

Полезные материалы за все 6 курсов / Учебники, методички, pdf / INBDEBooster Head and Neck Anatomy Notes
.pdfHead and Neck Anatomy
4 The Auricular Group
Auricular muscles
These muscles are associated with the ear. There are three in total, the auricularis anterior, posterior, and superior.
•Origin:
Auricularis anterior: lateral border of epicranial aponeurosis
Auricularis posterior: mastoid process of temporal bone
Auricularis superior: epicranial aponeurosis
•Insertion:
Auricularis anterior: major helix of ear
Auricularis posterior: posterior auricle
Auricularis superior: superior auricle
•Action:
Auricularis anterior: pulls auricle anteriorly
Auricularis posterior: pulls auricle posteriorly
Auricularis superior: pulls auricle superiorly
51
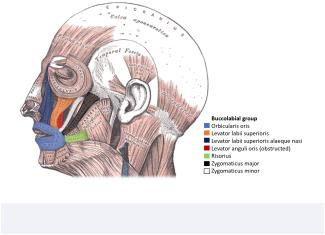
5 The Buccolabial Group
Overview
This group is the most extensive of all other facial muscle groups. Primarily, these muscles control movements of the lips and mouth region. For studying purposes, it may help to bring this section into two groups: one group for superior muscles of the mouth, and one group for inferior muscles of the mouth. 11 muscles will be discussed for this section:
Orbicularis oris
This muscle Is easily identifiable by its circular border around the mouth and lips. It has a marginal and peripheral portion.
•Origin:
Both parts: modiolus of mouth (fibromuscular junction)
•Insertion:
Marginal part: from modiolus of one side to the other
Peripheral part: skin of lips
•Action:
Both parts:
-Bilateral contraction closes mouth/lips
-Contraction of individual regions leads to various movements like pouting and puckering
-Important role in shaping the mouth for speech
Figure 9.03 The auricular muscle group
INBDE Booster | Booster PrepTM
Head and Neck Anatomy
The modiolus of the mouth has contributions from various muscles of facial expressions, which insert into the angle of the mouth at many different angles/orientations. These 9 muscles include the
•Zygomaticus major,
•Orbicularis oris,
•Buccinator,
•Levator anguli oris
•Mentalis
•Depressor labii inferior-is
•Depressor anguli oris
•Risorius
•Platysma
Levator labii superioris
This muscle is triangular in shape and is associated with the upper lip.
•Origin: zygomatic process of maxilla and maxillary process of zygomatic bone
•Insertion: skin of upper lip/orbicularis oris
•Action: elevation and eversion of upper lip
Levator labii superioris alaeque nasi
This is found bilaterally to the nose. It has three parts, the nasolabial, alar, and lip.
•Origin: frontal process of maxilla
•Insertion: perichondrium plus skin of major alar cartilage of the nose
•Action: elevation and eversion of upper (middle) lip, elevation of nasolabial furrow and lateral nasal ala
Levator anguli oris
This muscle is fairly straightforward in terms of its location and function.
•Origin: canine fossa of maxilla
•Insertion: angle of mouth (modiolus)
•Action: elevates angles of mouth, assisting in smiling
52
Risorius
The risorius is an interesting muscle because it is not found in all people.
•Origin: fascia of lateral cheek (parotid gland region), superficial masseter, and platysma
•Insertion: skin of angle of mouth (modiolus)
•Action: moves angles of mouth laterally and superiorly (smiling)
Zygomaticus major
This muscle is very well-known for its role in producing a smile when activated.
•Origin: lateral zygomatic bone
•Insertion: angle of mouth (modiolus)
•Action: elevates and everts angles of mouth, assisting in smiling
Zygomaticus minor
This muscle is similar to the zygomaticus major in terms of function.
•Origin: lateral zygomatic bone
•Insertion: skin of upper lip, lateral to levator labii superioris alaeque
•Action: elevates and everts angles of mouth, assisting in smiling
Figure 9.04 The buccolabial muscle group
INBDE Booster | Booster PrepTM

Head and Neck Anatomy
Depressor labii inferioris
This muscle is opposite to that of its superior counterpart.
•Origin: oblique line of mandible
•Insertion: skin of lower lip
•Action: depression of lip
Depressor anguli oris
This muscle is also opposite to that of its superior counterpart.
•Origin: oblique line and mental tubercle of mandible
•Insertion: modiolus
•Action: depresses angle of the mouth, assisting in frowning
Mentalis
This bilateral muscle is found mirrored across the midline of the face and forms the shape of a "v" from a frontal view.
•Origin: incisive fossa of mandible
•Insertion: skin of chin
•Action: elevates and wrinkles chin, lower lip "pouts"
Buccinator
The buccinator is located deep to the masseter and has three parts, superior/maxillary, inferior/ mandibular, and posterior/longitudinal.
•Origin:
Superior: alveolar process of maxilla
Inferior: buccinator ridge of mandible
Posterior: anterior margin of the pterygomandibular raphe
•Insertion: angle of mouth (modiolus)
•Action: facilitates chewing and swallowing by compressing cheeks inward against molars, activated when playing wind instruments (ex. the trumpet) or whistling
53
Figure 9.05 Other muscles with the buccolabial group
INBDE Pro Tip:
Differentiating less-obvious anatomical names:
•Mentalis: means "chin," but another way to remember this is that when many people think, they put their hands on their chin
•Risorius: means "laughing" or "ridiculous," which would involve this muscle when one laughs or smiles
•Procerus: means "tall" or "extended", so think of someone with a long nose like Pinocchio, which is associated with the location of this muscle
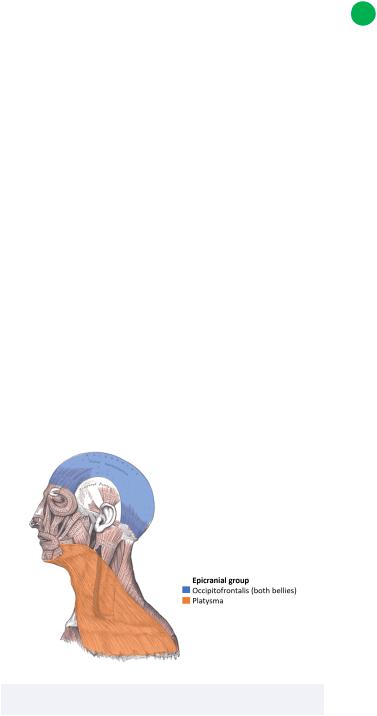
6 The Epicranial Group
Occipitofrontalis
This muscle is quite large, as it spans much of the medial skull from the occipital to the frontal region. As evident from its name, it has a frontal and occipital part.
•Origin:
Frontal part: skin of eyebrows
Occipital part: lateral two-thirds of superior nuchal line of occipital bone
•Insertion:
Frontal part: epicranial aponeurosis at coronal suture
Occipital part: epicranial aponeurosis at lambdoid suture
INBDE Booster | Booster PrepTM
Head and Neck Anatomy
•Action:
Frontal part: elevates brows, forms horizontal wrinkles on forehead
Occipital part: retracts scalp
Platysma
The platysma is a thin muscle often referred to as the "shaving muscle" because its activation tenses the skin of the neck to facilitate shaving.
•Origin: skin/fascia of superior thoracic and shoulder regions (clavicle, acromial region, pectoralis major and deltoid muscles)
•Insertion:
Medial fibers: lower border of the mandible and the skin of the lower lip
Lateral fibers: skin of the perioral region, modiolus
•Action: lateral fiber contraction causes corners of mouth and lip to lower while medial fiber contraction may depress mandible and open the mouth
Figure 9.06 The muscles of the epicranial group
54
7 Clinical Considerations
The above information should be studied with clinical relevance in mind whenever possible. For example, many muscles have individual functions, yet can also work together to perform facial expressions. However, some conditions make it difficult or impossible to perform certain expressions.
Muscles used to frown
The following muscles are used to frown:
•Orbicularis oculi (2 muscles)
•Corrugator supercilii (2 muscles)
•Procerus (1 muscle)
•Orbicularis oris (1 muscle)
•Depressor anguli oris (2 muscles)
•Depressor labii inferioris (2 muscles)
•Mentalis (1 muscle)
•Platysma (2 muscles)
Muscles used to smile
The following muscles are used to smile:
•Orbicularis oculi (2 muscles)
•Levator labii superioris (2 muscles)
•Levator anguli oris (2 muscles)
•Zygomaticus major (2 muscles)
•Zygomaticus minor (2 muscles)
•Risorius (2 muscles)
Muscles of facial expression disorders
There are various disorders that may be evident from observing a patient's inability to engage their facial muscles.
•Facial nerve paralysis results in a patient having difficulty speaking, eating, or showing facial expressions
May be caused by a stroke, Bell's palsy, infection, or tumors
Central facial lesion
-Paralysis of lower half of one side of the face; symmetrical lift of forehead observed
INBDE Booster | Booster PrepTM

Head and Neck Anatomy |
55 |
Peripheral facial lesion
-Paralysis of the ipsilateral eyelid and forehead of one side of face; asymmetrical lift of forehead observed
Figure 9.07 Summary of the muscles of facial expressions
INBDE Booster | Booster PrepTM
Head and Neck Anatomy |
56 |
Muscles of the Eye
The muscles of the eye is a smaller section of the INBDE, though it is relevant to a dentist's holistic knowledge of head anatomy. Candidates should be able to distinguish between the different muscles, paying particular attention to their innervation and function. These notes will provide some useful tips to help you remember information for this section of your board exam.
1 Muscles of the Eye Overview
The muscles of the eye include two major groups. There are 7 extrinsic or extraocular muscles of the eye. The majority of these muscles are important for major movements of the eye or supporting structures such as the eyelids. The intrinsic or intraocular muscles of the eye are important for changing the amount of light that enters the eye, which is essential for sight.
There are a handful of major movements of the eye you should be familiar with:
•Abduction: eye moves outward (laterally)
•Adduction: eye moves inward (medially)
•Intorsion: internal or medial rotation; ie. the top of the eye rotates towards the nose
•Extorsion: external or lateral rotation; ie. the top of the eye rotates away from the nose
•Elevation: eye moves upward (superiorly)
•Depression: eye moves downward (inferiorly)
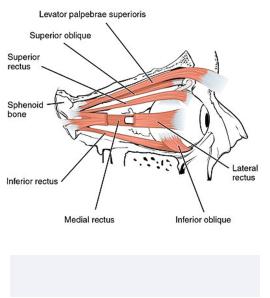
2 Extraocular Eye Muscles
Overview
These 7 muscles function to move the eye around within its socket (the orbit) to provide a greater sense of the environment to assist one's vision. These muscles are innervated by three main cranial nerves: the oculomotor nerve (CN III), the trochlear nerve (CN IV), and the abducens nerve (CN VI). The majority of these muscles are innervated by CN III, with only one muscle being innervated by CN IV and CN VI.
INBDE Pro Tip:
There is an incredibly useful tip to help you remember which cranial nerves innervate each muscle. Recall your knowledge of chemical formulae.
Here, we will represent the lateral rectus muscle and superior oblique muscle as LR and SO, respectively. All the other muscles will be represented with O. We will use subscript numbers to indicate the cranial nerves that innervate these muscles. Thus, we are left with
LR6SO4O3.
INBDE Booster | Booster PrepTM
Head and Neck Anatomy
Lateral rectus
•Origin: common tendinous ring of orbital apex
•Insertion: near limbus of eye (lateral aspect)
•Action: abduction of eye
•Innervation: Abducens nerve (CN VI)
Superior oblique
•Origin: sphenoid bone at orbital apex
•Insertion: sclera of superolateral aspect of eye
•Action: intorsion, abduction and depression of eye
•Innervation: Trochlear nerve (CN IV)
Medial rectus
•Origin: common tendinous ring of orbital apex
•Insertion: near limbus of eye (medial aspect)
•Action: adduction of eye
•Innervation: Oculomotor nerve (CN III)
Inferior oblique
•Origin: orbital surface of maxilla
•Insertion: inferolateral aspect of eye
•Action: abduction, elevation and extorsion of eye
•Innervation: Oculomotor nerve (CN III)
Superior rectus
•Origin: common tendinous ring of orbital apex
•Insertion: near limbus of eye (superior aspect)
•Action: adduction, elevation and intorsion of eye
•Innervation: Oculomotor nerve (CN III)
57
Inferior rectus
•Origin: common tendinous ring of orbital apex
•Insertion: near limbus of eye (inferior
•aspect)
•Action: depression, adduction, and extorsion of eye
•Innervation: Oculomotor nerve (CN III)
Levator palpebrae superioris
•Origin: lesser wing of sphenoid bone (inferior aspect), posterosuperior aspect of orbit
•Insertion: superior tarsal plate and skin of upper eyelid
•Action: elevation and retraction of upper eyelid
•Innervation: Oculomotor nerve (CN III)
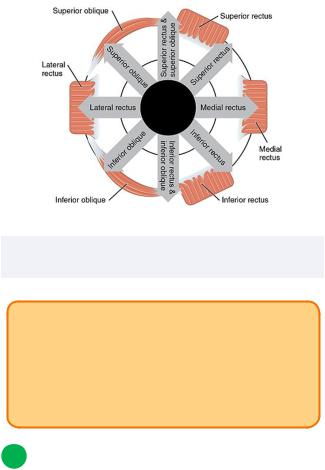
Figure 10.01 The extraocular muscles of the right eye
INBDE Booster | Booster PrepTM
Head and Neck Anatomy
Figure 10.02 The extraocular muscles of the right eye and their actions
INBDE Pro Tip:
Although there is a dedicated muscle for the upper eyelid, the levator palpebrae superioris, there is no individual muscle for the lower eyelid. The lower eyelid is formed by three lamellae, which includes the orbicularis oculi muscle.
3 Intraocular Eye Muscles
Overview
These 3 muscles function to change the amount of light entering the eye, which directly affects one's vision. These muscles are innervated by one of two different cranial nerves, either the oculomotor nerve CN III or the ophthalmic branch of the trigeminal nerve CN V1.
The origin and insertion of these muscles are a bit complex for the scope of the INBDE, so the general anatomy, function, and innervation are more relevant for you to know.
58
Ciliary muscle
•Anatomy: smooth muscle that surrounds and attaches to the lens in a circular fashion via the zonular fibers to change the lens shape
•Function: involved in near-sight accommodation; contraction produces spherical lens shape for near sight whereas relaxation does the opposite
Does NOT impact pupil size
•Innervation: Oculomotor nerve (CN III); parasympathetic nervous system fibers via short ciliary nerves
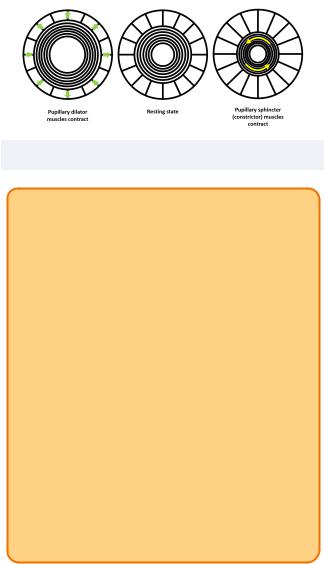
Sphincter pupillae
•Anatomy: six to eight rings of smooth muscle that encircles the pupil
•Function: does impact pupil size
Causes miosis, which is pupil constriction (minimizes light Intake during bright light)
•Innervation: Oculomotor nerve (CN III); parasympathetic nervous system fibers via short ciliary nerves
PSNS makes sense because we would require less light or sight during rest and digest
Dilator pupillae
•Anatomy: smooth muscle that runs in a radial fashion ie. the bands "point" towards the pupil
•Function: does impact pupil size
Causes mydriasis, which is pupil dilation (increases light intake during dim lighting)
•Innervation: Trigeminal nerve (CN V1); sympathetic nervous system fibers via long ciliary nerves
SNS makes sense because we would require more light or sight during fight or flight
INBDE Booster | Booster PrepTM
Head and Neck Anatomy |
59 |
Figure 10.03 The intraocular muscle movements
INBDE Pro Tip:
To remember which intraocular muscles are innervated by which nerves, group the ciliary muscle together with the sphincter pupillae muscle. These two muscles shorten other structures of the eye (the lens or pupil), whereas the dilator pupillae opens it up (the pupil).
Knowing this, the ciliary muscle and sphincter pupillae muscle can be grouped with the O3 of the extraocular mnemonic you know. Just remember that these intraocular muscles have PSNS innervation.
For the dilator pupillae, remember the mnemonic "dye five" since it is innervated by CN V1. You'll know it's the ophthalmic branch because it's the only branch that makes sense for the eye region!
INBDE Booster | Booster PrepTM
Head and Neck Anatomy |
60 |
Muscles of the Ear
The muscles of the of the ear is a minor topic to know for the INBDE, though it is still good to know this information if it ever comes up on your board exam. Candidates should be able to differentiate between the various groups of muscles within and external to the ear, in addition to their function. These notes provide everything you need to know for this section so you're feeling confident about the anatomy of the ear.
1 Muscles of the Ear Overview
The muscles of the ear have various functions depending on their location. The muscles of the middle ear play a protective role within the ear to prevent damage from occurring during loud sounds. The intrinsic muscles of the ear function to alter the overall shape of the ear, though have a minimal role in hearing. In contrast, the extrinsic muscles are responsible for changing the position of the outer ear.
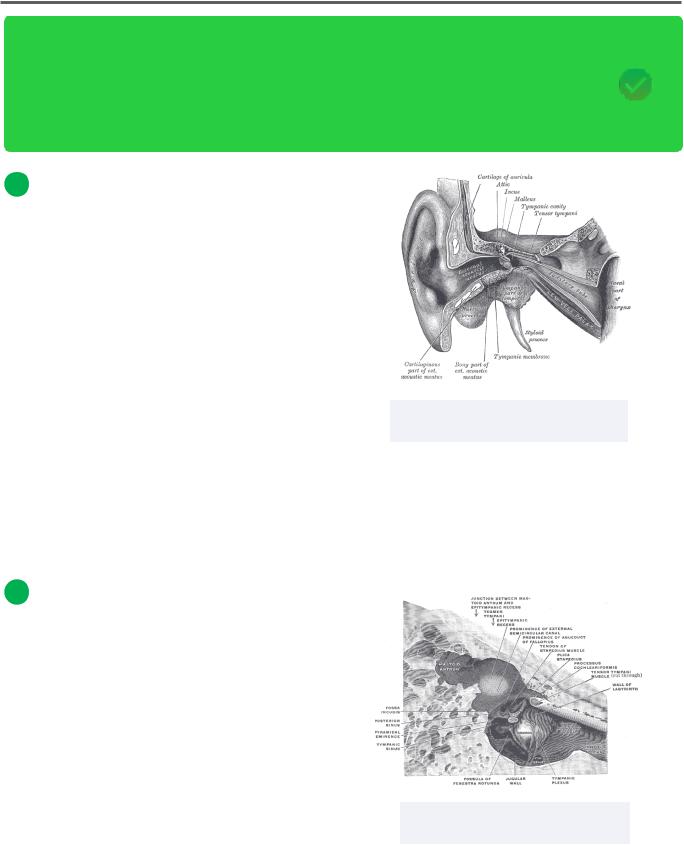
Figure 11.01 The tensor tympani within the middle ear
The intrinsic and extrinsic muscles are both innervated by the facial neve (CN VII). There are two muscles of the middle ear; the stapedius is also innervated by the facial nerve (CN VII), but the tensor tympani muscle is innervated by the trigeminal nerve (CN V3).
2 Muscles of the Middle Ear
Tensor tympani
•Origin: eustachian tube, greater wing of sphenoid
•Insertion: superior region of malleus
•Action: tenses tympanic membrane; protects against hearing impairment by softening loud sounds
Stapedius
•Origin: temporal bone (pyramidal eminence)
•Insertion: neck of stapes
•Action: prevents extreme oscillation of stapes when exposed to loud sounds
Figure 11.02 The stapedius within the middle ear
INBDE Booster | Booster PrepTM