

Chapter 5
Abnormalities Involving the Pleura
Abnormalities involving the pleura include pathologic processes (masses, calcifications, infections, thickening) of the pleura, in addition to fluid and air collections within the pleural space. This chapter will start off with more common conditions such as pleural effusions and pneumothorax, followed by less common/ more complex processes.
Pleural Effusion
Definition: fluid in the potential space between the parietal and visceral pleura. This usually results in obliteration part or all of the hemidiaphragms (silhouette sign), blunting of the costophrenic angles both peripherally on the frontal projection and posteriorly on the lateral.
Case 5.1
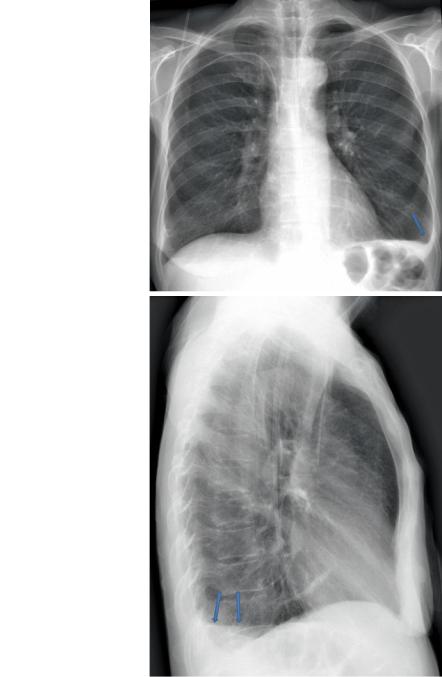
Figure 5.1 demonstrates a left pleural effusion on interdepartmental PA and lateral, a portable projection on same patient next day, then on CT.
Technique and Positioning Revisited
In the Chap. 2 of this book, we reviewed how technical factors such as rotation, X-ray energy, and markers are important. The preceding and following examples of the appearance of effusion also demonstrate how technique, especially portable positioning, is important in evaluating effusions, and differentiating them from other conditions such as consolidations.
L.R. Folio, Chest Imaging, DOI 10.1007/978-1-4614-1317-2_5, |
107 |
© Henry M. Jackson Foundation for the Advancement of Military Medicine, Inc. 2012 |
|
108
Fig. 5.1a,b PA (a) and lateral (b) erect projections of the chest demonstrate blunting of left costophrenic angle with a meniscus peripherally on the PA and posteriorly on the lateral (arrows). Also note the left PICC line with tip in SVC
5 Abnormalities Involving the Pleura
a
b