

Полезные материалы за все 6 курсов / Учебники, методички, pdf / INBDEBooster Head and Neck Anatomy Notes
.pdfHead and Neck Anatomy
Note: Recall that CN V2 is the maxillary branch of the trigeminal nerve.
Figure 4.03 The pterygopalatine fossa
Figure 4.04 The pterygopalatine fossa’s borders
2 Internal Fossae
Cranial fossae
There are general main fossae that can be used to describe the skull base in thirds. They are as follows:
•Anterior fossa: Contains the frontal lobes of the brain and is comprised of the frontal, ethmoid and lesser wing of sphenoid bones
•Middle fossa: Contains the pituitary gland and the temporal lobes of the brain and is formed by the greater wing of sphenoid and temporal lobes
•Posterior fossa: Contains the brainstem and cerebellum and is mainly formed by the occipital bone, and partly by the temporal bones
21
Figure 4.05 The three cranial fossae
INBDE Booster | Booster PrepTM
Head and Neck Anatomy |
22 |
Fascial Space Infections
The fascial spaces are an important topic for your board exam. Candidates must first understand these potential spaces, their borders, and contents so that this information can be applied within a clinical context. These notes include diagrams, tips and tricks that will highlight everything you need to know for this topic so that you are well-prepared and confident for these types of clinical problems.
1 Introduction to fascia
The fascia is a thin collection of fibrous tissues that surrounds and encases the body's organs, vasculature, bones, nerves, and muscles. It plays a small role in protection and support of these structures. During an anatomical dissection, it has a similar appearance to that of thick spider's webs or the pith of an orange. There are three types:
•Superficial fascia – classified as loose connective tissue and is found beneath the dermis
•Deep fascia – surrounds bones, nerves, muscles, and vasculature
•Visceral fascia – surrounds internal organs
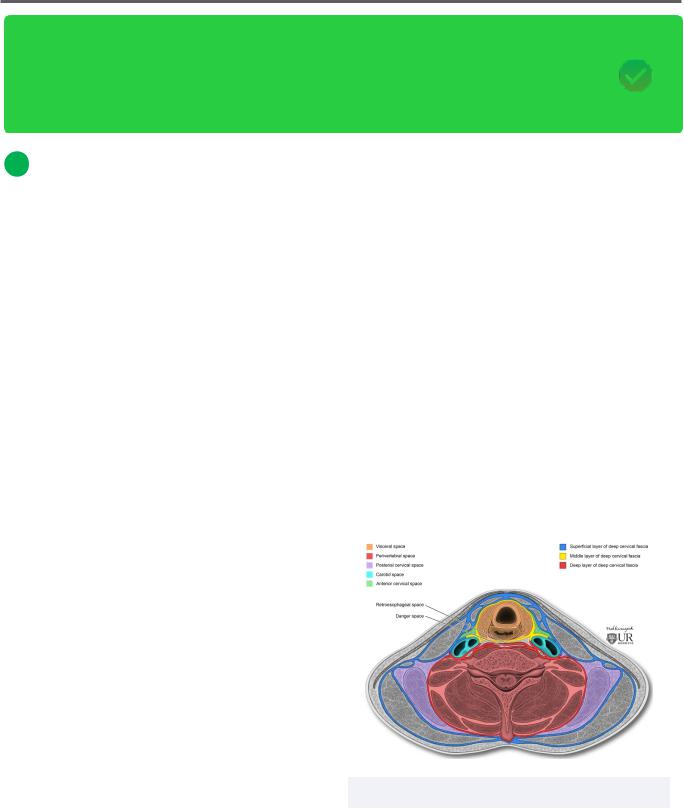
Cervical fascia
There are two types of cervical fascia in the neck:
•Superficial cervical fascia – is a thin layer of connective tissue found between the dermis and the deep cervical fascia
Contains the platysma muscle, cutaneous nerves and vessels, lymph nodes, and fat
•Deep cervical fascia – is found deep to the superficial cervical fascia and is comprised of four main layers:
Investing layer: is the most superficial deep fascial layer and encases the trapezius plus sternocleidomastoid muscles
Pretracheal layer: found in the anterior part of the neck
-Muscular part: houses the infrahyoid muscles
-Visceral part: encases the trachea, esophagus, and thyroid gland
Has contributions from the buccopharyngeal fascia
Prevertebral layer: is found encasing the vertebral column, the prevertebral muscles, scalene muscles, and deep muscles of the neck
-Also surrounds the brachial plexus and subclavian artery
Carotid sheath: contains the common and internal carotid arteries, CN X, internal jugular vein, sympathetic nerve fibres, and lymph nodes
Figure 5.01 Regions of the cervical fascia
INBDE Booster | Booster PrepTM

Head and Neck Anatomy
2Fascial Spaces and Infection Introduction
Fascial spaces
Fascial spaces are regions of the head and neck that are possible regions for infection, that would not otherwise be present in a healthy person. These spaces become larger as a result of infection from surrounding tissues and areas.
Fascial spaces overview
There are two main types of fascial spaces:
•Primary spaces: regions that can be directly infected as a result of periapical or periodontal infection and include the following spaces:
Perimandibular spaces:
-Submandibular
-Submental
-Sublingual
Buccal
Canine
Vestibular
•Secondary spaces: regions that can be infected from another fascial region (either primary or secondary) and include the following spaces:
Masticator space:
-Superficial and deep temporalInfratemporal space
-Submasseteric
-Pterygomandibular
Deep spaces of the neck:
-ParapharyngealLateral pharyngealRetropharyngeal
-Prevertebral
-Danger
Periorbital
23
Cardinal signs of infection
There are five cardinal signs of inflammation/ infection in an individual. They include:
•Rubor/redness as a result of increased blood flow
•Calor/heat resulting from increased blood flow, fluid accumulation, and inflammatory signals
•Tumor/swelling due to fluid accumulation
•Dolor/pain from the stretch receptors in nearby tissues being activated, inflammatory signals and cellular meditors
•Functio laesa/loss of function from pain, tissue structure impairment, as well as
fibroplasia and metaplasia
Within the context of dentistry, may be dyspnea (difficulty breathing), dysphagia (difficulty swallowing), trismus (lock-jaw) etc.
Vital signs of infection
On your board exam and in clinical practice, vital signs are important pieces of information when assessing a patient or conducting a diagnosis. The main vitals signs to look out for include:
•Elevated temperature >100 °F
•Elevated heart rate/pulse >100 bpm
•Elevated blood pressure >120/80
•Elevated breathing/respiratory rate >16 rpm
•Abnormal size of lymph nodes/ lymphadenopathy
INBDE Pro Tip:
As a general rule, infections will follow the path of least resistance. This means that areas with a lower volume of bone or muscle, including reduced bone density and muscular attachments, will facilitate the spread of infection.
This is an important rule to remember, as it can be applied across the various fascial spaces to help determine the likely path of infection.
INBDE Booster | Booster PrepTM
Head and Neck Anatomy |
24 |
3 Differentiating the Fascial Spaces |
|
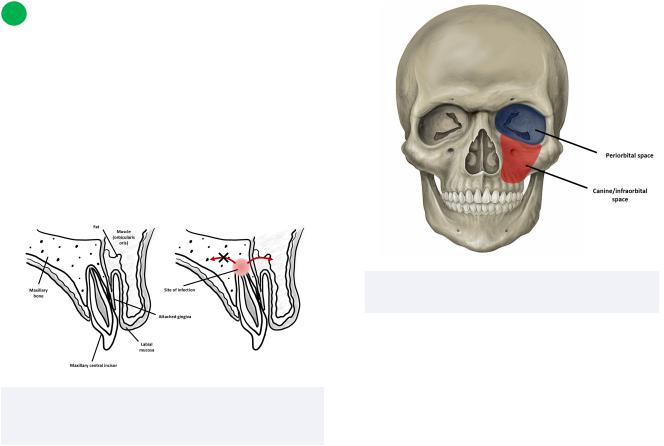
Vestibular space
The vestibular space can be found between the mucoperiosteum of a tooth and the cortical bone. It is an important fascial space because it is the most common region for dental infections to spread from the alveolar bone.
Figure 5.02 Sagittal view of normal tooth anatomy (left) and vestibular space infection forming via the path of least resistance (right)
The canine/infraorbital space
This potential space is found within the canine fossa, between the levator anguli oris and the levator labii superioris muscles.
•Infection may arise in this region via spread from affected maxillary canine teeth.
•Infections may present in the region through swelling of the upper lip, anterior cheek, vestibule, nasolabial folds, and in more serious cases, the lower eyelid.
The periorbital space
This region is located between the orbital septum and oribcularis oris. Due to its close proximity to the eye, an infection here can lead to edema of the eyelid and may also impair vision.
•Since this region is a secondary space, it may become infected as a result of a primary infection in the canine space
Figure 5.03 The periorbital and canine/ infraorbital spaces
The buccal space
The buccal space is found subcutaneously between the buccinator muscle and the skin of the face. It contains many important structures, such as the buccal fat pad, Stensen's duct, the facial artery, and branches of CN VII and IX.
•Infection of this region is evidenced by prominent swelling of the lip(s) and cheek
•May be caused by infected premolars or molars
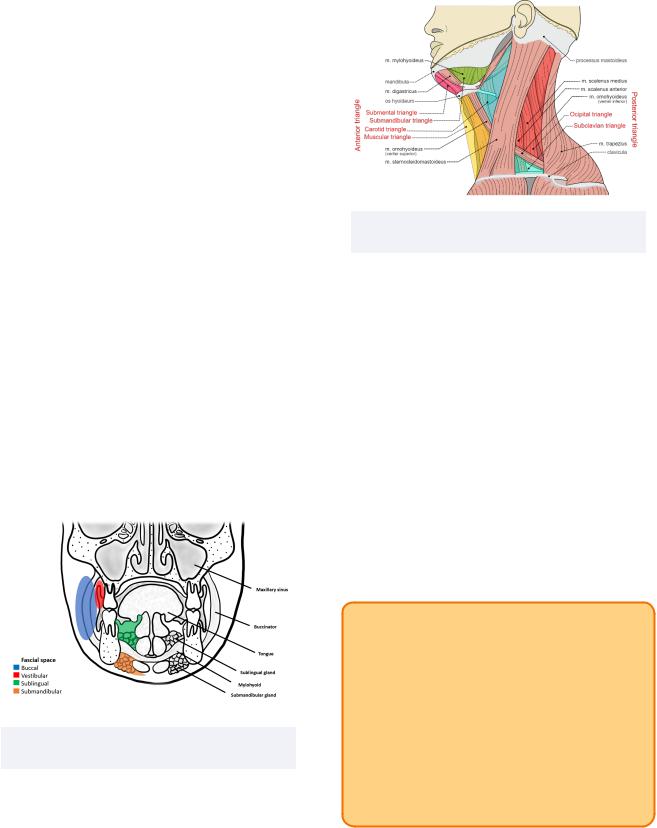
The sublingual space
This space is found laterally located to the muscles of the tongue as well as the lingual region of the body of the mandible.
•Infection may be caused by an infected sublingual gland or via periapical infection from the mandibular teeth whose roots are located superior to the mylohyoid muscle attachment
•The lingual and hypoglossal nerves are contained in this space, and may be affected
•Edema may be present, which may elevate and protrude the tongue; speech may also be affected
INBDE Booster | Booster PrepTM
Head and Neck Anatomy
The submandibular space
This space is located on the inferior aspect of the mandible, specifically between two muscles: the anterior and posterior bellies of digastric muscles.
•An infection may be derived from organs or structures within this region, such as the periapical regions of molar teeth found inferior to the mylohyoid muscle attachment
•Swelling localized to the submandibular region
The submental space
Any of the anterior mandibular teeth that become infected may form this space, located beneath the midline of the chin at the submental triangle.
•More specifically, it is bordered superiorly by the mylohyoid muscle attachment, and inferiorly by the superficial layer of the deep cervical fascia and platysma
•Infection may be evident from swelling of the chin, and potentially difficulty swallowing
Figure 5.04 A coronal section of the skull displaying various fascial spaces
25
Figure 5.05 Various triangles of the neck, namely the submental triangle
Clinical importance of perimandibular spaces
Recall that the three perimandibular spaces include the submandibular, submental, and sublingual spaces. Knowledge of these regions is important in the case of Ludwig's angina, which is an infection and subsequent swelling of these three regions. It can be described as follows:
•The infection spreads from the sublingual region in a posteroinferior direction
Floor of mouth is raised
May spread to the epiglottis and vocal cords
-May result in drooling, difficulty speaking, and difficulty breathing which could be life-threatening
INBDE Pro Tip:
One way to remember the contents of the perimandibular space is that "Perry uses his mandible to eat subs." In this way, you can remember that the perimandibular spaces include the submandibular, submental, and sublingual spaces.
Note that it does NOT include the submasseteric space, as this belongs within the masticator space.
INBDE Booster | Booster PrepTM
Head and Neck Anatomy
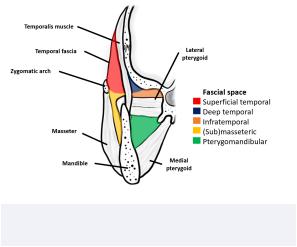
The superficial and deep temporal spaces The superficial temporal space is found between the temporal fascia and the temporalis muscle, and may be formed via infected upper third molars.
•This region contains the temporal fat pad
•Clinically, infection presents as a large "lump" near the zygomatic arch
The deep temporal space, as evident from its name, is deeper than the superficial temporal space because it is located between the temporalis muscle and the skull.
•Its source of infection is the same as the superficial region as well, though swelling may present slightly below the zygomatic arch near the infratemporal region and lateral eye
The infratemporal space
This space is often associated with the deep temporal space, and may also be called the infra-temporal portion of the deep temporal space. As such, it may be considered a component of the deep temporal space itself.
•It can be found lateral to the lateral pterygoid plate of the sphenoid bone, inferior to the base of the skull, and superior to the lateral pterygoid muscle.
•Contains maxillary artery branches and pterygoid venous plexus
•Infections in this region are unlikely, though when present, are serious due to significant vasculature
The submasseteric/masseteric space
The submasseteric or otherwise known as the masseteric space is found between the mandible and the masseter muscle. This space may be infected due to lower third molars that are buccally placed.
26
•Infection in this space may cause swelling at the angle of the mandible, in addition to trismus (difficulty opening the mouth) being an important clinical sign
The pterygomandibular space
This space is located lateral to the medial pterygoid muscle, and medial and superior to the mandible, and inferior to the lateral pterygoid.
•This potential space is very important clinically, as there are many key structures that reside within it and is relevant for procedures such as an inferior alveolar nerve block
•Contains the inferior alveolar nerve and artery, lingual nerve, sphenomandibular ligament, and the interpterygoid fascia
•This space may be infected due to lower third molars that are buccally placed or a contaminated needle during an inferior alveolar nerve block
•May present clinically as trismus, dysphagia, and swelling of the anterior retromolar area
Figure 5.06 Fascial spaces associated with muscles of mastication
INBDE Booster | Booster PrepTM

Head and Neck Anatomy
Clinical importance of the masticator space
Recall that the four components of this space include the submasseteric, pterygomandibular, temporal, and infratemporal spaces.
•Contains major structures, such as the muscles of mastication (see section on this for more information), ramus and body of
the mandible, CN V3, inferior alveolar nerve, artery and vein, as well as the pterygoid venous plexus
INBDE Pro Tip:
One way to remember the contents of the masticator space is its name! Each of the spaces allude to each of the muscles of mastication:
•Submasseteric: the masseter
•Pterygomandibular: the pterygoids
•Temporal/infratemporal: the temporalis
The parapharyngeal space
The parapharyngeal space forms a ring around the pharynx and is a clinically important region.
•Contains the lateral pharyngeal and retropharyngeal spaces
•May be a key pathway for the spread of infection from the facial region to the neck and mediastinum due to its association with the lateral and retropharyngeal spaces
The lateral pharyngeal space
This region is found lateral to the pharynx and forms an inverted pyramid at the base of the skull with its apex at the hyoid bone.
•Infection may be caused by the lower third molars, pterygomandibular or submandibular spaces, in addition to the tonsils
•Contains lymph nodes, carotid sheath, key vasculature such as the ascending pharyngeal and facial arteries, and key nerves such as CN IX, CN XI, CN XII
•May present clinically as difficulty opening mouth, dysphagia, or difficulty rotating the neck contralaterally
27
The retropharyngeal space
This space is found anterior to the alar fascia and posterior to the buccopharyngeal fascia. It is a clinically important area because its superior border is the base of the skull and its inferior border is the superior mediastinum.
•Infection in this region is thus very dangerous, since there is a high risk of infection spread
•Additionally, the risk of infection spread is increased because the danger space/area is deep to this region
The danger space/area
This space owes its name to the fact that infection in this region provides an easy outlet for further infection in the thorax.
•It is located deep to the retropharyngeal space, and superficial to the pretracheal space
•It is bordered anteriorly by the alar fascia and posteriorly by the prevertebral layer of the deep cervical fascia
•It is clinically important because its inferior border is the mediastinum, making infection spread quickly and easily from the pharynx to the mediastinum and its contents
The prevertebral space
The prevertebral space is bordered anteriorly by the danger space and posteriorly by the fascia of the vertebral column (specifically that attached to the spinous process and the ligamentum nuchae). Superiorly it is bound by the base of the skull and inferiorly it is bound by the superior mediastinum and as far as the coccyx.
•Contents include longus colli and longus capitis muscles, scalene muscles, vertebral artery and vein, phrenic nerve, and the brachial plexus in part
INBDE Booster | Booster PrepTM
Head and Neck Anatomy
The deep spaces of the neck summary
The retropharyngeal, danger, and prevertebral spaces are thought to be somewhat continuous with one another, and many sources tend to group these regions together. There is some overlap with the borders of these regions, particularly the inferior border and its relation to the mediastinum. Review Figure 1. for a diagram containing these deep spaces of the neck.
•Clinically, an infection can spread from these regions to the mediastinum (mediastinitis), though in rare circumstances an upper respiratory tract infection can be spread to these regions
•Infection in these spaces (depending on their specific localization) may cause a stiff neck, sore throat, dysphagia or dyspnea
INBDE Pro Tip:
Parallel parking can be a bit tricky! After all the head turning to check bind-spots and mirror for danger, you may hurt your neck!
The deep spaces of the neck can be remembered using the mnemonic "PaRalleL, Danger, Pain" which stands for the Parapharyngeal, Retropharyngeal, Lateral pharyngeal, Danger, and Prevertebral spaces.
The parotid space
The parotid space is considered a deep neck space. It forms a triangular shape that essentially outlines a cavity filled by the parotid gland. Other contents include the external carotid artery, retro-mandibular vein and intraparotid facial nerve.
•Infection to this area is usually not caused by primary infection nor odontogenic
•May be caused by parotitis (inflammaiton of parotid gland) or sialolithiasis (salivary gland stones)
•Presents as a medial bulge located on the lateral pharyngeal wall
28
4 Treatment
Various treatment options exist for fascial space infections. They may vary depending on the complexity of the case, specific region affected, or cause. A few potential treatments could include:
•Incision and drainage to reduce bacterial
load, alter local environment (introduce O2), reduce pressure from fluid accumulation, and increase blood flow to flush out remaining bacteria/mediators
•Extraction or pulpectomy for odontogenic causes
•Antibiotics to control spread of infection, reduce swelling, and for systemic infections
INBDE Booster | Booster PrepTM

Head and Neck Anatomy |
29 |
The Cranial Nerves
The cranial nerves section is arguably one of the most important topics that INBDE candidates need to be well-acquainted with. This is because the cranial nerves are responsible for innervating many key structures of the head and neck region, in addition to some other structures in the descending thorax and abdominal region. These notes will discuss the 12 cranial nerves in detail, with an emphasis on which cranial nerves are of more importance in the field of dentistry and the board exam. In these notes, tips, tricks, and helpful summaries will provide essential tools that will simplify information and assist in retention during studying.
1 Nervous system structure
Overview
The nervous system can be divided into two main categories, the central nervous system (CNS) and peripheral nervous system (PNS).
The CNS is comprised of the brain and the spinal cord. The brain can be further subdivided into:
•Forebrain (Cerebrum)
Cognition, hunger and thirst
•Midbrain
Auditory and visual responses
•Hindbrain (Pons, cerebellum, medulla)
Balance, respiration, cough reflex
The spinal cord relays voluntary movements, conducts sensory information to the brain and motor information away from the brain, includes the spinal reflex arc, and some autonomic functions.
The PNS is an extension of the brain and spinal cord in body. Its sensory component can be broken into:
•Somatic
General: pain, heat, touch, pressure, body position
Special: vision, hearing, balance
•Visceral:
General: pain or reflex sensations
Special: smell and taste
Its motor component can be broken into:
•Somatic:
Voluntary motor control of muscles
•Visceral or autonomic nervous system (ANS):
Actions under involuntary control like heartbeat, pupil constriction etc.
Sympathetic nervous system (SNS): fight or flight
Parasympathetic nervous system (PSNS): rest and digest
INBDE Booster | Booster PrepTM
Head and Neck Anatomy
Sympathetic fibers tend to have short preganglionic fibers and long postganglionic fibers. This is because the sympathetic nervous system has more widespread effects in the body, synapsing in the sympathetic ganglionic chain near the vertebral column. In contrast, the parasympathetic system has long preganglionic fibers, and short postganglionic fibers, where they synapse closer to their effector organs. This is because they tend to have more localized effects.
INBDE Pro Tip:
The sympathetic system is ready to fight or flight, so it’s excited to synapse right away. The parasympathetic system is resting and digesting (a little lazy), so it will take its time until it’s closer to its effector organ to synapse
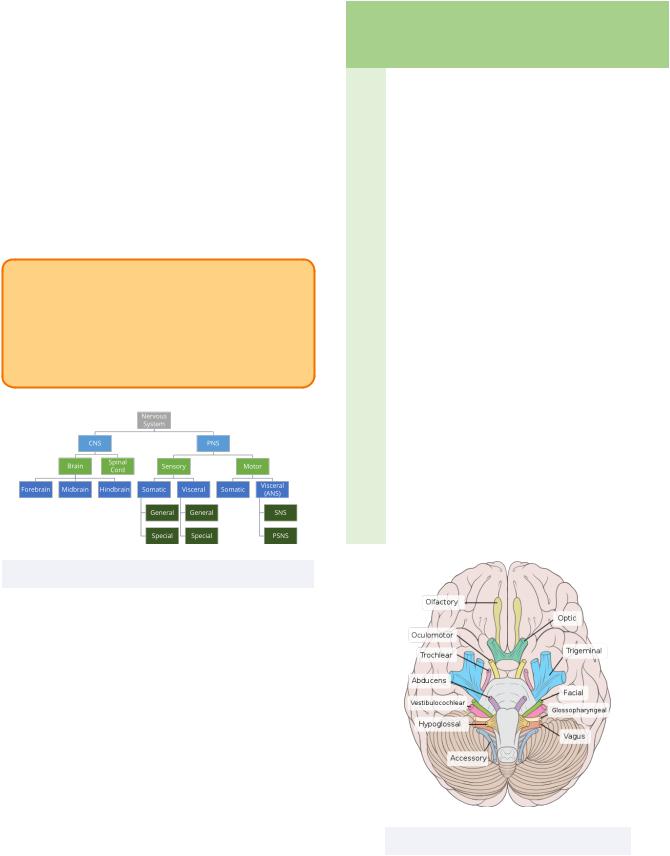
Figure 6.01 Organization of the nervous system
The parasympathetic system is more relevant to some of the cranial nerves than the sympathetic system is. There are 12 cranial nerves in total, ordered using roman numerals and each with their own respective names. Below is a table with the cranial nerves, with a color code used to group many of the cranial nerves together based on function.
|
|
|
|
30 |
|
|
|
|
|
# |
Name |
Name |
Function |
Function |
|
|
Mnem- |
|
Mnem- |
|
|
onic |
|
onic |
|
|
|
|
|
I |
Olfactory |
Oh |
Sensory |
Some |
|
|
|
|
|
II |
Optic |
Oh |
Sensory |
Say |
|
|
|
|
|
III |
Oculo- |
Oh |
Motor |
Marry |
|
motor |
|
|
|
|
|
|
|
|
IV |
Trochlear |
To |
Motor |
Money |
|
|
|
|
|
V |
Trigeminal |
Touch |
Both |
But |
|
|
|
|
|
VI |
Abducens |
And |
Motor |
My |
|
|
|
|
|
VII |
Facial |
Feel |
Both |
Brother |
|
|
|
|
|
VIII |
Vestibulo- |
Very |
Sensory |
Says |
|
cochlear |
|
|
|
|
|
|
|
|
IX |
Glosso- |
Green |
Both |
Big |
|
pharyngeal |
|
|
|
|
|
|
|
|
X |
Vagus |
Vege- |
Both |
Brains |
|
|
tables |
|
|
|
|
|
|
|
XI |
(Spinal) |
A |
Motor |
Matter |
|
Accessory |
|
|
|
|
|
|
|
|
XII |
Hypo- |
H |
Motor |
More |
|
glossal |
|
|
|
|
|
|
|
|
Figure 6.02 The 12 cranial nerves
INBDE Booster | Booster PrepTM