fetalis. These pregnancies are associated with a high frequency of fetal death.
Signs and symptoms
Turner syndrome is characterized by delayed growth that leads to a small stature and frequent infertility. Individuals with Turner syndrome report an increased incidence of fractures in childhood and osteoporotic fractures in adulthood. The incidence of diabetes mellitus (both insulin dependent and non-insulin dependent varieties) has been reported to be increased in Turner syndrome. Ischemic heart disease, stroke, and hypertension are also more common.
Growth in children with Turner syndrome is characterized by a slight intrauterine growth retardation, relatively normal growth rates for the first several years of life, a progressive deceleration of growth later in childhood, and the lack of a pubertal growth spurt. Growth patterns of Chinese girls with Turner syndrome parallel those of Caucasians, although their ultimate height is still less than normal.
Contrary to earlier reports, most individuals with Turner syndrome are not mentally retarded. They may have some learning disabilities, particularly with regard to spatial perception, visual-motor coordination, and mathematics. As a result, the nonverbal IQ in Turner syndrome tends to be lower than the verbal IQ.
Cardiovascular malformations are well-recognized congenital anomalies in Turner syndrome. Dilation and dissection of the aorta are reported in approximately half of women with Turner syndrome. Because of the potential consequences of aortic dilation, some experts recommend screening all individuals with Turner syndrome. However, the specific timing for this screening remains controversial in 2001.
Juvenile arthritis, an autoimmune condition, has been recently (1998) associated with Turner syndrome. The prevalence seems to be at least six times greater than would be expected if the two conditions were only randomly associated. Women with Turner syndrome have an
syndrome Turner
G A L E E N C Y C L O P E D I A O F G E N E T I C D I S O R D E R S |
1155 |