

1.3 Abnormalities of the Kidney |
11 |
|
|
1.3.6Simple (Solitary) Renal Cyst
•Numerous renal cysts are seen in the cystic kidney diseases, which include polycystic kidney disease and medullary sponge kidney.
•Simple renal cysts are different from these cysts.
•A renal cyst is an abnormal fluid collection in the kidney.
•Simple kidney cysts do not enlarge the kidneys, replace their normal structure, or cause reduced kidney function like PKD.
•Significant renal damage is rare in these cysts and usually only requires continuous followup and no surgical interventions.
•There are several types of renal cysts based on the Bosniak classification.
•The Bosniak classification categorizes renal cysts into five groups.
–Category I:
•Benign simple cyst with thin wall without septa, calcifications, or solid components.
•It does not enhance with contrast, and has a density equal to that of water.
–Category II:
•Benign cyst with a few thin septa, which may contain fine calcifications or a small segment of mildly thickened calcification.
•This includes homogenous, highattenuation lesions less than 3 cm with sharp margins but without enhancement.
•Hyperdense cysts must be exophytic with at least 75 % of its wall outside the kidney to allow for appropriate assessment of margins, otherwise they are categorized as IIF.
–Category IIF:
•Up to 5 % of these cysts are malignant and as such they require follow-up imaging, though there is no consensus recommendation on the appropriate interval of follow up.
•Well marginated cysts with a number of thin septa, with or without mild enhancement or thickening of septa.
•Calcifications may be present; these may be thick and nodular. There are no enhancing soft tissue components.
•This also includes nonenhancing highattenuation lesions that are completely
contained within the kidney and are 3 cm or larger.
–Category III:
•Indeterminate cystic masses with thickened irregular septa with enhancement.
•50 % of these lesions are ultimately found to be malignant.
–Category IV:
•Malignant cystic masses with all the characteristics of category III lesions but also with enhancing soft tissue components independent of but adjacent to the septa.
•100 % of these lesions are malignant.
•The majority are benign, simple cysts that can be monitored. However, some are cancerous or are suspicious for cancer and these are removed.
•Simple renal cysts are more common as people age. An estimated 25 % of people 40 years of age and 50 % of people 50 years of age have simple kidney cysts.
•The cause of simple kidney cysts is not fully understood and several theories were proposed.
–Obstruction of tubules
–Deficiency of blood supply to the kidneys may play a role.
–Diverticula sacs that form on the tubules, may detach and become simple kidney cysts.
•Simple kidney cysts usually do not cause symptoms or negatively affect the kidneys.
•In some cases, however, pain can develop when cysts enlarge and press on other organs.
•Most simple kidney cysts are found during imaging tests done for other reasons.
•Sometimes cysts become infected, causing fever, pain, and tenderness.
•Some studies have found a relationship between simple kidney cysts and high blood pressure.
12 |
1 Congenital Urological Malformations |
|
|
•When a cyst is found, the following imaging tests can be used to differentiate between simple and complicated renal cysts.
–Abdominal ultrasound
–CT-scan
–MRI
•Simple renal cysts that do not cause any symptoms require no treatment and can be monitored with periodic ultrasounds.
•Symptomatic simple renal cysts can be treated with ultrasound guided sclerotherapy.
•Large symptomatic simple renal cysts can be drained and deroofed laparoscopically.
•Parapelvic cysts:
–Parapelvic cysts originate from around the kidney at the adjacent renal parenchyma, and plunge into the renal sinus.
•Peripelvic cysts:
–Peripelvic cysts are contained entirely within the renal sinus, possibly related to dilated lymphatic channels.
–They can mimic hydronephrosis when viewed on CT in absence of contrast.
1.3.7Renal Fusion and Renal Ectopia
•Renal ectopy and fusion are common congenital anomalies of the kidney and urinary tract, and result from disruption of the normal embryologic migration of the kidneys.
•Although children with these anomalies are generally asymptomatic, some children develop symptoms due to complications, such as infection, renal calculi, and urinary obstruction (Figs. 1.13, 1.14, 1.15, 1.16, 1.17, and 1.18).
•The most frequent abnormality seen is a horseshoe kidney containing two excretory systems and two ureters.
•They are usually asymptomatic but are prone to obstruction.
1.3.8Horseshoe Kidney
•A horseshoe kidney is formed by fusion across the midline of two distinct functioning kidneys, one on each side of the midline.
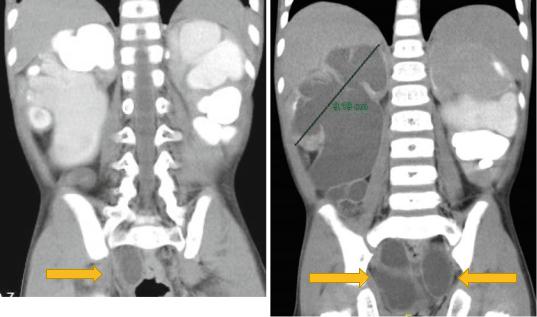
Figs. 1.13 and 1.14 CT-urography showing bilateral duplex kidney with hydroueters. Note the associated hydronephrosis and the massively dilated ureters
1.3 Abnormalities of the Kidney |
13 |
|
|
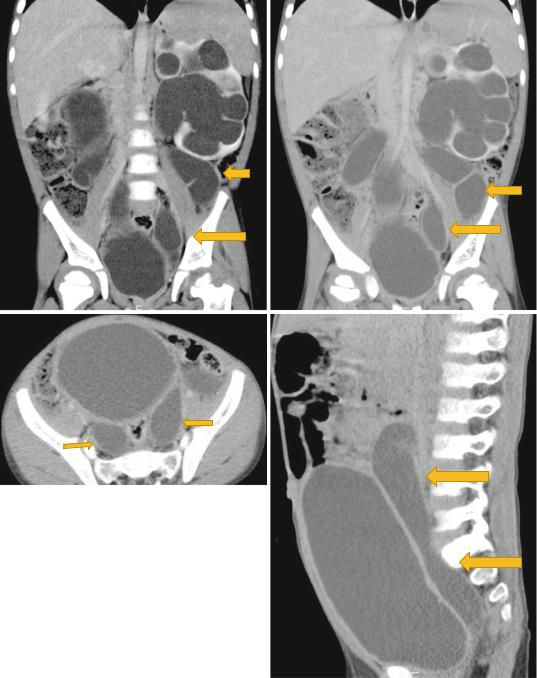
Figs. 1.15, 1.16, 1.17, and 1.18 CT-urography showing duplex kidneys with hydronephrosis and hydroureters
14 |
1 Congenital Urological Malformations |
|
|
•They are connected by an isthmus of either functioning renal parenchyma or fibrous tissue.
•In the vast majority of cases the fusion is between the lower poles (90 %).
•In the remainder the superior or both the superior or inferior poles are fused. This latter configuration is referred to as a sigmoid kidney.
–The kidneys develop in the pelvis and migrate up to their final position in the retroperitoneal space in the lumbar region.
•Prior to their ascent, the renal capsule has not matured and the kidneys still lie within the pelvis.
•It is suggested that abnormal flexion or growth of the developing spine and pelvic organs brings the immature kidneys together for a longer period than usual, leading to fusion of the two renal elements and hence forming the so-called horseshoe kidney.
•As this abnormal fusion occurs in the pelvis, the subsequent kidney cannot undergo normal migration and rotation.
•In the normal kidneys, the lower poles of the kidneys rotate laterally. However, with a horseshoe kidney, these poles remain medially positioned.
•The horseshoe kidney cannot migrate to the usual position because the fusion will not allow passage by the inferior mesenteric artery.
•Horseshoed kidney is the most common type of fusion anomaly.
•For the most part, the horseshoe kidney functions as a normal kidney. Many times, kidney malformations are accompanied by lower urinary tract anomalies as well.
•With horseshoe kidney, the kidneys can be located anywhere along the normal embryologic ascent of the kidneys.
•In 90 % of cases, the fusion of the kidneys occurs in the lower poles. In this condition, both kidneys are malrotated and their lower poles are joined.
•The collection system of a horseshoe kidney is usually deviated inwards at the lower poles because of the fusion with the isthmus.
•The ureters arise from the kidneys anterior rather than medially.
•The ureter also has a higher insertion point into the renal pelvis than that of a normal kidney.
•The blood supply to the horseshoe kidney is also different than most kidneys. There is actually several different ways that it can receive its supply. The blood supply could arise from the aorta, the iliac arteries and the inferior mesenteric artery. And it could occur as one of these, or a combination of all of them. Although in 65 % of the cases, the isthmus is supplied by single vessel from the aorta.
•It has been estimated that 22–24.8 % of patients with horseshoe kidney also have a renal vein anomaly as well. The most common of these is multiple right renal veins.
•The kidneys are joined by an isthmus which links the lower poles in 95 % of cases and the upper poles in 5 %.
•The isthmus may be fibrotic, dysplastic, or normal renal parenchyma.
•The position of the isthmus is variable.
•The isthmus lies at level of L4 just below the origin of the inferior mesenteric artery (IMA) in 40 %.
•The presence of the IMA may restrict further ascent of the horseshoe during early embryogenesis.
•In another 40 % the kidneys the isthmus is located in a normal anatomical position, whilst the kidneys lie lower in the pelvis in the remaining 20 %.
•Malrotation of the kidneys is always present and is attributed to early fusion prior to normal rotation.
•The renal pelvices remain anterior, with the ureters crossing the isthmus.
•The blood supply to horseshoe kidneys is extremely variable.
–Thirty percent have a normal anatomical pattern
–The remaining 70 % are supplied by a combination of vessels entering from the aorta or the renal, mesenteric, iliac, or sacral arteries.
–The isthmus frequently has separate blood vessels that may occasionally represent the entire renal blood supply.