


 Int. anal sphincter
Int. anal sphincter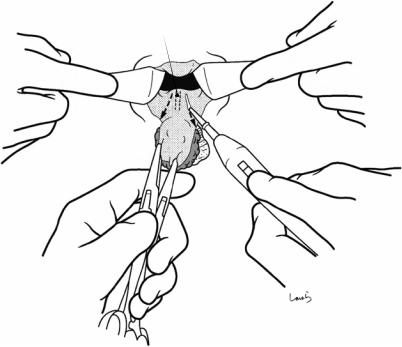
 Int. anal sphincter
Int. anal sphincter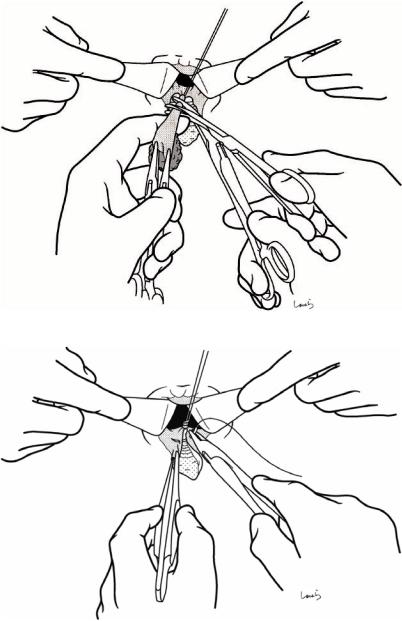
324 |
13 Hemorrhoidectomy |
|
|
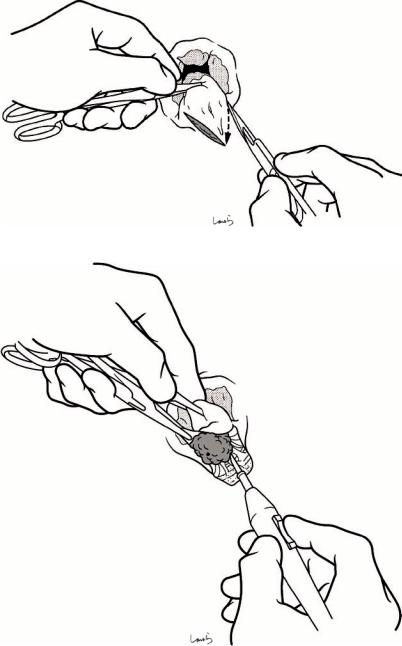
Fig. 13.8 After applying a clamp distal to the ligation and resecting the hemorrhoid, another 3-0 Vicryl suture is applied to make a double ligation. One of the two suture threads is left uncut so that we can use it as a stay suture for the next mucosal suture
Fig. 13.9 The mucosal defect formed by resection can either be left untreated as an open wound or suture-closed to achieve hemostasis at the mucosal stump and promote clean wound healing. A running 3-0 Vicryl suture is placed. The first ligation suture and stay suture are further tied to invaginate the stump
13 Hemorrhoidectomy |
325 |
|
|
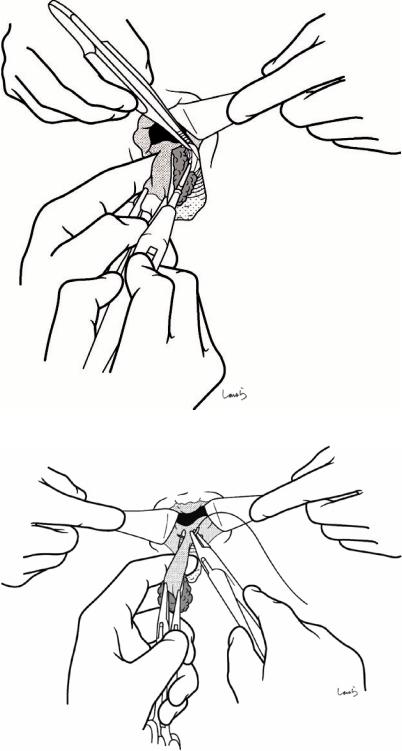
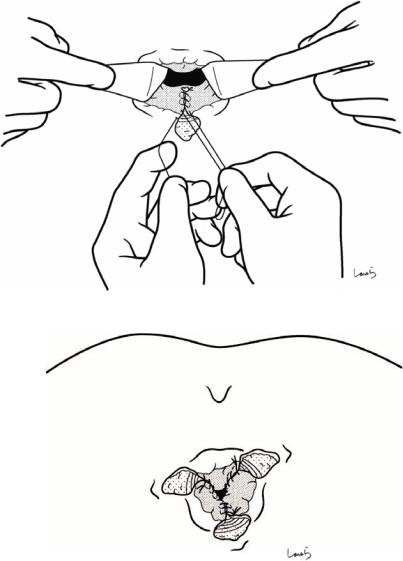
Fig. 13.10 The mucosal suture should not exceed the dentate line. To prevent the formation of dead space, we should leave the skin incision unsutured as an open wound for drainage
Fig. 13.11 The procedure described above is performed for all hemorrhoids, typically 3. The operation is completed after confirming the absence of bleeding and the completeness of the mucosal sutures