


76 |
4 Abnormal Lung Patterns |
Fig. 4.54 CT verifying reticulo-nodular pattern in the dependent lungs compatible with Pneumocystis jiroveci
Pneumonia (PJP)
Other causes of ground-glass opacities and interstitial infiltrates in patients with AIDS include CMV pneumonia, lymphocytic interstitial pneumonia, MAI infection, cryptococcal infection, Legionella, Mycoplasma, Chlamydia pneumoniae, AIDS-related lymphoma, Kaposi sarcoma, hypersensitivity pneumonia, and interstitial pulmonary edema from volume overload.
This patient was ultimately diagnosed with PJP by lung biopsy after a negative bronchoalveolar lavage [7].
Destructive Fibrotic Lung
The destructive process of pulmonary fibrosis (lung scarring resulting in restrictive lung) progresses by scar tissue gradually replacing normal lung tissue. This eventually results in lung tissue interspersed with pockets of air (holes). This process can lead to parts of the lung having a honeycomb-like appearance, as in the next case.
Case 4.18
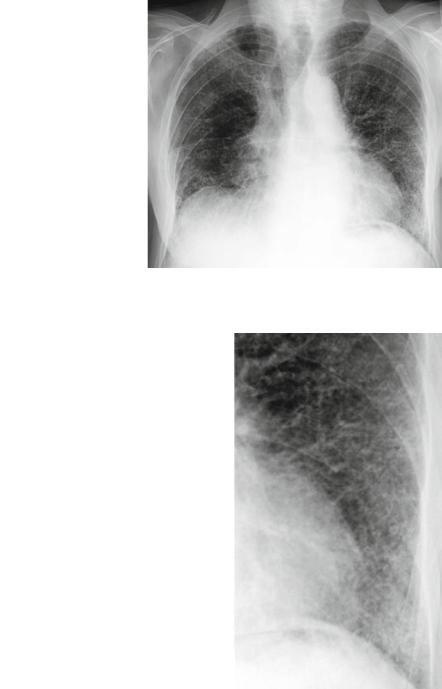
Figures 4.55–4.57 illustrate a case of fibrosing alveolitis and provide another example of a CXR with findings consistent with destructive findings (holes). This is most pronounced in the left lower lung.
Findings: honeycomb appearance.
Pattern: Interstitial, specifically, lines and holes.
Differential Diagnosis: Destructive lung, end-stage lung, lung fibrosis, scleroderma, LCH, LAM.
The following image is a CT of the lungs in a patient with a destructive pattern showing diffuse, stacked, irregular cyst formation.
Interstitial |
77 |
Fig. 4.55 Fibrosing alveolitis
Fig. 4.56 Close-up of same patient with fibrosing alveolitis; note the suggestion of holes peripherally