

- •Preface
- •Acknowledgments
- •Contents
- •1.1 Introduction
- •1.2 Normal Embryology
- •1.3 Abnormalities of the Kidney
- •1.3.1 Renal Agenesis
- •1.3.2 Renal Hypoplasia
- •1.3.3 Supernumerary Kidneys
- •1.3.5 Polycystic Kidney Disease
- •1.3.6 Simple (Solitary) Renal Cyst
- •1.3.7 Renal Fusion and Renal Ectopia
- •1.3.8 Horseshoe Kidney
- •1.3.9 Crossed Fused Renal Ectopia
- •1.4 Abnormalities of the Ureter
- •1.5 Abnormalities of the Bladder
- •1.6 Abnormalities of the Penis and Urethra in Males
- •1.7 Abnormalities of Female External Genitalia
- •Further Reading
- •2.1 Introduction
- •2.2 Pathophysiology
- •2.3 Etiology of Hydronephrosis
- •2.5 Clinical Features
- •2.6 Investigations and Diagnosis
- •2.7 Treatment
- •2.8 Antenatal Hydronephrosis
- •Further Reading
- •3.1 Introduction
- •3.2 Embryology
- •3.3 Pathophysiology
- •3.4 Etiology of PUJ Obstruction
- •3.5 Clinical Features
- •3.6 Diagnosis and Investigations
- •3.7 Management of Newborns with PUJ Obstruction
- •3.8 Treatment
- •3.9 Post-operative Complications and Follow-Up
- •Further Reading
- •4: Renal Tumors in Children
- •4.1 Introduction
- •4.2 Wilms’ Tumor
- •4.2.1 Introduction
- •4.2.2 Etiology
- •4.2.3 Histopathology
- •4.2.4 Nephroblastomatosis
- •4.2.5 Clinical Features
- •4.2.6 Risk Factors for Wilms’ Tumor
- •4.2.7 Staging of Wilms Tumor
- •4.2.8 Investigations
- •4.2.9 Prognosis and Complications of Wilms Tumor
- •4.2.10 Surgical Considerations
- •4.2.11 Surgical Complications
- •4.2.12 Prognosis and Outcome
- •4.2.13 Extrarenal Wilms’ Tumors
- •4.3 Mesoblastic Nephroma
- •4.3.1 Introduction
- •4.3.3 Epidemiology
- •4.3.5 Clinical Features
- •4.3.6 Investigations
- •4.3.7 Treatment and Prognosis
- •4.4 Clear Cell Sarcoma of the Kidney (CCSK)
- •4.4.1 Introduction
- •4.4.2 Pathophysiology
- •4.4.3 Clinical Features
- •4.4.4 Investigations
- •4.4.5 Histopathology
- •4.4.6 Treatment
- •4.4.7 Prognosis
- •4.5 Malignant Rhabdoid Tumor of the Kidney
- •4.5.1 Introduction
- •4.5.2 Etiology and Pathophysiology
- •4.5.3 Histologic Findings
- •4.5.4 Clinical Features
- •4.5.5 Investigations and Diagnosis
- •4.5.6 Treatment and Outcome
- •4.5.7 Mortality/Morbidity
- •4.6 Renal Cell Carcinoma in Children
- •4.6.1 Introduction
- •4.6.2 Histopathology
- •4.6.4 Staging
- •4.6.5 Clinical Features
- •4.6.6 Investigations
- •4.6.7 Management
- •4.6.8 Prognosis
- •4.7 Angiomyolipoma of the Kidney
- •4.7.1 Introduction
- •4.7.2 Histopathology
- •4.7.4 Clinical Features
- •4.7.5 Investigations
- •4.7.6 Treatment and Prognosis
- •4.8 Renal Lymphoma
- •4.8.1 Introduction
- •4.8.2 Etiology and Pathogenesis
- •4.8.3 Diagnosis
- •4.8.4 Clinical Features
- •4.8.5 Treatment and Prognosis
- •4.9 Ossifying Renal Tumor of Infancy
- •4.10 Metanephric Adenoma
- •4.10.1 Introduction
- •4.10.2 Histopathology
- •4.10.3 Diagnosis
- •4.10.4 Clinical Features
- •4.10.5 Treatment
- •4.11 Multilocular Cystic Renal Tumor
- •Further Reading
- •Wilms’ Tumor
- •Mesoblastic Nephroma
- •Renal Cell Carcinoma in Children
- •Angiomyolipoma of the Kidney
- •Renal Lymphoma
- •Ossifying Renal Tumor of Infancy
- •Metanephric Adenoma
- •Multilocular Cystic Renal Tumor
- •5.1 Introduction
- •5.2 Embryology
- •5.4 Histologic Findings
- •5.7 Associated Anomalies
- •5.8 Clinical Features
- •5.9 Investigations
- •5.10 Treatment
- •Further Reading
- •6: Congenital Ureteral Anomalies
- •6.1 Etiology
- •6.2 Clinical Features
- •6.3 Investigations and Diagnosis
- •6.4 Duplex (Duplicated) System
- •6.4.1 Introduction
- •6.4.3 Clinical Features
- •6.4.4 Investigations
- •6.4.5 Treatment and Prognosis
- •6.5 Ectopic Ureter
- •6.5.1 Introduction
- •6.5.3 Clinical Features
- •6.5.4 Diagnosis
- •6.5.5 Surgical Treatment
- •6.6 Ureterocele
- •6.6.1 Introduction
- •6.6.3 Clinical Features
- •6.6.4 Investigations and Diagnosis
- •6.6.5 Treatment
- •6.6.5.1 Surgical Interventions
- •6.8 Mega Ureter
- •Further Reading
- •7: Congenital Megaureter
- •7.1 Introduction
- •7.3 Etiology and Pathophysiology
- •7.4 Clinical Presentation
- •7.5 Investigations and Diagnosis
- •7.6 Treatment and Prognosis
- •7.7 Complications
- •Further Reading
- •8.1 Introduction
- •8.2 Pathophysiology
- •8.4 Etiology of VUR
- •8.5 Clinical Features
- •8.6 Investigations
- •8.7 Management
- •8.7.1 Medical Treatment of VUR
- •8.7.2 Antibiotics Used for Prophylaxis
- •8.7.3 Anticholinergics
- •8.7.4 Surveillance
- •8.8 Surgical Therapy of VUR
- •8.8.1 Indications for Surgical Interventions
- •8.8.2 Indications for Surgical Interventions Based on Age at Diagnosis and the Presence or Absence of Renal Lesions
- •8.8.3 Endoscopic Injection
- •8.8.4 Surgical Management
- •8.9 Mortality/Morbidity
- •Further Reading
- •9: Pediatric Urolithiasis
- •9.1 Introduction
- •9.2 Etiology
- •9.4 Clinical Features
- •9.5 Investigations
- •9.6 Complications of Urolithiasis
- •9.7 Management
- •Further Reading
- •10.1 Introduction
- •10.2 Embryology of Persistent Müllerian Duct Syndrome
- •10.3 Etiology and Inheritance of PMDS
- •10.5 Clinical Features
- •10.6 Treatment
- •10.7 Prognosis
- •Further Reading
- •11.1 Introduction
- •11.2 Physiology and Bladder Function
- •11.2.1 Micturition
- •11.3 Pathophysiological Changes of NBSD
- •11.4 Etiology and Clinical Features
- •11.5 Investigations and Diagnosis
- •11.7 Management
- •11.8 Clean Intermittent Catheterization
- •11.9 Anticholinergics
- •11.10 Botulinum Toxin Type A
- •11.11 Tricyclic Antidepressant Drugs
- •11.12 Surgical Management
- •Further Reading
- •12.1 Introduction
- •12.2 Etiology
- •12.3 Pathophysiology
- •12.4 Clinical Features
- •12.5 Investigations and Diagnosis
- •12.6 Management
- •Further Reading
- •13.1 Introduction
- •13.2 Embryology
- •13.3 Epispadias
- •13.3.1 Introduction
- •13.3.2 Etiology
- •13.3.4 Treatment
- •13.3.6 Female Epispadias
- •13.3.7 Surgical Repair of Female Epispadias
- •13.3.8 Prognosis
- •13.4 Bladder Exstrophy
- •13.4.1 Introduction
- •13.4.2 Associated Anomalies
- •13.4.3 Principles of Surgical Management of Bladder Exstrophy
- •13.4.4 Evaluation and Management
- •13.5 Cloacal Exstrophy
- •13.5.1 Introduction
- •13.5.2 Skeletal Changes in Cloacal Exstrophy
- •13.5.3 Etiology and Pathogenesis
- •13.5.4 Prenatal Diagnosis
- •13.5.5 Associated Anomalies
- •13.5.8 Surgical Reconstruction
- •13.5.9 Management of Urinary Incontinence
- •13.5.10 Prognosis
- •13.5.11 Complications
- •Further Reading
- •14.1 Introduction
- •14.2 Etiology
- •14.3 Clinical Features
- •14.4 Associated Anomalies
- •14.5 Diagnosis
- •14.6 Treatment and Prognosis
- •Further Reading
- •15: Cloacal Anomalies
- •15.1 Introduction
- •15.2 Associated Anomalies
- •15.4 Clinical Features
- •15.5 Investigations
- •Further Reading
- •16: Urachal Remnants
- •16.1 Introduction
- •16.2 Embryology
- •16.4 Clinical Features
- •16.5 Tumors and Urachal Remnants
- •16.6 Management
- •Further Reading
- •17: Inguinal Hernias and Hydroceles
- •17.1 Introduction
- •17.2 Inguinal Hernia
- •17.2.1 Incidence
- •17.2.2 Etiology
- •17.2.3 Clinical Features
- •17.2.4 Variants of Hernia
- •17.2.6 Treatment
- •17.2.7 Complications of Inguinal Herniotomy
- •17.3 Hydrocele
- •17.3.1 Embryology
- •17.3.3 Treatment
- •Further Reading
- •18: Cloacal Exstrophy
- •18.1 Introduction
- •18.2 Etiology and Pathogenesis
- •18.3 Associated Anomalies
- •18.4 Clinical Features and Management
- •Further Reading
- •19: Posterior Urethral Valve
- •19.1 Introduction
- •19.2 Embryology
- •19.3 Pathophysiology
- •19.5 Clinical Features
- •19.6 Investigations and Diagnosis
- •19.7 Management
- •19.8 Medications Used in Patients with PUV
- •19.10 Long-Term Outcomes
- •19.10.3 Bladder Dysfunction
- •19.10.4 Renal Transplantation
- •19.10.5 Fertility
- •Further Reading
- •20.1 Introduction
- •20.2 Embryology
- •20.4 Clinical Features
- •20.5 Investigations
- •20.6 Treatment
- •20.7 The Müllerian Duct Cyst
- •Further Reading
- •21: Hypospadias
- •21.1 Introduction
- •21.2 Effects of Hypospadias
- •21.3 Embryology
- •21.4 Etiology of Hypospadias
- •21.5 Associated Anomalies
- •21.7 Clinical Features of Hypospadias
- •21.8 Treatment
- •21.9 Urinary Diversion
- •21.10 Postoperative Complications
- •Further Reading
- •22: Male Circumcision
- •22.1 Introduction
- •22.2 Anatomy and Pathophysiology
- •22.3 History of Circumcision
- •22.4 Pain Management
- •22.5 Indications for Circumcision
- •22.6 Contraindications to Circumcision
- •22.7 Surgical Procedure
- •22.8 Complications of Circumcision
- •Further Reading
- •23: Priapism in Children
- •23.1 Introduction
- •23.2 Pathophysiology
- •23.3 Etiology
- •23.5 Clinical Features
- •23.6 Investigations
- •23.7 Management
- •23.8 Prognosis
- •23.9 Priapism and Sickle Cell Disease
- •23.9.1 Introduction
- •23.9.2 Epidemiology
- •23.9.4 Pathophysiology
- •23.9.5 Clinical Features
- •23.9.6 Treatment
- •23.9.7 Prevention of Stuttering Priapism
- •23.9.8 Complications of Priapism and Prognosis
- •Further Reading
- •24.1 Introduction
- •24.2 Embryology and Normal Testicular Development and Descent
- •24.4 Causes of Undescended Testes and Risk Factors
- •24.5 Histopathology
- •24.7 Clinical Features and Diagnosis
- •24.8 Treatment
- •24.8.1 Success of Surgical Treatment
- •24.9 Complications of Orchidopexy
- •24.10 Infertility and Undescended Testes
- •24.11 Undescended Testes and the Risk of Cancer
- •Further Reading
- •25: Varicocele
- •25.1 Introduction
- •25.2 Etiology
- •25.3 Pathophysiology
- •25.4 Grading of Varicoceles
- •25.5 Clinical Features
- •25.6 Diagnosis
- •25.7 Treatment
- •25.8 Postoperative Complications
- •25.9 Prognosis
- •Further Reading
- •26.1 Introduction
- •26.2 Etiology and Risk Factors
- •26.3 Diagnosis
- •26.4 Intermittent Testicular Torsion
- •26.6 Effects of Testicular Torsion
- •26.7 Clinical Features
- •26.8 Treatment
- •26.9.1 Introduction
- •26.9.2 Etiology of Extravaginal Torsion
- •26.9.3 Clinical Features
- •26.9.4 Treatment
- •26.10 Torsion of the Testicular or Epididymal Appendage
- •26.10.1 Introduction
- •26.10.2 Embryology
- •26.10.3 Clinical Features
- •26.10.4 Investigations and Treatment
- •Further Reading
- •27: Testicular Tumors in Children
- •27.1 Introduction
- •27.4 Etiology of Testicular Tumors
- •27.5 Clinical Features
- •27.6 Staging
- •27.6.1 Regional Lymph Node Staging
- •27.7 Investigations
- •27.8 Treatment
- •27.9 Yolk Sac Tumor
- •27.10 Teratoma
- •27.11 Mixed Germ Cell Tumor
- •27.12 Stromal Tumors
- •27.13 Simple Testicular Cyst
- •27.14 Epidermoid Cysts
- •27.15 Testicular Microlithiasis (TM)
- •27.16 Gonadoblastoma
- •27.17 Cystic Dysplasia of the Testes
- •27.18 Leukemia and Lymphoma
- •27.19 Paratesticular Rhabdomyosarcoma
- •27.20 Prognosis and Outcome
- •Further Reading
- •28: Splenogonadal Fusion
- •28.1 Introduction
- •28.2 Etiology
- •28.4 Associated Anomalies
- •28.5 Clinical Features
- •28.6 Investigations
- •28.7 Treatment
- •Further Reading
- •29: Acute Scrotum
- •29.1 Introduction
- •29.2 Torsion of Testes
- •29.2.1 Introduction
- •29.2.3 Etiology
- •29.2.4 Clinical Features
- •29.2.5 Effects of Torsion of Testes
- •29.2.6 Investigations
- •29.2.7 Treatment
- •29.3 Torsion of the Testicular or Epididymal Appendage
- •29.3.1 Introduction
- •29.3.2 Embryology
- •29.3.3 Clinical Features
- •29.3.4 Investigations and Treatment
- •29.4.1 Introduction
- •29.4.2 Etiology
- •29.4.3 Clinical Features
- •29.4.4 Investigations and Treatment
- •29.5 Idiopathic Scrotal Edema
- •29.6 Testicular Trauma
- •29.7 Other Causes of Acute Scrotum
- •29.8 Splenogonadal Fusion
- •Further Reading
- •30.1 Introduction
- •30.2 Imperforate Hymen
- •30.3 Vaginal Atresia
- •30.5 Associated Anomalies
- •30.6 Embryology
- •30.7 Clinical Features
- •30.8 Investigations
- •30.9 Management
- •Further Reading
- •31: Disorders of Sexual Development
- •31.1 Introduction
- •31.2 Embryology
- •31.3 Sexual and Gonadal Differentiation
- •31.5 Evaluation of a Newborn with DSD
- •31.6 Diagnosis and Investigations
- •31.7 Management of Patients with DSD
- •31.8 Surgical Corrections of DSD
- •31.9 Congenital Adrenal Hyperplasia (CAH)
- •31.10 Androgen Insensitivity Syndrome (Testicular Feminization Syndrome)
- •31.13 Gonadal Dysgenesis
- •31.15 Ovotestis Disorders of Sexual Development
- •31.16 Other Rare Disorders of Sexual Development
- •Further Reading
- •Index
Disorders of Sexual Development |
31 |
|
31.1Introduction
•The birth of a new baby is one of the most dramatic events in a family, and the first question is usually “is it a boy or a girl?”
•When a child is born with ambiguous external genitalia it often comes as a surprise for the parents and diagnostic dilemma for the treating physicians.
•It is also considered as an endocrine emergency situation presenting a problem of sex assignment.
•It is important for clinicians to promptly make an accurate diagnosis and counsel parents on therapeutic options.
•It is also important to understand the psychological and social implications of gender assignment in some of these patients.
•In the past several names such as intersex or ambiguous genitalia were used to describe disorders of sexual development but they were not accurately descriptive.
•Intersex (Figs. 31.1, 31.2, 31.3, 31.4, 31.5, 31.6, and 31.7):
–Intersex literally means that the body is between the two sexes, male and female.
–This is a term that is no longer used; it has now been replaced by disorders of sexual development (DSD).
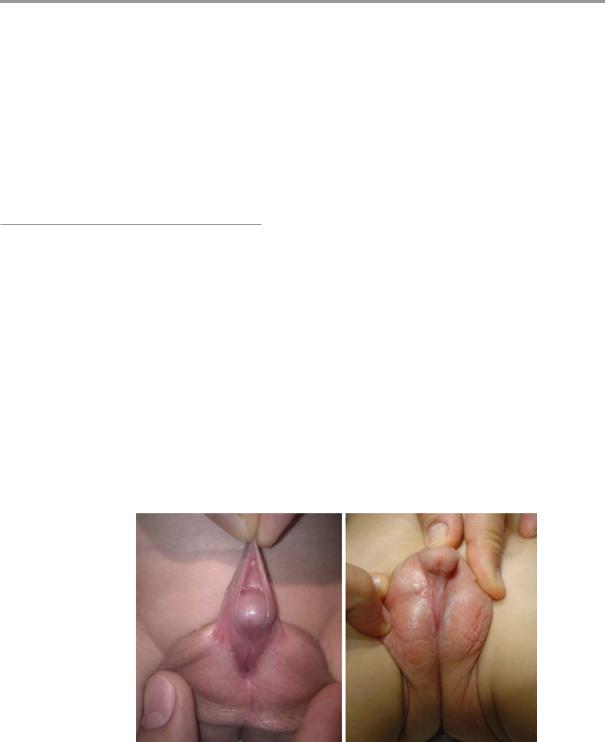
Figs. 31.1 and
31.2 Clinical photographs showing severe hypospadias with abnormal genitalia
© Springer International Publishing Switzerland 2017 |
635 |
A.H. Al-Salem, An Illustrated Guide to Pediatric Urology, DOI 10.1007/978-3-319-44182-5_31 |
|

636 |
31 Disorders of Sexual Development |
|
|
•In the past the term “hermaphrodite” was sometimes erroneously used to describe people with intersex/DSD conditions. The term hermaphroditism, was used after the Greek god of sexuality Hermes and the goddess of love and sexuality, Aphrodite. The correct technical definition of a hermaphrodite is a single organism that has complete sets of both male and female sexual organs. This term is also no longer used to describe humans.
•The nomenclatures such as ‘intersex’, ‘hermaphrodite’, and ‘pseudohermaphrodite’ are no longer used. They are confusing terms and
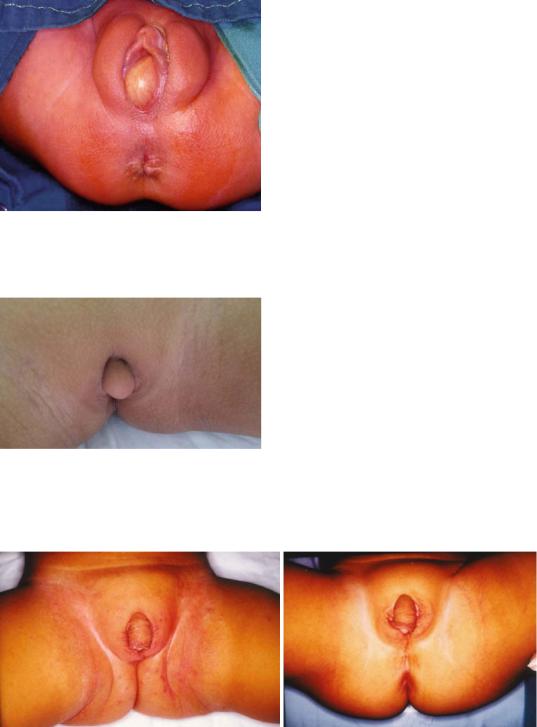
Fig. 31.3 A clinical photograph of a patient with DSD. It is difficult to decide whether this is a true male or not. This patient was investigated and found to have severe virilization secondary to congenital adrenal hyperplasia leading to enlargement of the clitoris resembling a male penis
Figs. 31.4 and
31.5 Clinical photographs of two new born with cloacal exstrophy. Note there are no clear external genitalia and these patients need further evaluation prior to sex assignment. The external genitalia in these patients are usually small and not well developed
could be perceived to be pejorative by some affected families.
•All these were replaced by the term Disorders of Sexual Development (DSD).
•This was coined by International Consensus Conference on Intersex organized by the Lawson Wilkins Pediatric Endocrine Society and the European Society for Pediatric Endocrinology in 2006.
•It replaces the earlier terms Intersex and ambiguous genitalia which were controversial and associated with a lot of social stigma and confusion.
•Disorders of sex development (DSD) are defined as congenital conditions in which development of chromosomal, gonadal, or anatomical sex is atypical.
•The use of the term disorder of sex development (DSD) is controversial among many activists and community organizations.
•Although there are potential criticisms to the new nomenclature, the DSD terminology has been generally accepted and is now popularly used in the literature.
•The medical term disorders of sex development (DSDs) is used to describe individuals with an atypical composition of chromosomal, gonadal and phenotypic sex, which leads to differences in the development of the urogenital tract and reproductive system.
•The term DSD has a comprehensive definition including any problem noted at birth in which
31.1 Introduction |
637 |
|
|
Fig. 31.6 Clinical photograph of a newborn with imperforated hymen with hydrocolpos causing abnormalities of external genitalia
Fig. 31.7 A clinical photograph showing abnormal external genitalis. This female patient was found to have a dermoid cyst over the clitoris causing abnormaliities of the external genitalia
the genitalia are atypical in relation to the chromosomes or gonads. The karyotype is used as a prefix defining the classification of DSD.
•The newly proposed terminology and classifications have eliminated some confusion for both the patient and the family, as well as for health professionals.
•DSDs are rare and complex.
•It is estimated that the overall incidence of DSDs is 1 in 4,500–5,500 live births.
•Congenital adrenal hyperplasia (CAH) and mixed gonadal dysgenesis are the most common causes of ambiguous genitalia, constituting approximately over 50 % of all cases of genital ambiguity in the newborn period (Figs. 31.8 and 31.9).
•The incidence of CAH and mixed gonadal dysgenesis is 1:15,000 and 1:10,000, respectively.
•Currently, many countries screen newborns for CAH by use of filter-paper blood spot 17-hydroxyprogesterone measurements.
•Disorders of sexual development includes a variety of conditions in which the reproductive system or the external genitalia are not normal for a female or male.
•There are three general descriptive terms to describe the sex of a person:
–Genotypic sex (Chromosomal sex): This refers to the sex based on the number of sex chromosomes. This depends on the presence of 46,XX or 46,XY chormosomes.
Figs. 31.8 and 31.9 Clinical photographs showing two patients with congenital adrenal hyperplasia. Note the abnormal external genitalia which show severe virilization
638 |
31 Disorders of Sexual Development |
|
|
–Anatomical sex (Gonadal sex): This refers to the sex according to the gonadal differentiation. This depends on the presence of a uterus, ovaries and tubes or testes, epididymis, seminal vesicles, ejaculatory ducts and prostate.
–Phenotypic sex: This refers to the sex based on the external anatomy of the genitalia. This results from the differentiation of the external genitalia under the influence of sex-determining genes and hormones.
•Abnormalities in any of these result in a range of conditions that lead to abnormal development of the sex organs and genitalia (Disorders of sex development).
•Children with DSD often have both male and female characteristics internally as well as externally.
•Gender identity:
–This refers to the individual’s perception about his/her own gender. In some individuals, gender identity is different from the phenotypic sex.
•When a child is born with DSD, the gender may not be obvious.
•The development of sex organs and external genitalia is a very complex process that starts at around 7–8 weeks of pregnancy in the developing fetus and is complete by 12 weeks.
•Great advances have been made over recent years in understanding the genetics and pathology of DSD.
•The Chicago Consensus new nomenclature is based on the primary genetic defect.
•It includes three broad categories: 1. Sex chromosome DSD
2. 46, XX DSD
3. 46, XY DSD
•The most common DSD is Congenital Adrenal Hyperplasia (CAH).
–This results in a female (XX chromosomes) having genitals that look somewhat masculine.
–In mild cases, CAH results in a slightly enlarged clitoris.
–In more severe cases it can be difficult to decide whether a baby is male or female.
–Most children with CAH think of themselves as girls.
–CAH when it occurs in males (XY chromosomes), the result is over-masculinization and premature puberty.
•Mixed gonadal dysgenesis (MGD) is the second most common cause of DSDs.
•Another common DSD is Androgen Insensitivity Syndrome (AIS).
–This occurs in males (XY chromosomes) who do not respond to testosterone normally.
–This results in a feminine appearance.
–There are two types, complete and partial.
–In Complete Androgen Insensitivity Syndrome (CAIS) the result is a totally feminine appearance, including typical female breast development.
–Diagnosis in 46,XY phenotypic females with complete androgen insensitivity usually occurs after puberty during an evaluation for primary amenorrhea.
–In the Partial Androgen Insensitivity Syndrome (PAIS), the genitals can vary from mostly female to almost completely male.
•One of the more unusual DSDs is 5-Alpha Reductase Deficiency (5ARD), popularly known as “Penis at 12.”
–It is caused by a deficiency of the enzyme 5-Alpha Reductase which converts testesterone to dihydrotestesterone in males (XY).
–Dihyrotestesterone is responsible for the development of the male external genitalia.
•The classic presentation of MIS (Mullerian inhibiting substance) deficiency is a boy with a hernia on one side and an impalpable contralateral gonad. At the time of surgery, a uterus and fallopian tubes are noted along with normal Wolffian structures.
•Clinicians should suspect the possibility of a DSD in patients with both hypospadias and cryptorchidism.
•Infants born with ambiguous genitalia represent a true medical and social emergency.