


78 |
4 Abnormal Lung Patterns |
Fig. 4.57 CT of destructive cyst formation, honeycomb pattern in periphery
Langerhans Cell Histiocytosis
When you see lines, dots, and holes together as in the images below, think about Langerhans cell histiocytosis (LCH). One can consider the differential for each set of lines, dots, and holes; however, this would be an extensive differential diagnosis. Considerations can be narrowed based on the severity of findings, the mixture of each entity, and the clinical history.
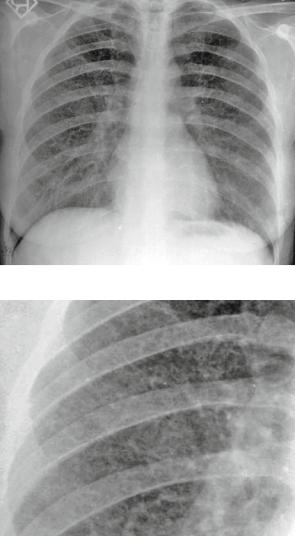
Case 4.19
Figures 4.58 and 4.59 are from a case of LCH.
Findings: Lines and dots diffusely distributed, with holes between lines. Pattern: Interstitial, specifically lines, dots, and holes.
Differential Diagnosis: Langerhans cell histiocytosis (LCH) and LAM (lymphangioleiomyomatosis). Again, one could consider an exhaustive differential (all of interstitial); however, the combination of lines, dots, and holes is typically seen in LCH.
Open lung biopsy supported LCH.
Vascular Pattern
Normal Pulmonary Vascular Anatomic Review
As mentioned previously, normal pulmonary markings (vessels, arteries for the most part) can typically be followed from the hilum toward the lung periphery in all directions. They branch at acute angles, taper, and diverge toward the periphery.
Vascular Pattern |
79 |
Fig. 4.58 CXR showing lines, dots, and holes together
Fig. 4.59 Close-up of CXR showing lines, dots, and holes
Pulmonary markings on-end appear as small masses or nodules. They are recognized as normal vessels by the fact that they are often superimposed upon vessels of the same diameter branching in other directions. They are also larger toward the hilum and similarly sized to vessels nearby.
Radiological Signs in the Vascular Pattern
Abnormal diameter or distribution/ distortion of pulmonary vasculature.