

Biomechanics Principles and Applications - Donald R. Peterson & Joseph D. Bronzino
.pdf

Exercise Physiology |
19-3 |
19.2 Cardiovascular Adjustments
Mechanoreceptors in the muscles, tendons, and joints send information to the CNS that the muscles have begun movement, and this information is used by the CNS to increase heart rate via the sympathetic autonomic nervous system. Cardiac output, the rate of blood pumped by the heart, is the product of heart rate and stroke volume (amount of blood pumped per heart beat). Heart rate increases nearly exponentially at the beginning of exercise with a time constant of about 30 s. Stroke volume does not change immediately but lags a bit until the cardiac output completes the loop back to the heart.
During rest a large volume of blood is stored in the veins, especially in the extremities. When exercise begins, this blood is transferred from the venous side of the heart to the arterial side. Attempting to push extra blood flow through the resistance of the arteries causes a rise in both systolic (during heart ventricular contraction) and diastolic (during the pause between contractions) blood pressures. The increased blood pressures are sensed by baroreceptors located in the aortic arch and carotid sinus (Figure 19.2).
As a consequence, small muscles encircling the entrance to the arterioles (small arteries) are caused to relax by the CNS. Since, by Poiseuille’s Law:
R = |
8L μ |
(19.6) |
π r 4 |
where
R = resistance of a tube, N·sec/m5 L = length of the tube, m
μ = viscosity of the fluid, kg/(m·sec) or N·sec/m2 r = radius of the tube lumen, m
increasing the arteriole radius by 19% will decrease its resistance to one-half. Thus, systolic pressure returns to its resting value, and diastolic pressure may actually fall. Increased blood pressures are called afterload on the heart.
To meet the oxygen demand of the muscles, blood is redistributed from tissues and organs not directly involved with exercise performance. Thus, blood flows to the gastrointestinal tract and kidneys are reduced, whereas blood flows to skeletal muscle, cardiac muscle, and skin are increased.
The heart is actually two pumping systems operated in series. The left heart pumps blood throughout the systemic blood vessels. The right heart pumps blood throughout the pulmonary system. Blood pressures in the systemic vessels are higher than blood pressures in the pulmonary system.
Two chambers comprise each heart. The atrium is like an assist device that produces some suction and collects blood from the veins. Its main purpose is to deliver blood to the ventricle, which is the more
|
|
Muscle |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cerebellum |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Stroke volume |
|
|
|
|
|||
Higher |
|
|
|
|
Medullary |
|
|
|
|
|
|
|
|
|
|
Cardiac |
|
nervous |
|
|
|
vasomotor and |
|
|
Heart |
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
output |
||||||
centers |
|
|
|
cardiac centers |
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
Heart rate |
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Peripheral |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
resistance |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Carotid and aortic |
|
|
|
|
|
|
Blood pressure |
|
|
|
|||
|
|
|
|
|
baroreceptors |
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FIGURE 19.2 General scheme for blood pressure regulation. Dashed lines indicate neural communication, and solid lines indicate direct mechanical effect.

19-4 |
Biomechanics |
powerful chamber that develops blood pressure. The myocardium (heart muscle) of the left ventricle is larger and stronger than the myocardium of the right ventricle. With two hearts and four chambers in series, there could be a problem matching flow rates from each of them. If not properly matched, blood could easily accumulate downstream from the most powerful chamber and upstream from the weakest chamber.
Myocardial tissue exerts a more forceful contraction if it is stretched before contraction begins. This property (known as Starling’s law of the heart) serves to equalize the flows between the two hearts by causing a more powerful ejection from the heart in which more blood accumulates during diastole. The amount of initial stretching of the cardiac muscle is known as preload.
19.3 Maximum Oxygen Uptake
The heart has been considered to be the limiting factor for delivery of oxygen to the tissues. As long as oxygen delivery is sufficient to meet demands of the working muscles, exercise is considered to be aerobic. If oxygen delivery is insufficient, anaerobic metabolism continues to supply muscular energy needs, but lactic acid accumulates in the blood. To remove lactic acid and reform glucose requires the presence of oxygen, which must usually be delayed until exercise ceases or exercise level is reduced.
Fitness of an individual is characterized by a mostly reproducible measurable quantity known as maximal oxygen uptake (VO2max ) that indicates a person’s capacity for aerobic energy transfer and the ability to sustain
high-intensity exercise for longer than 4 or 5 min (Figure 19.3). The more fit, the higher is VO2max . Typical values are 2.5 l/min for young male nonathletes, 5.0 l/min for well-trained male athletes; women have
VO2max values about 70 to 80% as large as males. Maximal oxygen uptake declines with age steadily at 1% per year.
Exercise levels higher than those that result in VO2max can be sustained for various lengths of time. The accumulated difference between the oxygen equivalent of work and VO2max is called the oxygen deficit incurred by an individual (Figure 19.4). There is a maximum oxygen deficit that cannot be exceeded by an individual. Once this maximum deficit has been reached, the person must cease exercise.
The amount of oxygen used to repay the oxygen deficit is called the excess postexercise oxygen consumption (EPOC). EPOC is always larger than the oxygen deficit because (1) elevated body temperature immediately following exercise increases bodily metabolism in general, which requires more than resting levels of oxygen to service, (2) increased blood epinephrine levels increase general bodily metabolism, (3) increased respiratory and cardiac muscle activity requires oxygen, (4) refilling of body oxygen stores requires excess oxygen, and (5) there is some thermal inefficiency in replenishing muscle chemical stores. Considering only lactic acid oxygen debt, the total amount of oxygen required to return the body to its normal resting state is about twice the oxygen debt; the efficiency of anaerobic metabolism is about 50% of aerobic metabolism.
19.4 Respiratory Responses
Respiratory also increases when exercise begins, except that the time constant for respiratory response is about 45 sec instead of 30 sec for cardiac responses (Table 19.1). Control of respiration (Figure 19.5) appears to begin with chemoreceptors located in the aortic arch, in the carotid bodies (in the neck), and in the ventral medula (in the brain). These receptors are sensitive to oxygen, carbon dioxide, and acidity levels but are most sensitive to carbon dioxide and acidity. Thus, the function of the respiratory system appears to be remove excess carbon dioxide and, secondarily, to supply oxygen. Perhaps this is because excess CO2 has narcotic effects, but insufficient oxygen does not produce severe reactions until oxygen levels in the inhaled air fall to one-half of normal. There is no well-established evidence that respiration limits oxygen delivery to the tissues in normal individuals.
Exercise Physiology |
19-5 |
|
|
Phase |
|
|
|
(%) |
|
|
Phase |
|
|
5 |
I |
II |
III |
|
(l/min) |
|
I |
II |
III |
|
|
3 |
7 |
|
|
|
concentration |
|
|
|
|
|
|
10 |
|
|
|
4 |
|
|
18 |
|
|
|
|
/sec)× |
|
|
|
|
|
|
|
|
|
||
5 |
|
|
|
uptake |
|
|
|
|
|
|
|
(m |
|
|
|
|
|
|
|
|
|
||
3 |
|
|
2 |
2 |
16 |
|
|
|
|
||
uptake |
|
|
|
|
2 |
O |
|
|
|
|
|
O |
|
|
|
|
O |
Exhaled |
|
|
|
|
|
2 |
1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
0 |
|
|
14 |
|
|
|
|
10 |
|
|
|
|
|
(%) |
|
|
|
|
|
5 |
|
|
|
|
produced(l/min) |
concentration |
|
|
|
|
|
(m |
3 |
|
|
|
|
|
|
|
|
||
× |
7 |
|
|
4 |
|
|
5 |
|
|
|
|
/sec) |
|
|
|
|
|
|
|
|
|
|
|
3 |
5 |
|
|
|
|
|
|
|
|
|
|
produced |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2 |
2 |
2 |
4 |
|
|
|
|
|
O |
0 |
600 |
1200 |
1800 |
CO |
ExhaledCO |
0 |
600 |
1200 |
|
1800 |
2 |
1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
0 |
|
|
3 |
|
|
|
|
exchangeRespiratoryratio |
|
Time (sec) |
|
|
(beats/sec)rateHeart |
|
Time (sec) |
|
|
||
1.1 |
|
|
|
|
3 |
|
|
|
180 |
||
|
|
|
|
|
|
|
|
|
|||
|
0.9 |
|
|
|
|
|
2 |
|
|
|
120 |
|
0.7 |
|
|
|
|
|
1 |
|
|
|
60 |
5 |
30 |
|
|
|
|
|
|
|
|
|
|
×10 |
0 |
600 |
1200 |
1800 |
ventilationMinute(l/min) |
lacateBlood(moi/m |
0 |
600 |
1200 |
1800 |
|
ventilationMinute(m |
|||||||||||
/sec) |
|
|
|
|
|
3 |
|
|
|
|
|
|
|
|
|
14.0 |
|
) |
10 |
|
|
|
10 |
3 |
20 |
|
|
|
|
|
|
|
|
|
|
|
10 |
|
|
7.0 |
|
|
5 |
|
|
|
5 |
|
|
|
|
|
|
|
|
|
|
|
|
|
0 |
|
|
0 |
|
|
0 |
|
|
|
0 |
|
|
Time (sec) |
|
|
|
|
Time (sec) |
|
|
||
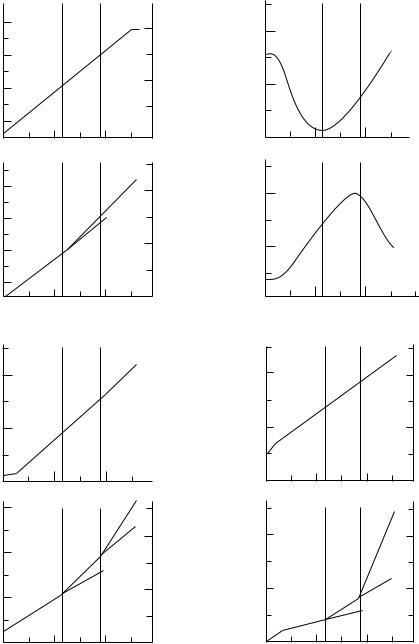
FIGURE 19.3 Concurrent typical changes in blood and respiratory parameters during exercise progressing from rest to maximum. (Adapted and redrawn from Skinner, J.S. and McLellan, T.H. 1980, by permission of the American Alliance for Health, Physical Education, Recreation and Dance.)


Exercise Physiology |
19-7 |
Oxygen is conveyed by convection in the upper airways and by diffusion in the lower airways to the alveoli (lower reaches of the lung where gas exchange with the blood occurs). Oxygen must diffuse from the alveoli, through the extremely thin alveolocapillary membrane into solution in the blood. Oxygen diffuses further into red blood cells where it is bound chemically to hemoglobin molecules. The order of each of these processes is reversed in the working muscles where the concentration gradient of oxygen is in the opposite direction. Complete equilibration of oxygen between alveolar air and pulmonary blood requires about 0.75 sec. Carbon dioxide requires somewhat less, about 0.50 sec. Thus, alveolar air more closely reflects levels of blood carbon dioxide than oxygen.
Both respiration rate and tidal volume (the amount of air moved per breath) increase with exercise, but above the anaerobic threshold the tidal volume no longer increases (remains at about 2 to 2.5 l). From that point, increases in ventilation require greater increases in respiration rate. A similar limitation occurs for stroke volume in the heart (limited to about 120 ml).
The work of respiration, representing only about 1 to 2% of the body’s oxygen consumption at rest, increases to 8 to 10% or more of the body’s oxygen consumption during exercise. Contributing greatly to this is the work to overcome resistance to movement of air, lung tissue, and chest wall tissue. Turbulent airflow in the upper airways (those nearest and including the mouth and nose) contributes a great deal of pressure drop. The lower airways are not as rigid as the upper airways and are influenced by the stretching and contraction of the lung surrounding them. High exhalation pressures external to the airways coupled with low static pressures inside (due to high flow rates inside) tend to close these airways somewhat and limit exhalation airflow rates. Resistance of these airways becomes very high, and the respiratory system appears like a flow source, but only during extreme exhalation.
19.5 Optimization
Energy demands during exercise are so great that optimal courses of action are followed for many physiological responses (Table 19.2). Walking occurs most naturally at a pace that represents the smallest energy expenditure; the transition from walking to running occurs when running expends less energy than walking; ejection of blood from the left ventricle appears to be optimized to minimize energy expenditure; respiratory rate, breathing waveforms, the ratio of inhalation time to exhalation time, airways resistance, tidal volume, and other respiratory parameters all appear to be regulated to minimize energy expenditure [Johnson, 1993].
19.6 Thermal Response
When exercise extends for a long enough time, heat begins to build up in the body. In order for heat accumulation to become important, exercise must be performed at a relatively low rate. Otherwise, performance time would not be long enough for significant amounts of heat to be stored.
Muscular activities are at most 20–25% efficient, and, in general, the smaller the muscle, the less efficient it is. Heat results from the other 75–80% of the energy supplied to the muscle.
Thermal challenges are met in several ways. Blood sent to the limbs and blood returning from the limbs are normally conveyed by arteries and veins in close proximity deep inside the limb. This tends to conserve heat by countercurrent heat exchange between the arteries and veins. Thermal stress causes blood to return via surface veins rather than deep veins. Skin surface temperature increases and heat loss by convection and radiation also increases. In addition, vasodilation of cutaneous blood vessels augments surface heat loss but puts an additional burden on the heart to deliver added blood to the skin as well as the muscles. Heart rate increases as body temperature rises.
Sweating begins. Different areas of the body begin sweating earlier than others, but soon the whole body is involved. If sweat evaporation occurs on the skin surface, then the full cooling power of evaporating sweat (670 W·h/kg) is felt. If the sweat is absorbed by clothing, then the full benefit of sweat evaporation is not realized at the skin. If the sweat falls from the skin, no benefit accrues.

19-8 |
|
|
|
Biomechanics |
|||
|
TABLE 19.2 Summary of Exercise Responses for a Normal Young Male |
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
Light |
Moderate |
Heavy |
Maximal |
|
|
|
Rest |
Exercise |
Exercise |
Exercise |
Exercise |
|
|
|
|
|
|
|
|
|
|
Oxygen uptake (l/min) |
0.30 |
0.60 |
2.2 |
3.0 |
3.2 |
|
|
Maximal oxygen uptake (%) |
10 |
20 |
70 |
95 |
100 |
|
|
Physical work rate (W) |
0 |
10 |
140 |
240 |
430 |
|
|
Aerobic fraction (%) |
100 |
100 |
98 |
85 |
50 |
|
|
Performance time (min) |
α |
480 |
55 |
9.3 |
3.0 |
|
|
Carbon dioxide production (l/min) |
0.18 |
1.5 |
2.3 |
2.8 |
3.7 |
|
|
Respiratory exchange ratio |
0.72 |
0.84 |
0.94 |
1.0 |
1.1 |
|
|
Blood lactic acid (mMol/l) |
1.0 |
1.8 |
4.0 |
7.2 |
9.6 |
|
|
Heart rate (beats/min) |
70 |
130 |
160 |
175 |
200 |
|
|
Stroke volume (l) |
0.075 |
0.100 |
0.105 |
0.110 |
0.110 |
|
|
Cardiac output (l/min) |
5.2 |
13 |
17 |
19 |
22 |
|
|
Minute volume (l/min) |
6 |
22 |
50 |
80 |
120 |
|
|
Tidal volume (l) |
0.4 |
1.6 |
2.3 |
2.4 |
2.4 |
|
|
Respiration rate (breaths/min) |
15 |
26 |
28 |
57 |
60 |
|
|
Peak flow (l/min) |
216 |
340 |
450 |
480 |
480 |
|
|
Muscular efficiency (%) |
0 |
5 |
18 |
20 |
20 |
|
|
Aortic hemoglobin saturation (%) |
98 |
97 |
94 |
93 |
92 |
|
|
Inhalation time (sec) |
1.5 |
1.25 |
1.0 |
0.7 |
0.5 |
|
|
Exhalation time (sec) |
3.0 |
2.0 |
1.1 |
0.75 |
0.5 |
|
|
Respiratory work rate (W) |
0.305 |
0.705 |
5.45 |
12.32 |
20.03 |
|
|
Cardiac work rate (W) |
1.89 |
4.67 |
9.61 |
11.81 |
14.30 |
|
|
Systolic pressure (mmHg) |
120 |
134 |
140 |
162 |
172 |
|
|
Diastolic pressure (mmHg) |
80 |
85 |
90 |
95 |
100 |
|
|
End-inspiratory lung volume (l) |
2.8 |
3.2 |
4.6 |
4.6 |
4.6 |
|
|
End-expiratory lung volume (l) |
2.4 |
2.2 |
2.1 |
2.1 |
2.1 |
|
|
Gas partial pressures (mmHg) |
|
|
|
|
|
|
|
Arterial pCO2 |
40 |
41 |
45 |
48 |
50 |
|
|
pO2 |
100 |
98 |
94 |
93 |
92 |
|
|
Venous pCO2 |
44 |
57 |
64 |
70 |
72 |
|
|
pO2 |
36 |
23 |
17 |
10 |
9 |
|
|
Alveolar pCO2 |
32 |
40 |
28 |
20 |
10 |
|
|
pO2 |
98 |
94 |
110 |
115 |
120 |
|
|
Skin conductance [watts/(m2·◦ C)] |
5.3 |
7.9 |
12 |
13 |
13 |
|
|
Sweat rate (kg/sec) |
0.001 |
0.002 |
0.008 |
0.007 |
0.002 |
|
|
Walking/running speed (m/sec) |
0 |
1.0 |
2.2 |
6.7 |
7.1 |
|
|
Ventilation/perfusion of the lung |
0.52 |
0.50 |
0.54 |
0.82 |
1.1 |
|
|
Respiratory evaporative water loss (l/min) |
1.02 × 10–5 |
4.41 × 10–5 |
9.01 × 10–4 |
1.35 × 10–3 |
2.14 × 10–3 |
|
|
Total body convective heat loss (W) |
24 |
131 |
142 |
149 |
151 |
|
|
Mean skin temperature (◦ C) |
34 |
32 |
30.5 |
29 |
28 |
|
|
Heat production (W) |
105 |
190 |
640 |
960 |
1720 |
|
|
Equilibrium rectal temperature (◦ C) |
36.7 |
38.5 |
39.3 |
39.7 |
500 |
|
|
Final rectal temperature (◦ C) |
37.1 |
38.26 |
39.3 |
37.4 |
37 |
|
Sweating for a long time causes loss of plasma volume (plasma shift), resulting in some hemoconcentration (2% or more). This increased concentration increases blood viscosity, and cardiac work becomes greater.
19.7 Applications
Knowledge of exercise physiology imparts to the medical or biological engineer the ability to design devices to be used with or by humans or animals, or to borrow ideas from human physiology to apply to other situations. There is need for engineers to design the many pieces of equipment used by sports and health enthusiasts, to modify prostheses or devices for the handicapped to allow for performance of greater than
Exercise Physiology |
19-9 |
light levels of work and exercise, to alleviate physiological stresses caused by personal protective equipment and other occupational ergonometric gear, to design human-powered machines that are compatible with the capabilities of the operators, and to invent systems to establish and maintain locally benign surroundings in otherwise harsh environments. Recipients of these efforts include athletes, the handicapped, laborers, firefighters, space explorers, military personnel, farmers, power-plant workers, and many others. The study of exercise physiology, especially in the language used by medical and biological engineers, can result in benefits to almost all of us.
Defining Terms
Anaerobic threshold: The transition between exercise levels that can be sustained through nearly complete aerobic metabolism and those that rely on at least partially anaerobic metabolism. Above the anaerobic threshold, blood lactate increases and the relationship between ventilation and oxygen uptake becomes nonlinear.
Excess postexercise oxygen consumption (EPOC): The difference between resting oxygen consumption and the accumulated rate of oxygen consumption following exercise termination.
Maximum oxygen consumption: The maximum rate of oxygen use during exercise. The amount of maximum oxygen consumption is determined by age, sex, and physical condition.
Oxygen deficit: The accumulated difference between actual oxygen consumption at the beginning of exercise and the rate of oxygen consumption that would exist if oxygen consumption rose immediately to its steady-state level corresponding to exercise level.
References
Johnson, A.T. 1993. How much work is expended for respiration? Front. Med. Biol. Eng. 5: 265.
Mole,´ P.A. 1983. Exercise metabolism. In A.A. Bove and D.T. Lowenthal (Eds.), Exercise Medicine, pp. 43–88. New York, Academic Press.
Skinner, J.S. and McLellan, T.H. 1980. The transition from aerobic to anaerobic metabolism. Res. Q. Exerc. Sport 51: 234.
White, A., Handler, P., Smith, E.L. et al. 1959. Principles of Biochemistry. New York, McGraw-Hill.
Further Information
A comprehensive treatment of quantitative predictions in exercise physiology is presented in Biomechanics and Exercise Physiology by Arthur T. Johnson (John Wiley & Sons, 1991). There are a number of errors in the book, but an errata sheet is available from the author.
P.O. Astrand and K. Rodahl’s Textbook of Work Physiology (McGraw-Hill, 1970) contains a great deal of exercise physiology and is probably considered to be the standard textbook on the subject.
Biological Foundations of Biomedical Engineering, edited by J. Kline (Little Brown, Boston), is a very good textbook of physiology written for engineers.