





















Section Ill • Gross Anatomy
Names of the Major Dural Sinuses
1 . Superior sagittal*
2.Inferior sagittal
3.Straight*
4.Transverse* (2)
5.Sigmoid (2)
6.Cavernous (2)
7.Superior petrosal (2)
* Drain into the confluence of sinuses located at the inion.
Folds (Duplications) of Dura Mater
A.Faix Cerebri
B.Tentorium Cerebelli
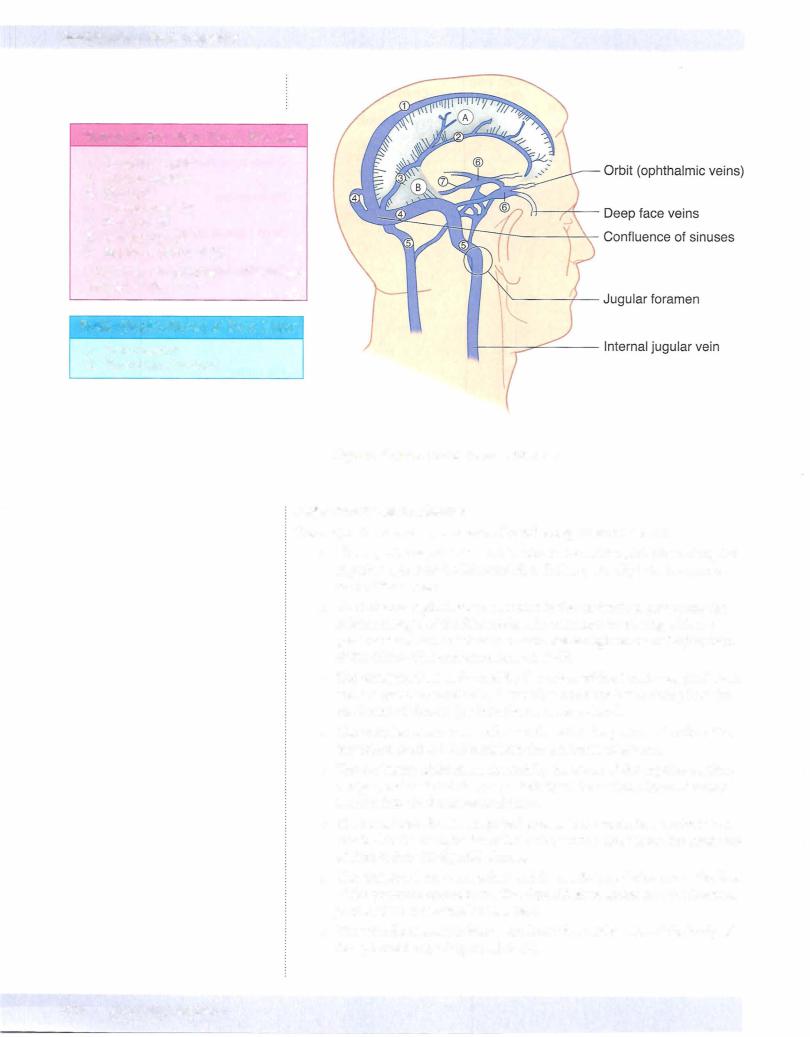
Figure 111-6-1 2. Dural Venous Sinuses
Major dural venous sinuses
The major dural venous sinuses are the following (Figure III-6- 12):
•The superior sagittal sinus is located in the midsagittal plane along the superior aspect of the falx cerebri. It drains primarily into the conflu ence of the sinuses.
•The inferior sagittal sinus is located in the midsagittal plane near the inferior margin of the falx cerebri. It terminates by joining with the great cerebral vein (of Galen) to form the straight sinus at the junction of the falx cerebri and tentorium cerebelli.
•The straight sinus is formed by the union of the inferior sagittal sinus and the great cerebral vein. It usually terminates by draining into the confluens of sinuses (or into the transverse sinus) .
•The occipital sinus is a small sinus found in the posterior border of the tentorium cerebelli. It drains into the confluens of sinuses.
•The confluens ofsinuses is formed by the union of the superior sagittal,
straight, and occipital sinuses posteriorly at the occipital bone. It drains laterally into the 2 transverse sinuses.
•The transversesinuses are paired sinuses in the tentorium cerebelli and attached to the occipital bone that drain venous blood from the confluens of sinuses into the sigmoid sinuses.
•The sigmoidsinuses are paired and form a S-shaped channel in the floor of the posterior cranial fossa. The sigmoid sinus drains into the internal jugularvein at the jugular foramen.
•The paired cavernous sinuses are located on either side of the body of the sphenoid bone (Figure III-6- 1 3) .
324 MEDICAL



Chapter 6 • Head and Neck
A. Epidural Hematoma* |
B. Subdural Hematoma* |
Figure 111-6-14. lntracranial Hemorrhage
Subarachnoid Hemorrhage
A subarachnoid hemorrhage results from a rupture of a berry aneurysm in the circle ofWillis. The most common site is in the anterior part ofthe circle ofWillis at the branch point ofthe anterior cerebral and anterior communicating arteries. Other common sites are in the proximal part of the middle cerebral artery or at the junction ofthe internal carotid and posterior communicating arteries.
•Typical presentation associated with a subarachnoid hemorrhage is the onset of a severe headache.
ORBITAL MUSCLES AND THEIR INNERVATION
In the orbit, thereare 6 ex.traocular muscles thatmovethe eyeball (Figure III-6-16).
A seventh muscle, the levator palpebrae superioris, elevates the upper eyelid.
•Pour ofthe 6 ex.traocular muscles (the superior, inferior, and medial rec tus, and the inferior oblique, plus the levatorpalpebrae superioris) are innervated by the oculomotor nerve (CN III).
•The superior oblique muscle is the only muscle innervated by the troch lear nerve (CN IV).
•The lateral rectus is the only muscle innervated by the abducens nerve (CN VI).
•The levator palpebrae superioris is composed ofskeletal muscle inner vated by the oculomotor nerve (CN III) and smooth muscle (the superior tarsal muscle) innervatedby sympathetic fibers.
•Sympathetic fibersreachthe orbit from a plexus on the internal carotid artery ofpostganglionic axons that originate from cell bodies in the supe rior cervical ganglion.
•The orbital muscles and their actions are illustrated in Figure III-6- 1 5.
MEDICAL 327



SECTION
Neuroscience




















