334 |
12 Urinary Tract Infection in Infants and Children |
|
|
•Children with grade IV or V VUR or a significantly abnormal renal and urinary bladder ultrasound should be evaluated further for a possible surgical management.
•Constipation should be addressed in infants and children who have had a UTI to help prevent subsequent infections.
•There is some evidence that cranberry juice decreases symptomatic UTIs over 12-months, particularly in women with recurrent UTIs.
•The effectiveness of cranberry juice in children is less certain, and the high dropout rate in studies indicates that cranberry juice may not be acceptable for long-term prevention.
Antibiotics used for prophylaxis
Antibiotic |
Single daily dose |
Sulfamethoxazole and |
5–10 mg/kg SMZ, |
trimethoprim (SMZ-TMP) |
1–2 mg/kg TMP |
|
PO |
Trimethoprim |
1–2 mg/kg PO |
Nitrofurantoin |
1–2 mg/kg PO |
|
|
Cephalexin |
10 mg/kg PO |
Further Reading
1. [Guideline] Subcommittee on Urinary Tract Infection; Steering Committee on Quality Improvement and Management. Urinary tract infection: clinical practice guideline for the diagnosis and management of the initial UTI in febrile infants and children 2 to 24 months. Pediatrics. 2011.
2. American Academy of Pediatrics Task Force on Circumcision. Circumcision policy statement. Pediatrics. 2012;130(3):585–6.
3.American Academy of Pediatrics, Subcommittee on Urinary Tract Infection, Steering Committee on Quality Improvement and Management, Roberts KB. Urinary tract infection: clinical practice guideline for diagnosis and management of the initial UTI in febrile infants and children 2 to 24 months. Pediatrics. 2011;128(3):595–610.
4.Bloomfield P, Hodson EM, Craig JC. Antibiotics for acute pyelonephritis in children. Cochrane Database
Syst Rev. 2005;(1):CD003772.
5. Finnell SM, Carroll AE, Downs SM. Technical report—diagnosis and management of an initial UTI in febrile infants and young children. Pediatrics. 2011;128(3):e749–70.
6. Garin EH, Olavarria F, Garcia Nieto V, Valenciano B, Campos A, Young L. Clinical significance of primary
vesicoureteral reflux and urinary antibiotic prophylaxis after acute pyelonephritis: a multicenter, randomized, controlled study. Pediatrics. 2006;117(3): 626–32.
7. Girardet P, Frutiger P, Lang R. Urinary tract infections in pediatric practice. A comparative study of three diagnostic tools: dip-slides, bacterioscopy and leucocyturia. Paediatrician. 1980;9(5–6):322–37.
8. Glissmeyer EW, Korgenski EK, Wilkes J, et al. Dipstick screening for urinary tract infection in febrile infants. Pediats. 2014;133(5):e1121–7.
9. Goldsmith BM, Campos JM. Comparison of urine dipstick, microscopy, and culture for the detection of bacteriuria in children. Clin Pediatr (Phila). 1990;29(4):214–8.
10. Heldrich FJ, Barone MA, Spiegler E. UTI: diagnosis and evaluation in symptomatic pediatric patients. Clin Pediatr (Phila). 2000;39(8):461–72.
11. Hoberman A, Charron M, Hickey RW, Baskin M, Kearney DH, Wald ER. Imaging studies after a first febrile urinary tract infection in young children. N Engl J Med. 2003;348(3):195–202.
12. Hoberman A, Wald ER, Hickey RW, et al. Oral versus initial intravenous therapy for urinary tract infections in young febrile children. Pediatrics. 1999;104(1 pt 1):79–86.
13. Hom J. Are oral antibiotics equivalent to intravenous antibiotics for the initial management of pyeloneophritis in children? Pediatr Child Health. 2010;15(3): 150–2.
14. Jepson RG, Williams G, Craig JC. Cranberries for preventing urinary tract infections. Cochrane Database Syst Rev. 2012;(10):CD001321.
15.Keren R, Chan E. A meta-analysis of randomized, controlled trials comparing shortand long-course
antibiotic therapy for urinary tract infections in children. Pediatrics. 2002;109(5), E70.
16. Lunn A, Holden S, Boswell T, Watson AR. Automated microscopy, dipsticks and the diagnosis of urinary tract infection. Arch Dis Child. 2010;95(3):193–7.
17.Michael M, Hodson EM, Craig JC, Martin S, Moyer VA. Short versus standard duration oral antibiotic therapy for acute urinary tract infection in children. Cochrane Database Syst Rev.
2003;(1):CD003966.
18. Montini G, Toffolo A, Zucchetta P, et al. Antibiotic treatment for pyelonephritis in children: multicentre randomised controlled non-inferiority trial. BMJ. 2007;335(7616):386.
19.Mori R, Lakhanpaul M, Verrier-Jones K. Diagnosis and management of urinary tract infection in children:
summary of NICE guidance. BMJ. 2007;335(7616): 395–7.
20. Pennesi M, Travan L, Peratoner L, Bordugo A, Cattaneo A, Ronfani L, et al. Is antibiotic prophylaxis in children with vesicoureteral reflux effective in preventing pyelonephritis and renal scars? A randomized, controlled trial. Pediatrics. 2008;121(6): e1489–94.
Further Reading |
335 |
|
|
21. Salo J, Ikäheimo R, Tapiainen T, Uhari M. Childhood urinary tract infections as a cause of chronic kidney disease. Pediatrics. 2011;128(5):840–7.
22. Schoen EJ, Colby CJ, Ray GT. Newborn circumcision decreases incidence and costs of urinary tract infections during the first year of life. Pediatrics. 2000;105(4 Pt 1):789–93.
23. Schroeder AR, Chang PW, Shen MW, Biondi EA, Greenhow TL. Diagnostic accuracy of the urinalysis for urinary tract infection in infants <3 months of age. Pediatrics. 2015;135(6):965–71.
24. Shaikh N, Morone NE, Bost JE, Farrell MH. Prevalence of urinary tract infection in childhood: a meta-analysis. Pediatr Infect Dis J. 2008;27(4): 302–8.
25.Singh-Grewal D, Macdessi J, Craig J. Circumcision for the prevention of urinary tract infection in boys. Arch Dis Child. 2005;90(8):853–8.
26.Supavekin S, Surapaitoolkorn W, Pravisithikul N, Kutanavanishapong S, Chiewvit S. The role of DMSA renal scintigraphy in the first episode of urinary tract infection in childhood. Ann Nucl Med. 2013;27(2): 170–6.
27.Toffolo A, Ammenti A, Montini G. Long-term clinical consequences of urinary tract infections during childhood: a review. Acta Paediatr. 2012;101(10): 1018–31.
28. Tosif S, Baker A, Oakley E, Donath S, Babl FE. Contamination rates of different urine collection methods for the diagnosis of urinary tract infections in young children: an observational cohort study. Paediatr Child Health. 2012;48(8):659–64.
29. Tran D, Muchant DG, Aronoff SC. Short-course versus conventional length antimicrobial therapy for uncomplicated lower urinary tract infections in children: a meta-analysis of 1279 patients. J Pediatr. 2001;139(1):93–9.
30.Wald ER. Vesicoureteral reflux: the role of antibiotic prophylaxis. Pediatrics. 2006;117(3):919–22.
31. Wan J, Skoog SJ, Hulbert WC, Casale AJ, Greenfield SP, Cheng EY, et al. Section on Urology response to new Guidelines for the diagnosis and management of UTI. Pediatrics. 2012;129(4):e1051–3.
32. Whiting P, Westwood M, Watt I, Cooper J, Kleijnen J. Rapid tests and urine sampling techniques for the diagnosis of urinary tract infection (UTI) in children under five years: a systematic review. BMC Pediatr. 2005;5(1):4.
33. Williams G, Craig JC. Long-term antibiotics for preventing recurrent urinary tract infection in children. Cochrane Database Syst Rev. 2011;(3):CD001534.
34. Zorc JJ, Kiddoo DA, Shaw KN. Diagnosis and management of pediatric urinary tract infections. Clin Microbiol Rev. 2005;18(2):417–22.

Bladder Exstrophy-Epispadias |
13 |
Complex |
13.1Introduction
•Bladder exstrophy (also known as Ectopia vesicae) is a congenital anomaly that exists as part of the exstrophy-epispadias complex.
•It is characterized by protrusion of the open urinary bladder through a defect in the lower abdominal wall.
•Bladder exstrophy-epispadias complex is a spectrum of rare congenital malformations involving the urinary, genital, and musculoskeletal systems in which the bladder remains open through a lower abdominal defect.
•Bladder exstrophy-epispadias-cloacal exstrophy complex is the most severe and comprises a spectrum of anomalies involving the urinary
tract, genital tract, musculoskeletal system and sometimes the intestinal tract.
•The bladder exstrophy-epispadias complex comprises a spectrum of congenital abnormalities that includes (Figs. 13.1 and 13.2):
–Classic bladder exstrophy
–Epispadias
–Cloacal exstrophy
–Other rare variants
–The spectrum often include abnormalities of the bony pelvis, pelvic floor, and genitalia
•The underlying embryologic mechanism leading to this spectrum of anomalies is unknown but it is believed that all represent a spectrum of the same embryological defect. It is thought to result from failed reinforcement of the cloacal membrane by underlying mesoderm.
|
SMALL OMPHALOCELE |
|
|
|
|
|
|
|
|
|
|
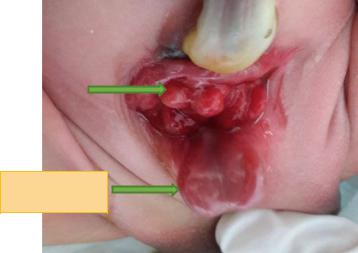
Fig. 13.1 A clinical |
|
|
|
|
|
½ URINARY |
|
|
|
|
|
|
|
|
½ URINARY |
||
photograph showing |
|
|
|
||
BLADDER |
|
|
|
||
|
|
|
BLADDER |
||
classic cloacal |
|
|
|
|
|
exstrophy. Note the |
|
|
|
|
|
open urinary bladder |
|
|
|
|
|
into two halves and the |
|
|
|
|
|
ileocecal region |
|
|
|
|
|
protruding in the |
|
|
|
|
|
middle of the bladder. |
|
|
|
|
|
Note the small |
|
|
|
ILEOCECAL REGION |
|
omphalocele |
|
|
|
|
|
© Springer International Publishing Switzerland 2017 |
337 |
||||
A.H. Al-Salem, An Illustrated Guide to Pediatric Urology, DOI 10.1007/978-3-319-44182-5_13