370 |
15 Left Lateral Sectionectomy |
|
|
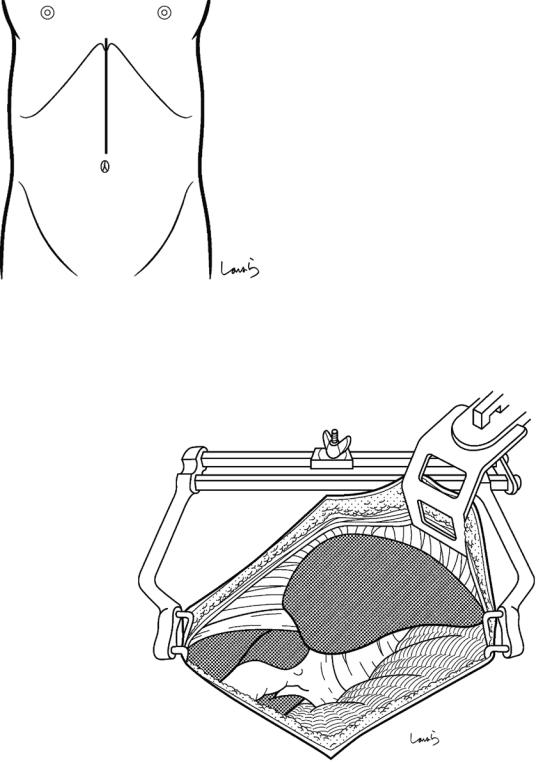
Fig. 15.1 The surgeon stands on the right side of the patient and makes an upper abdominal midline incision extending from the xiphoid process to the umbilicus to open the abdomen to the left of the round ligament of the liver
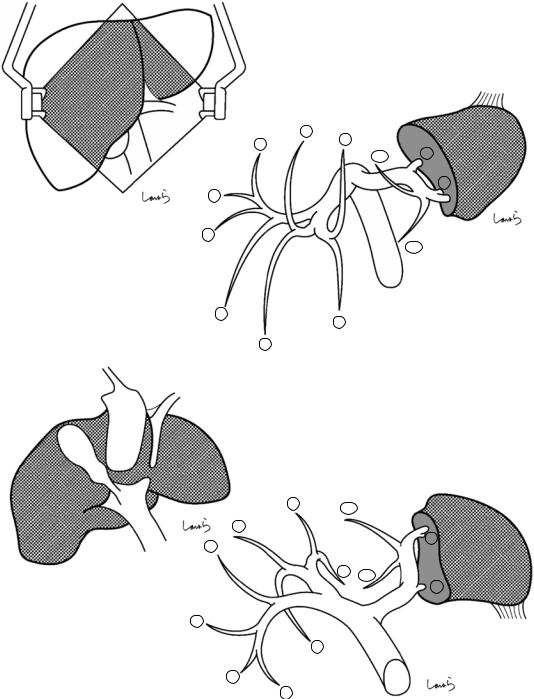
Fig. 15.2 A wound retractor and a left rib retractor are applied to secure the operative field. A surgical laparotomy sponge is placed over the stomach, spleen, and transverse colon
15 Left Lateral Sectionectomy |
371 |
|
|
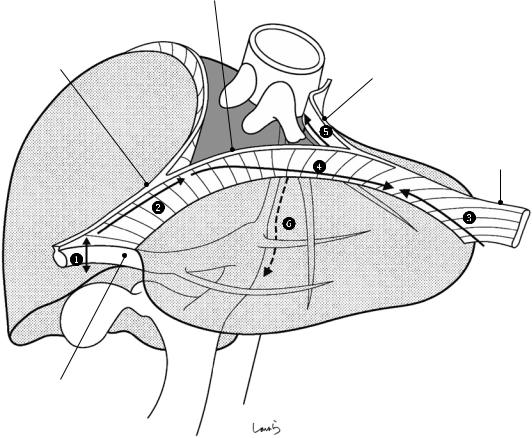
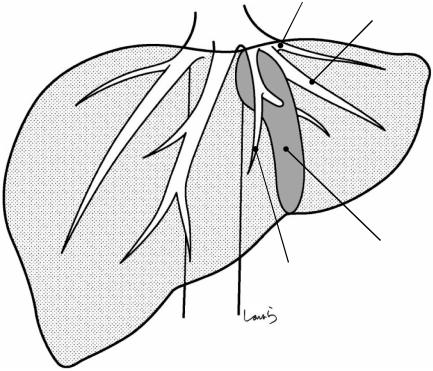
Ant. layer of L coronary lig.
|
IVC |
Falciform lig. |
Post. layer of L coronary lig. |
|
L triangular lig.
Ligamentum teres
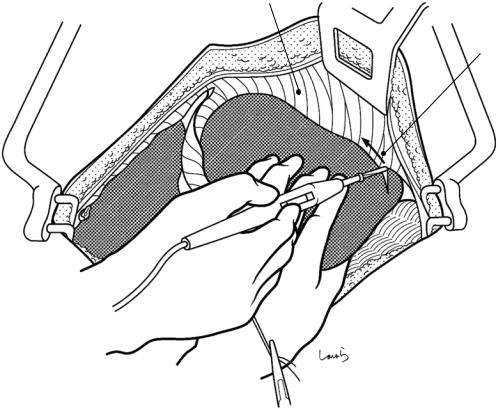
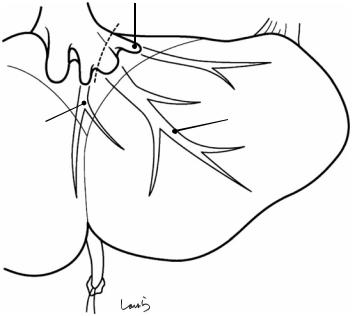
Fig. 15.3 The procedure begins with mobilization of the lateral segment and is performed in the following order: dividing the round ligament, dividing the falciform ligament, dividing the left triangular liga-
ment, dividing the anterior layer of the left coronary ligament, dividing the posterior layer of the left coronary ligament, and dividing the attachment of the lesser omentum to the liver
372 |
15 Left Lateral Sectionectomy |
|
|
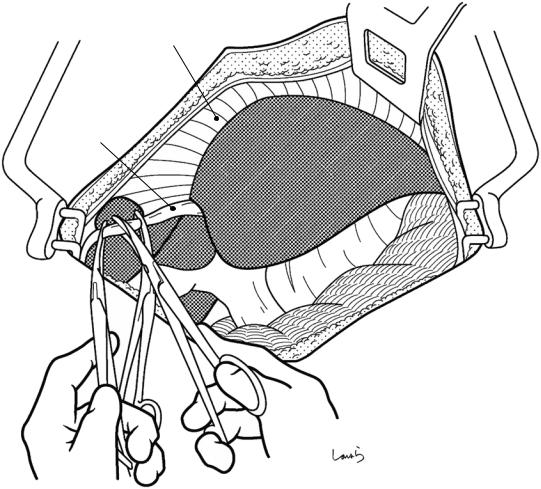
Falciform lig.
Ligamentum teres
Fig. 15.4 The round ligament is ligated and divided at a point closer to the abdominal wall side. The suture thread on the liver side is kept long enough to allow for later traction and is grasped with Pean forceps
376 15 Left Lateral Sectionectomy
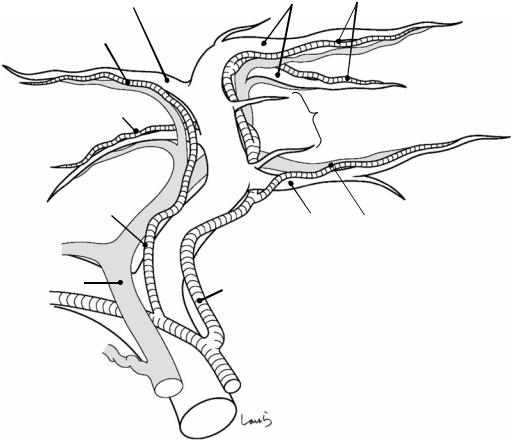
Mid. hepatic v. |
L hepatic v. |
|
|
|
R coronary lig. |
|
|
|
|
|
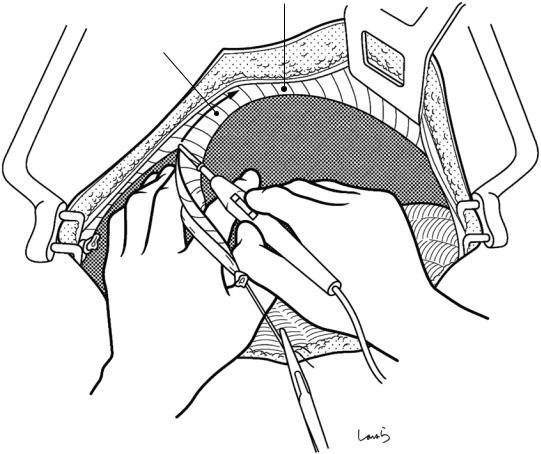
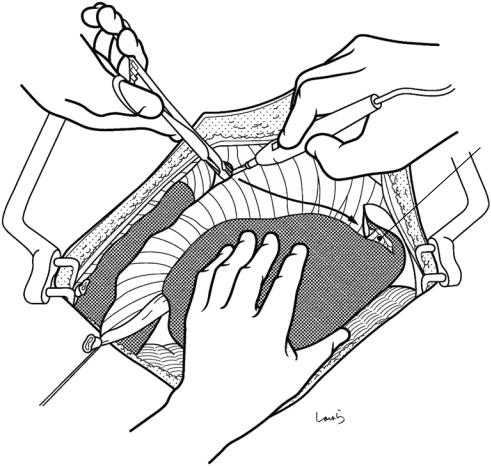
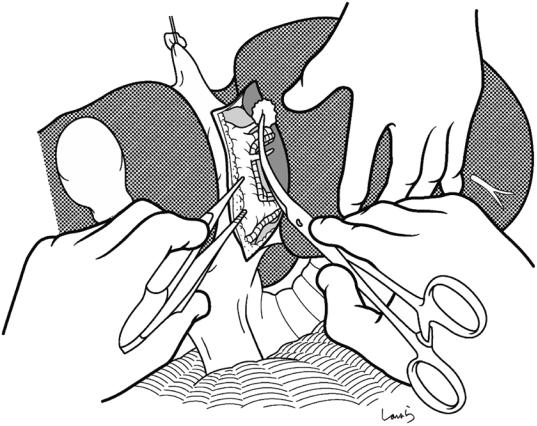
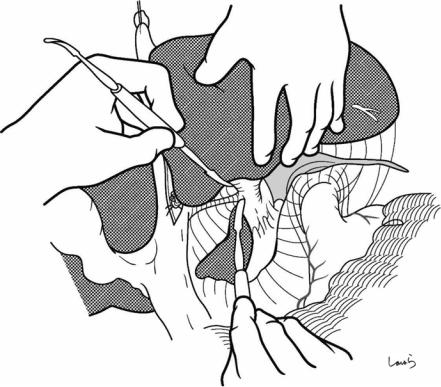
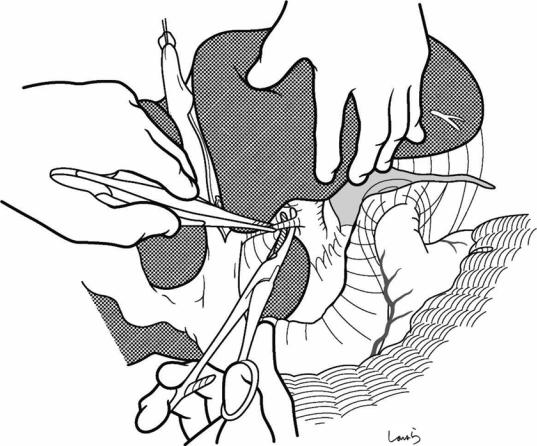
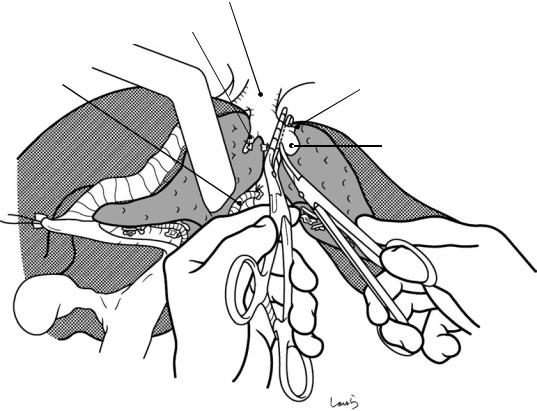
Fig. 15.8 The connective tissue surrounding the left and middle hepatic veins are roughly dissected with Metzenbaum scissors. These two veins often form a com-
mon trunk at their root. Cutting the right coronary ligament slightly may make it easier to identify the hepatic veins
380 |
15 Left Lateral Sectionectomy |
|
|
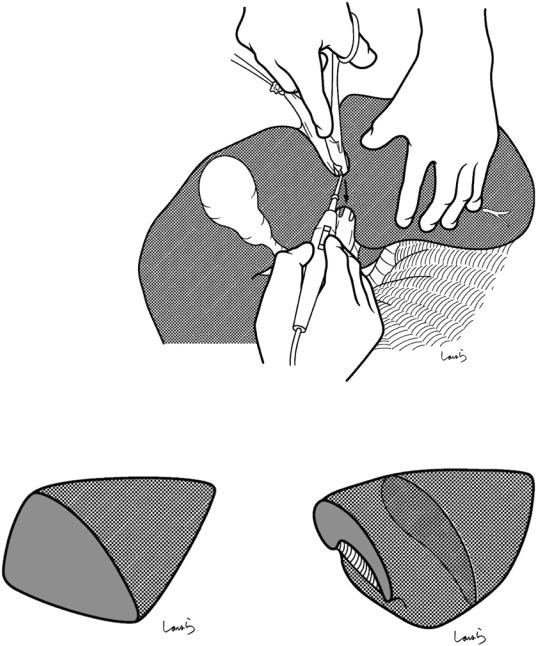
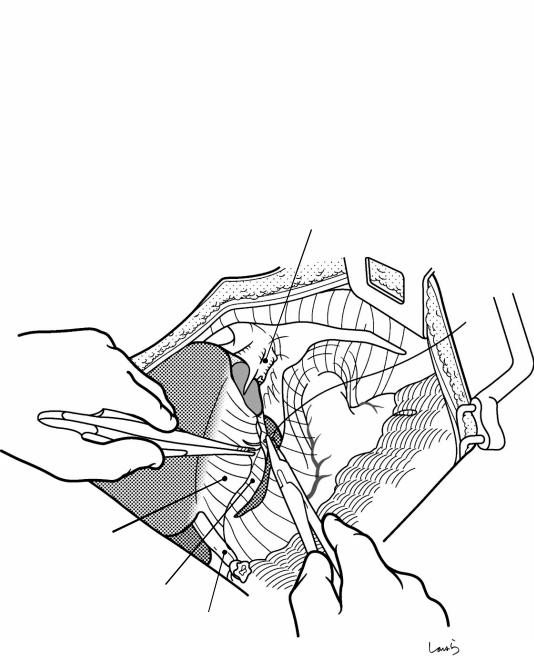
Fig. 15.12 We move on now to dissection of the Glissonean vessels. The suture thread applied to the round ligament is pulled cranially but slightly to the right to cause the lateral segment to stand upright. If the liver parenchyma forms a bridge overlying the umbilical portal vein, scoop the bridge with dissection forceps at once and divide with electrocautery
a |
b |
Wrong shape |
Correct shape |
Fig. 15.13 The lateral segment of the liver is generally thought to have a pyramidal shape (a), but it is actually flat- shaped (b), with its longitudinal cross section not triangular-shaped but rather spindleor comma-shaped
382 |
15 Left Lateral Sectionectomy |
|
|
Ligamentum teres
Cut edge of lesser omentum
Lobule of Spiegel within caudate lobe
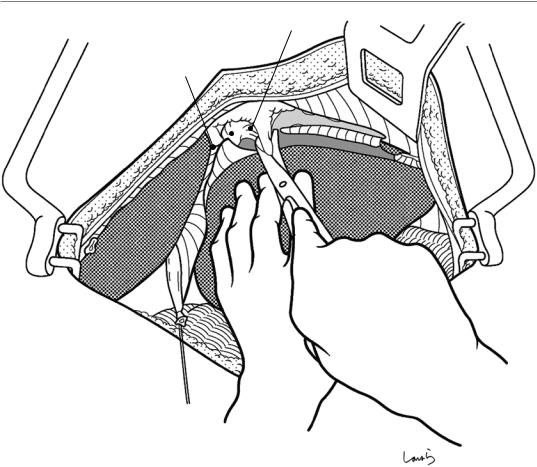
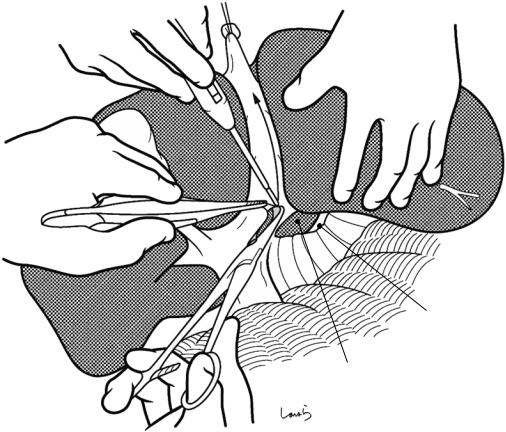
Fig. 15.15 In front of the umbilical portal vein, right- angled dissection forceps are inserted upward from the preformed cut edge of the lesser omentum to scoop just
the peritoneum (arrow) and divide it with electrocautery. The dissection line should ascend along the left margin of the round ligament
386 |
15 Left Lateral Sectionectomy |
|
|
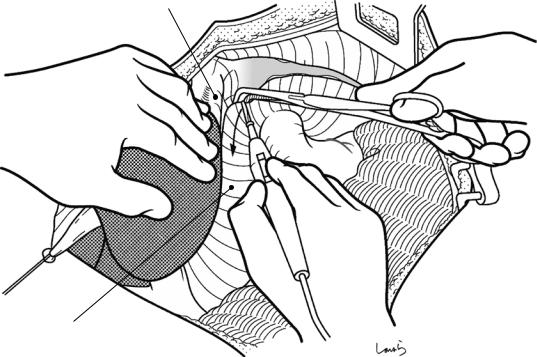
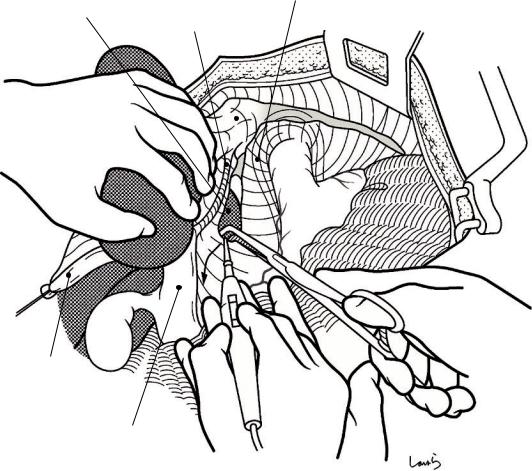
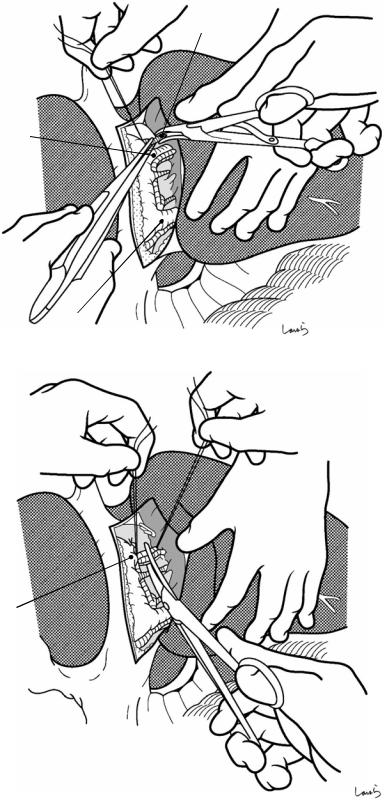
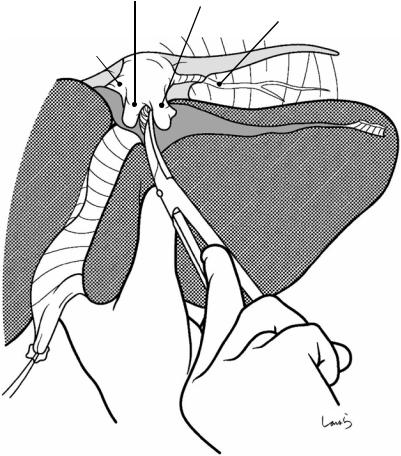
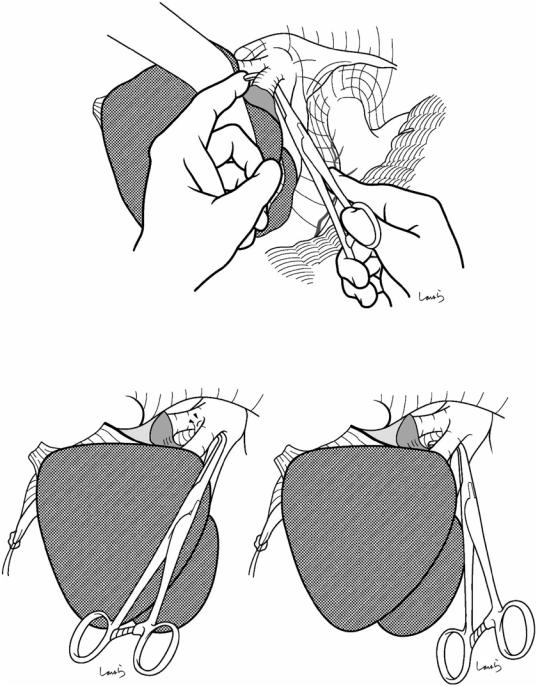
Fig. 15.20 The bile duct has a fibrous pattern/structure and cannot be identified easily. The connective tissue is peeled off laterally with a gauze ball to expose the bifurcation of the B3 and B2 (a). Then, dissection forceps are inserted along the liver parenchyma to scoop up each duct close to the bifurcation and then ligate/divide them (b). The ducts can be ligated en bloc before the bifurcation if the resulting ligated bundle is not too thick
|
a |
P3 +A3 |
|
(ligated on proximal side) |
|
|
B3
B2
b
B3
P2 + A2
(ligated on resection side)
388 |
15 Left Lateral Sectionectomy |
|
|
L hepatic v.
Fig. 15.22 Dissection of the left hepatic vein: With the lateral segment everted to the right, the connective tissue around the lateroposterior aspect of the left hepatic vein is roughly excised with dissectors
394 |
15 Left Lateral Sectionectomy |
|
|
L sup. hepatic v.
L hepatic v.
 Br. from S3
Br. from S3
Dissection plane of liver
Umbilical fissure v.
Fig. 15.28 At this point, the lateral segment is discolored dark red, bordered by the falciform ligament. Parenchymal dissection is performed along the imaginary dissection line set 1 cm to the left of the ligament. The procedure is the same as that for right lobectomy. A relatively thick
branch extending from S3 and draining into the umbilical fissure vein may be encountered around the upper border and should be ligated and divided. The dissection area is small, so the dissection can be completed very quickly
396 |
15 Left Lateral Sectionectomy |
|
|
Sutured stump of L hepatic v.
Falciform lig.
Cut edge of lesser omentum
Ligamentum teres
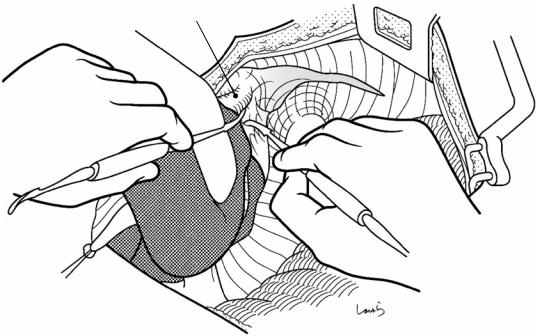
Fig. 15.30 After achieving hemostasis of the dissection plane, the falciform ligament is placed over the plane as a “lid.” If the ligament is broad enough, the entire plane can
be covered with the ligament. Suturing the ligament to the cut edge of the lesser omentum will result in a beautiful lid that you know will be secure
15 Left Lateral Sectionectomy |
397 |
|
|
Sutured stump of L hepatic v.
Dissection plane of liver covered by falciform lig.
Contour of caudate lobe
Fig. 15.31 After washing the abdominal cavity, an 8-mm duple drain is inserted via the right abdominal wall through the foramen of Winslow to the vicinity of the dis-
section plane of the liver. The operation is then completed by closing the abdominal wall, suturing in three layers