Tubular abnormalitis
Etiology : kidney congenital diseases, pyelonephritis, interstitial nephritis, autoimmune diseases, tumors.
•Polyuria
•Nocturia
•< of urine density
•Nephrogenic osteopathy
•Electrolytes disorders
•Glucosuria
•Acidosis
•Normal GFR



Incidence of AKI*
•500 ppm/year – UK ( up to 38,000/yr)
•Incidence of AKI needing dialysis 200 ppm/year
•Pre renal and acute tubular necrosis (ATN) accounts for 75% of the cases of AKI
•7% of all hospital admissions( 65% of intensive care admission)
•Mortality:
•5-10% in uncomplicated AKI
•50-70% in AKI secondary to other organ failure( intensive care)
•> 50% in dialysis requiring AKI
*Xue JL, Daniels F, Star RA et al. Incidence and mortality of acute renal failure in Medicare beneficiaries, 1992 to 2001. J Am Soc Nephrol 2006; 17: 1135–1142.

Staging of AKI
The cause of AKI should be determined whenever possible

Conceptual model for AKI
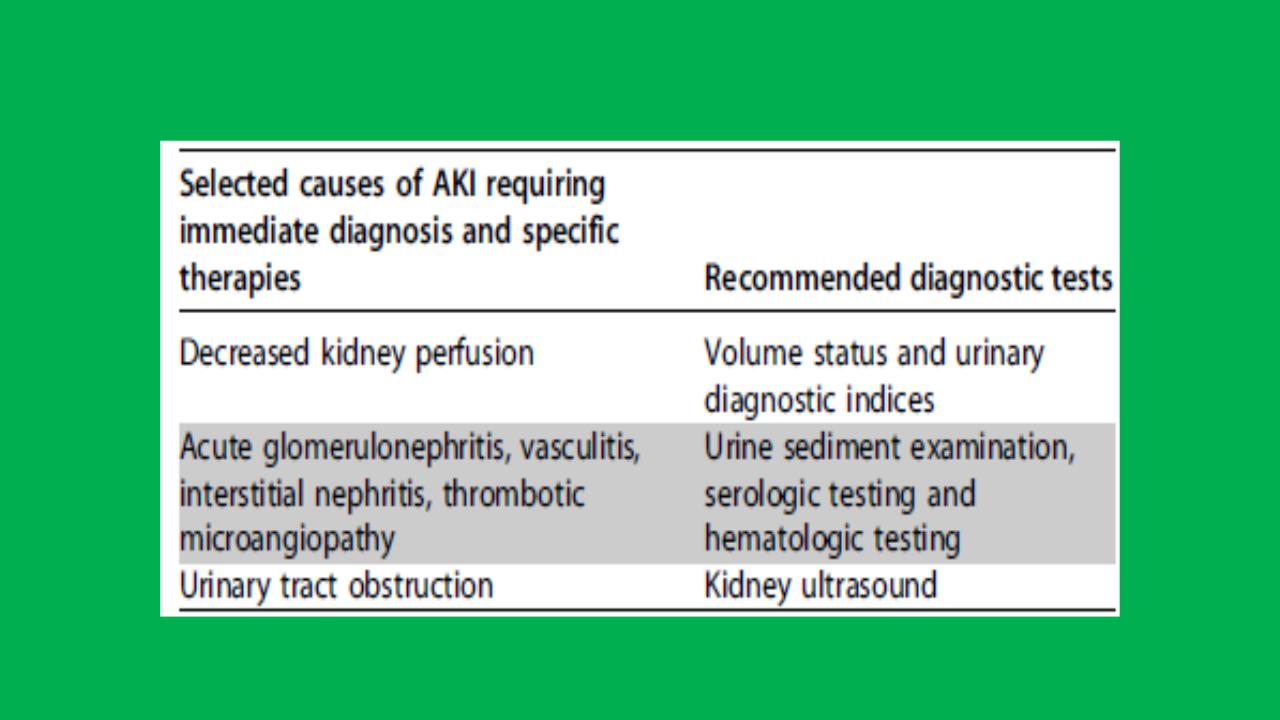
Causes of AKI and diagnostic tests
Exposure and susceptibility risk factors for non-specific AKI

Classification of AKI
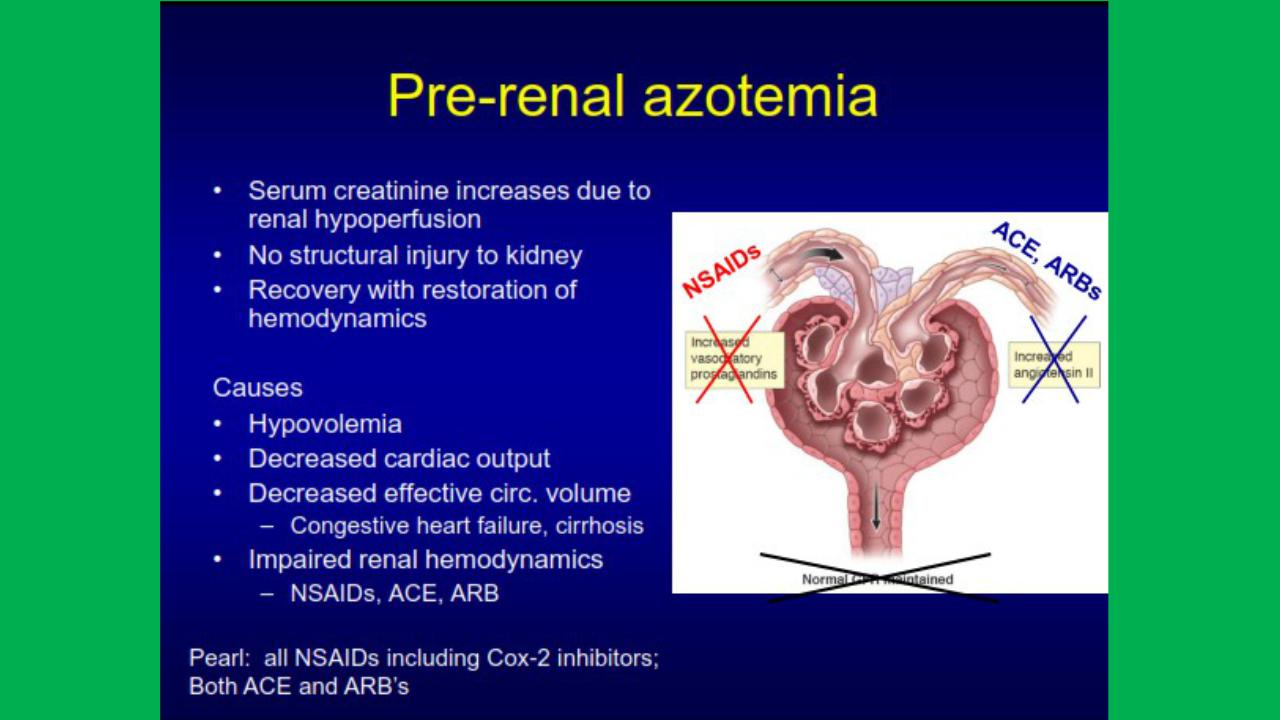
•Pre-renal
•Intrisic renal damage
•Post-renal
•Anuric
•< 50 cc / 24 hrs
•Oliguric
•< 500 cc / 24 hrs
•Non-olguric
•Normal urine output, but inadequate clearance
•GFR 2 ml/min will produce ~3L of urine/day if there is no tubular reabsorption