

SAOphthalmicAtlas&Guide
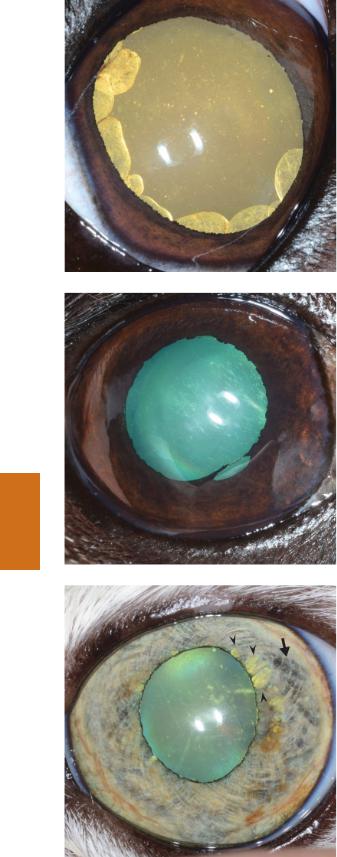
.pdfFigure 5.31 Chronic, superficial ulcerative keratoconjunctivitis and corneal sequestrum of the left eye of a Persian cat. Conjunctival hyperemia is present, and superficial corneal vessels extend from the dorsal and medial limbus. The sequestrum is the bronze to light brown discoloration in the central cornea. Corneal sequestra are discussed on pages 113 and 114.
Figure 5.32 Chronic, superficial ulcerative keratoconjunctivitis and corneal sequestrum. There is chemosis, conjunctival hyperemia, and superficial corneal vascularization. The vessels extend from the dorsal limbus to the sequestrum. In contrast to the previous figure, the sequestrum is dark brown. Mild corneal edema is present immediately around the sequestrum. Fluorescein stain has been applied to the eye. However, it is not retained over the sequestrum in spite of an epithelial defect due to the hydrophobic nature of the sequestrum. Corneal sequestra are discussed on pages 113 and 114.
Figure 5.33 Chronic, superficial ulcerative keratitis and corneal sequestrum. There is diffuse, superficial corneal vascularization. The sequestrum is the black, central corneal lesion. The cornea around the sequestrum is ulcerated. However, fluorescein is retained only at the periphery of the sequestrum because the sequestrum is hydrophobic. Corneal sequestra are discussed on pages 113 and 114.
Chapter 5 Cornea 31
Chapter 5

6 |
Anterior uvea |
|
Please see Chapter 15 for more information about diseases, diagnostic testing, and treatment plans related to the anterior uvea.
Figure 6.1 This photo was taken from the right side of the dog’s head to show PPMs spanning the anterior chamber. The PPMs are the thin, brown and white strands extending from the lateral iris collarette to the large, white opacity that obscures the view of the nasal pupillary margin. This opacity is corneal fibrosis at the PPM insertion. Discussion of PPMs can be found on pages 116 and 117.
Figure 6.2 These iris-to-iris PPMs were an incidental finding. The black arrowheads indicate PPMs on the iris (thin white strands). The PPMs at 2 and 8 o’clock lie flat on the iris, while the PPM at 10 o’clock crosses the pupillary aperture (red arrowhead) to insert onto the ventral iris collarette. Discussion of PPMs can be found on pages 116 and 117.
Small Animal Ophthalmic Atlas and Guide, First Edition. Christine C. Lim.
© 2015 John Wiley & Sons, Inc. Published 2015 by John Wiley & Sons, Inc.
32

Figure 6.3 Posterior synechiae. The synechiae arise from the pupillary margin from 6 to 9 o’clock and are adherent to the anterior lens capsule. Where present, these adhesions prevent complete dilation of the pupil, and mild dyscoria has resulted. Linear white opacities in the dorsal cornea are reflections and not true changes. Anterior uveitis is discussed on pages 121 to 124.
Figure 6.4 Anterior chamber uveal cysts. Two free-floating, circular brown objects were seen in the ventral anterior chamber. The horizontal white line seen over the larger, more dorsal cyst is a reflection of the eyelid margin. Transillumination confirmed both of these structures to be thin-walled uveal cysts, and no diagnostics or therapeutics were needed. Discussion of uveal cysts can be found on pages 117 and 118.
Figure 6.5 This patient was referred for evaluation of an intraocular mass. The round cyst is in the ventral anterior chamber. It is much darker brown than the cysts in the previous photograph. However, during transillumination, light was visualized passing through the structure, confirming it to be cystic. No treatment was needed. The white color change overlying the ventromedial eye is a reflection. Discussion of uveal cysts can be found on pages 117 and 118.
Chapter 6 Anterior uvea 33
Chapter 6
34 Section I Atlas
Figure 6.6 Transillumination of multiple posterior chamber cysts. The cysts are rounded objects visible at the pupillary margin from 3 to 11 o’clock. Transillumination causes the cysts to appear yellow; this is the effect of light passing through the thin walls of the cyst (which appear light brown in ambient light). Discussion of uveal cysts can be found on pages 117 and 118.
Figure 6.7 Scalloped pupillary margin due to age-related iris atrophy. The atrophy is more severe at the 5–6 o’clock pupillary margin, where there is a full-thickness defect of the iris. Discussion of iris atrophy can be found on page 118.
Chapter 6
Figure 6.8 Iris atrophy in the left eye of a 14-year-old, spayed female Persian. Thinning of the iris along the pupillary margin from 1 to 2 o’clock allows tapetal reflection to be visible through the iris tissue (arrowheads), giving the iris a moth-eaten appearance. At the adjacent iris collarette (arrow), the black posterior pigmented epithelium is visible through the thinned anterior iris stroma. Discussion of iris atrophy can be found on page 118.

Figure 6.9 Marked iris atrophy in the right eye of a 15-year-old, spayed female Chihuahua. The tapetal reflection is clearly visible through full-thickness iris defects. Dyscoria is also present as result of atrophy affecting the muscles of the iris. Discussion of iris atrophy can be found on page 118.
Figure 6.10 Focal, flat iridal hyperpigmentation (arrow) in a DSH. This was found incidentally during ophthalmic examination. The lesion was photographed at each visit, and at last examination, had not appreciably changed. A histopathologic diagnosis was therefore not obtained. Feline iris melanoma is further discussed on pages 118 and 119.
Figure 6.11 Histopathology confirmed iris melanoma in this 6-year-old, castrated male DSH. The iris is mildly thickened in the melanotic areas. Very mild dyscoria is present. Eversion of the pupillary margin, which allows visualization of the posterior pigmented epithelium, is present along the dorsal, medial, and ventral pupillary margins. Feline iris melanoma is discussed on pages 118 and 119.
Chapter 6 Anterior uvea 35
Chapter 6

36 Section I Atlas
Figure 6.12 This cat presented for evaluation of brown discoloration of the iris, which was previously yellow. Due to the considerable iris involvement, raised iridal surface, dyscoria, altered pupillary constriction, and IOP of 30 mm Hg, melanoma was suspected and enucleation recommended. Histopathology confirmed extensive iris melanoma. Feline iris melanoma is discussed on pages 118 and 119.
Figure 6.13 This dog was referred for evaluation and removal of a slow-growing, pigmented iridal mass in the left eye. The mass is flat, brown to black, and located within the peripheral iris from approximately 1 to 3 o’clock. Histopathology confirmed anterior uveal melanocytoma. Canine iris melanocytoma is further discussed on pages 119 and 120.
Chapter 6
Figure 6.14 Rapidly progressing iridal hyperpigmentation in the right eye of a 7-month-old, spayed female retriever cross. The bulk of the mass is visible within the medial iris. The affected iris is thickened and raised with impaired muscle function (dyscoria is visible, due to incomplete dilation of the medial pupil). Enucleation was performed. Histopathology confirmed iridal melanocytoma. Canine iris melanocytoma is further discussed on pages 119 and 120.

Figure 6.15 Iridociliary adenoma. The mass is pink because it contains little melanin and is vascular. It is located in the ventromedial posterior chamber of the left eye. The eye appeared comfortable and visual, but enucleation was recommended due to enlargement of the mass noted on serial visits. This condition is discussed on pages 120 and 121.
Figure 6.16 Anterior uveitis in the right eye of a dog. Chemosis and episcleral congestion are present, as well as deep corneal vasculature (visible at the lateral limbus) and marked corneal edema. The pupil was miotic. Anterior uveitis is discussed on pages 121 to 124.
Figure 6.17 Aqueous flare is pathognomonic for anterior uveitis. In a normal, uninflamed eye, light is reflected off the cornea (arrowhead) and anterior lens capsule (arrow), and the two reflections are separated by a dark space. However, in the presence of inflammation, anterior chamber debris (inflammatory cells and proteins) reflects light that traverses the anterior chamber. The result is a band of light visible between the corneal and the anterior lens capsule reflections (bracket). Anterior uveitis is discussed on pages 121 to 124.
Chapter 6 Anterior uvea 37
Chapter 6

38 Section I Atlas
Figure 6.18 Multiple bright white corneal opacities are visible in the ventral one-fourth of the cornea in this photograph. These are keratic precipitates, which are clusters of white cells and inflammatory debris adhered to the corneal endothelium. Presence of keratic precipitates indicates a past episode of anterior uveitis or current anterior uveitis. Anterior uveitis is discussed on pages 121 to 124.
Figure 6.19 Chronic, ulcerative, stromal keratitis and anterior uveitis in a 9-year-old, spayed female miniature poodle. Concurrent diseases included diabetes mellitus and KCS. This photograph depicts episcleral congestion, deep corneal vascularization, corneal stromal loss (black arrow), corneal fluorescein retention, and corneal edema. White blood cells have settled in the ventral anterior chamber (hypopyon). The multiple round, white opacities visible within the medial cornea (red arrowhead) are keratic precipitates. The ovoid, white opacity medial to the fluorescein uptake is the pupil (the black arrowhead indicates the dorsal pupillary margin). Both miosis and dyscoria are present. Anterior uveitis is discussed on pages 121 to 124.
Chapter 6
Figure 6.20 Hyphema in the left eye of a dog. Blood is present throughout the anterior chamber, but has settled ventrally as a result of gravity. Also visible in this photograph are deep corneal vessels (most noticeable along the ventral and medial limbus) and mild corneal edema (bluish-white discoloration most noticeable near the limbus). Anterior uveitis is discussed on pages 121 to 124.

Figure 6.21 Rubeosis iridis is increased redness of the iris due to inflammation. The color change is secondary to vascular engorgement and formation of new blood vessels. Also visible in this photo are deposits of inflammatory debris and red blood cells on the anterior lens capsule (seen within the dorsolateral pupil and paracentral pupil). Anterior uveitis is discussed on pages 121 to 124.
Figure 6.22 Focal rubeosis iridis and iris thickening in the left eye of a DSH with suspected spinal cord lymphoma. The lateral iris between the two arrows is raised, thickened, and more pink than normal. Dyscoria is also present. Anterior uveitis is discussed on pages 121 to 124.
Figure 6.23 Posterior synechiae. Two thin adhesions are visible extending from the pupillary margin to the anterior lens capsule at 3 and 7 o’clock. A broader adhesion is also present, arising from the pupillary margin from 3 to 6 o’clock. As a result of the adhesions, the ventromedial pupil is unable to completely dilate. A focal cataract is also present in the central lens. Anterior uveitis is discussed on pages 121 to 124.
Chapter 6 Anterior uvea 39
Chapter 6

40 Section I Atlas
Figure 6.24 Iris bombé following traumatic uveitis. Note the mild episcleral hyperemia and miotic pupil (due to uveitis). The pupillary and peripheral zones of the iris are located posterior relative to the iris collarette, which is billowing anteriorly. The small amount of visible lens is completely opaque, with a sparkly appearance indicating resorption. The crescent-shaped, white opacity near the limbus from 6 to 9 o’clock is a reflection.
Chapter 6