

Consolidation |
59 |
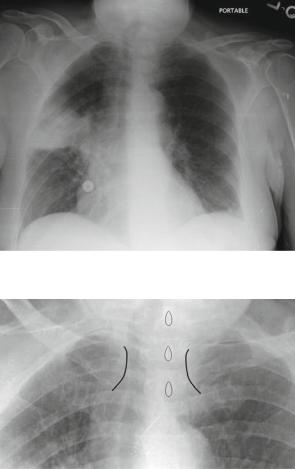
Fig. 4.33 Right upper lobe pneumonia; again limited inferiorly by the horizontal fissure, in this case making it resemble a mass
Fig. 4.34 Note the medial clavicles (outlined in black) and the orientation relative to the vertebral spinous processes (outlined in teardrop shapes). This indicates the patient is rotated toward their right
Water (Transudate)
Water can cause congestion and appear as airspace opacities/consolidation. See examples below for a transudate manifesting as a consolidation.
Pulmonary Edema
Pulmonary edema is not a disease by itself; it represents accumulation of fluid in extravascular lung from underlying process. We can divide it into four main categories based on pathophysiology.
60 |
4 Abnormal Lung Patterns |
1.Increase hydrostatic pressure edema: There are two phases: interstitial edema and alveolar edema. This is most commonly seen in left-sided heart failure in the ICU and ER. The interstitial phase often includes peribronchial cuffing and septal lines. The alveolar phase often includes batwing airspace opacities.
2.Permeability edema with diffuse alveolar damage: There are several precipitating factors unrelated to cardiac insufficiency. Pulmonary or extrapulmonary ARDS is the most severe and has three overlapping stages.
•Exudative stage: Interstitial edema resulting in alveolar filling (hence it skips the interstitial pattern).
•Proliferative stage: Inhomogeneous ground-glass opacities (can have a mixture of all three in this stage).
•Fibrotic stage: Cystic areas may be seen and can cause pneumothorax.
3.Permeability edema without diffuse alveolar damage: Often results in patchy, bilateral airspace opacities, ill-defined vessels, peribronchial cuffing. Unlike edema with diffuse alveolar damage, these findings can reverse. It is seen in heroin-induced pulmonary edema or following the administration of cytokines and in high-altitude pulmonary edema.
4.Mixed edema: This is generally an airspace opacification finding, depending on etiology (neurogenic, reperfusion, status post lung, transplant, re-expansion, post pneumonectomy, post reduction, air embolism).
Findings often vary in daily ICU CXRs, helping narrow differential to edema in that infection does not usually clear within a day or two (for example).
Case 4.11
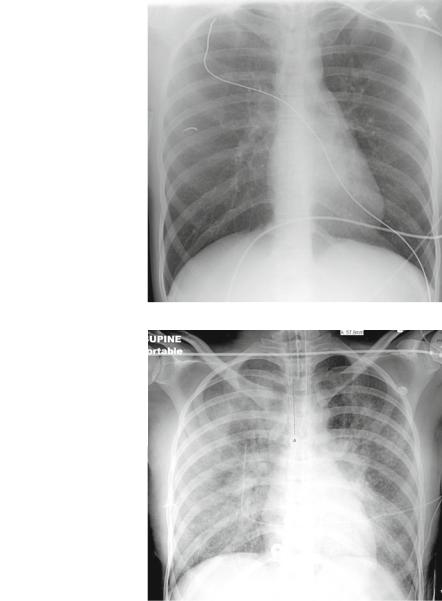
This first case is a young male suffering from an MI. Figures 4.35 and 4.36 demonstrate a fast transition from a normal CXR to an abnormal diffuse airspace process.
Findings: Bilateral and diffuse fluffy/patchy airspace and reticulo-nodular opacities. Also, ET tube tip is well above the carina (note measurement, 5.7 cm) and enteric tube in stomach.
Pattern: Consolidation, diffuse bilaterally. One could consider ground glass and reticulo-nodular (interstitial) pattern.
Differential Diagnosis: Acute (or Adult) Respiratory Distress Syndrome (ARDS), pulmonary edema (although small heart). The reason “pus” is not as highly considered is the acuteness of the process and the lack of fever or other infectious symptoms before the arrest. Also, pneumonias typically respect fissures and not immediately diffuse. The same goes for “cells” differential because this is a young patient who had a normal CXR hours before.
Diagnosis: Acute respiratory failure can occur two basic ways: failure of respiratory pump to deliver adequate oxygen to healthy lungs (neurogenic), or failure of
Consolidation |
61 |
Fig. 4.35 The first portable AP projection fails to demonstrate airspace opacities or other abnormality (normal CXR)
Fig. 4.36 This follow-up portable CXR (on the same patient) was obtained a few hours later in the ICU after the patient required ventilatory support. Note the diffuse patchy airspace opacities representing edema (transudate)
damaged lungs to manage gas exchange. Diffusely damaged lungs are characteristic of ARDS, which consists of acute respiratory distress, progressive hypoxemia refractory to oxygen administration, increasing lung stiffness, and diffuse radiographic lung opacification.