


various breeds. The myocardial performance index has been studied in Newfoundlands with DCM (129). Using pulsed-wave Doppler of mitral closure to opening time and left ventricular ejection time, this study found increased pre-ejection periods, shortened ejection time, and increased isovolumic relaxation and contraction time periods, with resultant significantly increased Tei index in dogs with overt DCM. Normal Newfoundlands had Tei indexes of .28 ± .12 while dogs with DCM had a Tei index of .51 ± .32. This parameter does not show any more specificity in differentiating normal from abnormal function, and it cannot reliably differentiate subclinical from normal hearts. Diastolic dysfunction with restrictive physiology is only present in these dogs with more advanced stages of dilated cardiomyopathy (129).
Right Ventricular Cardiomyopathy
Right ventricular dilated cardiomyopathy is typically an infiltrative disease involving fatty and fibrous replacement of myocytes after presumed cell death occurs (123,159,169,170). This entity is also called right ventricular dysplasia. The left side of the heart echocardiographically may appear normal even though histological changes may be present (171). There is severe right ventricular and atrial dilation with poor right ventricular systolic function and paradoxical septal motion secondary to the elevated right-sided diastolic pressures (Figure 7.46). Other signs of right-sided heart failure like pleural and pericardial effusion may be seen both radiographically and echocardiographically. There may be tricuspid insufficiency, and if present, spectral Doppler should be used to rule out pulmonary hypertension as a cause of the right-sided heart failure instead of cardiomyopathy. The foramen ovale may become patent when right atrial pressure become excessive (170). In man right ventricular cardiomyopathy is associated with highly irregular endocardial surfaces with prominent bulges and deep fissures (123,159). An arrhythmogenic form of this cardiomyopathy is reported in cats (169,171,172). Significant dilation of the right ventricle and atrium with systolic dysfunction and arrhythmia (ventricular tachyarrhythmia, atrioventricular block, atrial fibrillation) are seen in these cats that present in rightsided congestive heart failure (172). Arrhythmogenic right ventricular cardiomyopathy is reported in dogs, and Boxers have a predisposition to developing the right ventricular arrhythmias sometimes without echocardiographic evidence of abnormal myocardium or function (173–176).
Right Ventricular Cardiomyopathy
Features
RV dilation
RA dilation
Paradoxical septal motion
Irregular endocardial surface
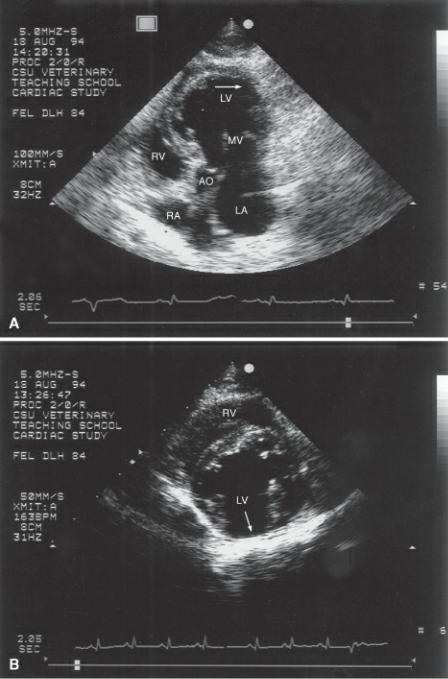
Figure 7.46 Right ventricular cardiomyopathy usually spares the left side of the heart. The right ventricle in both the M-mode image (a) and the right parasternal four chamber view (b) is dilated and functions poorly. The M-mode image also displays paradoxical septal motion. RV = right ventricle, RA = right atrium, LV = left ventricle, LA = left atrium, species = feline.

Restrictive Cardiomyopathy
Restrictive cardiomyopathy (RCM), found primarily in the cat, is poorly characterized and is sometimes called intermediate, intergrade, or unclassified cardiomyopathy (44). Restrictive cardiomyopathy is the preferred term however, and intermediate cardiomyopathy should be reserved for cases where the features of more than one type of cardiomyopathy exist and differentiation is not possible (177,178). Primary RCM is typically idiopathic with predominant diastolic failure secondary to infiltrative fibrosis of the myocardium (44,179). A less common form of RCM is endomyocardial fibrosis, an obliterative process (179). Secondary processes that may result in restrictive physiology include amyloid heart disease, hypertension, HCM, and DCM. Restrictive physiology is characterized by reduced ventricular compliance where diastolic filling is completed early in the diastolic time period (124,178,180,181).
Two-Dimensional Evaluation

Myocardial restrictive cardiomyopathy typically involves normal to near normal left ventricular chamber size and wall thicknesses with significant left atrial dilation (179,182,183). Echocardiographic features are not well documented nor does restrictive cardiomyopathy have uniformly accepted diagnostic criteria. Moderate to severe left atrial enlargement is one consistently required criteria for RCM however (44). Atrial enlargement may be seen only on the left, but typically both atria are involved. Atrial dilation occurs secondary to high left ventricular filling pressure and reduced ventricular compliance. There may be mild mitral insufficiency, but often there is no regurgitation at all (44,86,87,178,183,186). At times a thrombus is seen within the left atrial or auricular cavity (44,178). More often however the smoke-like echoes (spontaneous echo contrast) of sluggish blood may be seen within the atrial chamber (Figures 7.26, 7.47).
Restrictive Cardiomyopathy
Features
Left atrial dilation
Usually severe
Often with only mild mitral insufficiency
Hypertrophy only mild if present
Increased echogenicity in areas of myocardium (fibrosis)
Function normal early, becoming depressed as fibrosis develops
Figure 7.47 Very large atria are classically seen with restrictive cardiomyopathy. This atrium contains smoke-like echoes indicative of sluggish blood flow through the chamber (arrows). RA = right atrium, RV = right ventricle, LA = left atrium, AO = aorta, plane = right parasternal transverse heart base, species = feline.
Hypertrophy, if present, is mild, and left ventricular chamber size is usually normal but may be slightly increased. The endocardial surface is irregular with areas of the septum or free wall that are visibly thicker than other areas. There may be echogenic areas within the myocardium representing fibrosis, but this is not a consistent finding (Figure 7.48) (44,86,123,178). One uncommon form of restrictive cardiomyopathy involves endomyocardial scarring with connections between the septum
and left ventricular wall (179). There may be midventricular obstruction associated with this form of the disease as the fibrotic muscle becomes obliterative (179). There is usually fibrosis of the chordae and the papillary muscles resulting in mitral regurgitation. There may be evidence of myocardial infarction and involvement of the right side of the heart (179).
Figure 7.48 Irregular endocardial surfaces as well as small focal areas of fibrosis seen as bright hyperechoic areas are typically found in restrictive cardiomyopathies. (A) Apical five-chamber view of a heart with restrictive cardiomyopathy, (B) transverse left ventricular plane in a restrictive cardiomyopathy heart. There is also an area of infarcted muscle with aneurysmal dilation along the free wall (arrow) where the myocardium is almost nonexistent. RV = right ventricle, LV = left ventricle, RA = right atrium, AO = aorta, LA = left atrium, MV = mitral valve, species = feline.
When cats decompensate, right-sided heart changes become evident on the echocardiographic exam. These signs include right ventricular dilation with hypertrophy and pleural and pericardial effusions (44,178).
Evaluation of Function
Systolic left ventricular function in RCM is normal to mildly depressed with fractional shortenings above 22%. There may be areas of hypokinesis or dyskinesia associated with the myocardial fibrosis (44,86,178). Diastolic dysfunction is the predominant feature of RCM (44,86,178,184).
Doppler evaluation of mitral inflow may show increased E velocity, rapid early deceleration, and little if any filling late in diastole resulting in reduced or absent atrial filling component on the inflow profile (Figures 4.75, 7.49) (48). Early RCM may not show the restrictive pattern of filling but instead shows evidence of impaired relaxation. This mitral inflow pattern shows reduced early filling with a strong atrial component to filling resulting in an E : A ratio less than 1. In the cat, this is a very difficult pattern to record. Heart rates are usually too rapid to differentiate the two phases of left ventricular filling (86,123,181).
Diastolic Dysfunction and RCM
Poor compliance
PW Spectral Doppler
Increased transmitral E wave
Reduced or absent transmitral A wave
Short IVRT
Tissue Doppler
Increased E′ at mitral annulus
Figure 7.49 Restrictive physiology results in high atrial pressures and large E wave velocities with little if any filling secondary to atrial contraction.
Tissue Doppler imaging in cats with restrictive cardiomyopathy shows increased diastolic velocity at the mitral annulus on apical four-chamber views and on the left ventricular wall on right parasternal transverse views at the level of the papillary muscles (48). Acceleration and deceleration rates are increased at both locations. This study showed a subgroup of cats with unclassified cardiomyopathy with tissue Doppler velocities that were no different from tissue velocities in cats with hypertrophic cardiomyopathy (48).