

202 |
6 Congenital Ureteral Anomalies |
|
|
–Bladder capacity may be improved with enterocystoplasty.
–A variety of bladder outlet procedures have been described:
•Young-Dees-Leadbetter bladder neck reconstruction
•Kropp procedure
•Pubovaginal sling
•Bladder neck closure
•Artificial urinary sphincter
•Duplex system:
–Treatment depends on the function of the involved upper pole and whether VUR is present.
–If function is adequate, an ureteropyelostomy (upper-pole ureter to lower-pole renal pelvis) or ureteroureterostomy (upper-pole ureter to lower-pole ureter) is performed if no VUR is noted in the lower pole ureter.
–In patients with a functioning upper-pole system and coexisting lower-pole VUR, a common sheath ureteral reimplantation is performed.
–If the upper-pole moiety is nonfunctional, a partial nephroureterectomy is performed and the upper-pole ureter is removed to the pelvic brim.
–If patients have coexisting upper-pole VUR, the ureteral stump should be ligated to prevent reflux of urine into the retroperitoneum.
–The more distal the ureter insertion, the worse the prognosis.
6.6Ureterocele
6.6.1Introduction
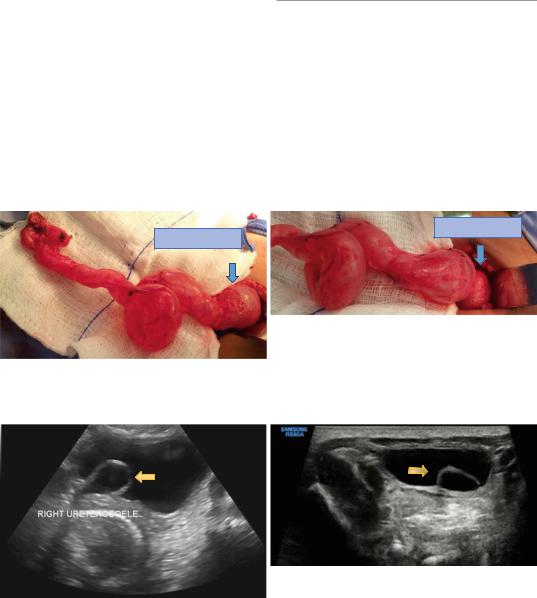
•A ureterocele is a congenital saccular dilatation of the distal segment of the ureter (Figs. 6.20, 6.21, 6.22, and 6.23).
•This anomaly most frequently involves the upper pole of a duplex system.
•A ureterocele contained within the bladder is called an orthotopic ureterocele.
URETEROCE
URETEROCE
Figs. 6.20 and 6.21 Clinical intraoperative photographs showing ureterocele. Note the associated severely dilated ureter. Note also the small atrophic dysplastic kidney
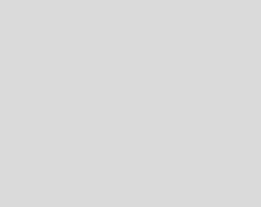
Figs. 6.22 and 6.23 Pelvic ultrasound showing right and left ureterocele
6.6 Ureterocele |
203 |
|
|
•Sometimes, the ureterocele extends beyond the bladder into the urethra.
•This is called an ectopic ureterocele.
•These patients may present with a cystic mass at the urethral meatus representing a prolapsed ureterocele.
•Ureteroceles are often associated with obstruction and VUR.
•The incidence of ureterocele is approximately 1 in 4,000 children.
•Approximately 80 % occur in females.
•Approximately 10 % are bilateral.
•Approximately 80 % are associated with duplicated collecting systems with single system ureteroceles being more common in males and adults.
•Indications for surgical interventions include:
– Obstruction
– Urosepsis or compromised renal function may necessitate urgent decompression prior to definitive surgical reconstruction
6.6.2Classification
•The AAP classification of ureteroceles:
–Intravesical ureteroceles
–Ectopic ureteroceles
•Stephens et al. classification of ureteroceles:
–Stenotic ureterocele (40 %):
•This is the most common type of ureterocele.
•The ureterocele lies within the bladder.
•Its orifice lies within the trigone and is obstructive.
•It corresponds to an intravesical ureterocele.
–Sphincteric ureterocele (30 %):
•In this form of ureterocele, a rather dilated ureter courses through the submucosa of the bladder, and adopts a more normal caliber as it travels into the urethra.
•It has an opening at the level of the sphincter.
•Its orifice is not narrow, but drainage from the ureterocele is impaired by contraction of the sphincter.
•The associated ureterocele can be very large.
–Sphincterostenotic ureterocele (6 %):
•The ureterocele has an orifice at the level of the sphincter.
•Its narrow orifice further impedes its drainage so that the ureterocele remains dilated and obstructs the bladder outlet.
–Blind ureterocele (5 %):
•This form of ureterocele extends under the trigone and into the bladder outlet.
•No opening is identifiable.
•The dilated ureterocele can cause severe bladder outlet obstruction.
–Non-obstructive ureterocele (5 %):
•This type of ureterocele lies entirely within the bladder, and has a large opening which does not impede drainage of the ureterocele.
–Caecoureterocele (5 %):
•This form of ureterocele extends submucosally into the urethra.
•The orifice of the ureterocele lies more proximally either in the urethra or the bladder.
•A “tongue” of submucosal ureterocele lies caudal to the opening.
•If its opening is small, filling of the ureterocele may obstruct the bladder outlet.
•If the ureterocele has a large opening (either naturally or iatrogenically) the tongue of the caecoureterocele will fill by reflux during voiding and may obstruct the urethra.
Classification of Ureteroceles
•The AAP classification:
–Intravesical ureterocele
–Ectopic ureterocele
•The Stephens et al. classification:
–Stenotic ureterocele (40 %)
–Sphincteric ureterocele (30 %)
–Sphincterostenotic ureterocele (6 %)
–Blind ureterocele (5 %)
–Non-Obstructive ureterocele (5 %)
–Caecoureterocele (5 %)

204 |
6 Congenital Ureteral Anomalies |
|
|
6.6.3Clinical Features
•The exact incidence of ureterocele is not known and at post-mortem, ureterocele was estimated to occur 1 in 500–4,000.
•In patients with duplex kidneys, ureterocele is found in 5–20 %.
•With the wide spread use of antenatal ultrasound, half to three quarters of ureteroceles are detected antenatally.
–It is common for ureteroceles to obstruct the upper pole of the affected kidney from which they have arisen.
–The lower pole ureter may be obstructed by the dilated upper pole ureter.
–A ureterocele that obstructs the bladder outlet will affect the contralateral kidney as well.
•Ureteroceles may be associated with vesicoureteral reflux which affect the ipsilateral lower pole in half, and the contralateral kidney in a quarter.
•Abnormal bladder function is common in children with ureterocele.
–More than half will have abnormally large bladders, and residual volumes are common.
–Stones have been observed in a large proportion of adult patients presenting with ureterocele.
6.6.4Investigations and Diagnosis
•The aims of investigating patients with ureteroceles are:
–To confirm the diagnosis
–To determine its structure (intravesical or ectopic)
–To identifying coexisting pathology:
•VUR
•Lower pole and bladder outlet obstruction
•Abdominal and pelvic ultrasound (Figs. 6.24, 6.25 and 6.26):
–The ureterocele and its associated dilated ureter and upper pole are usually identified on ultrasound.
Figs. 6.24, 6.25, and 6.26 Abdominal and pelvic ultrasounds showing right ureterocele