

90 |
4 Abnormal Lung Patterns |
Lobar Atelectasis (Collapse)
Atelectasis literally means incomplete expansion or loss of volume.
Signs
Primary
•Vessel asymmetry
•Fissure appears as an edge
Secondary
•Volume loss
•Elevation of diaphragm
•Shift of mediastinum and ribs
Patterns of lobar atelectasis as seen on CXRs are presented in the image below.
Lobar Atelectasis Patterns
The following figures and descriptions provide examples of the patterns of lobar atelectasis.
1.Right Upper Lobe (RUL, Fig. 4.66)
Collapse is superior and medially and creates a wedge-shaped opacity in the
right upper paramediastinal area on the frontal projection. The major fissure is displaced anteriorly and the minor fissure superiorly. There may be a triangular opacity with apex pointing toward hilum on lateral view. There is tracheal deviation to the right and superior displacement of the hilum. The right hemidiaphragm may be elevated. If there is a large central obstructing mass causing the atelectasis, you may have a convex bulge into the central medial portion of the displaced minor fissure. This will give a “Reverse S-sign of Golden.” There may be focal diaphragmatic tenting (juxtaphrenic peak sign) which is most commonly traction on the inferior accessory fissure.
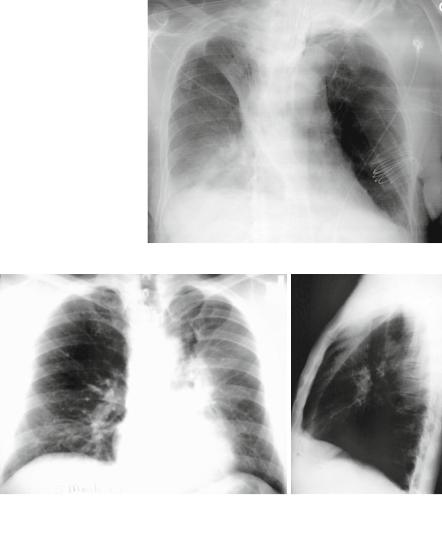
2.Left Upper Lobe (LUL, Fig. 4.67)
Due to lack of a left minor fissure, the appearance of LUL collapse is much dif-
ferent than RUL, except when an accessory left minor fissure is present. In such a case, the upper division of the LUL atelectasis will look like RUL atelectasis. Otherwise, the left major fissure is displaced anteriorly, roughly parallel to the anterior chest wall, and there is a band of opacity anterior to the major fissure. On the PA view, there is a hazy opacity that silhouettes the left heart border.
3. and 4. Lower Lobes (LLs, Figs. 4.68 and 4.69)
This pattern is similar in both the right and left lower lobes. Collapse is in posterior, medial, and inferior direction. The major fissure swings downward and backward. The hilum is displaced inferiorly, the hemidiaphragm is elevated. On the PA view,
Airway (Bronchial) Patterns |
91 |
Fig. 4.66 Example of RUL collapse
a |
b |
Fig. 4.67 Example of LUL collapse, AP (a) and lateral (b) projections. Note the overall increased density of the left hemithorax is due to the LUL collapsing anteriorly as seen on the lateral projection
there is a triangular opacity adjacent to the spine with the base on the hemidiaphragm. On the lateral view, there is increased opacity over the lower thoracic vertebrae with or without a smooth anterior margin, depending upon if the major fissure is tangential to the X-ray beam. The posterior aspect of the hemidiaphragm is obscured, unless the patient has an incomplete pulmonary ligament. Another indirect sign is the vascular nodular sign, which is a result of compensatory hyperinflation of the upper lobe. This is radiographically seen as “hair-pin” turning of vessels and “too-many nodules” along the cardiac margin, which are end-on vessels. Kattan’s triangle sign, which is the shifted v-shaped opacity superior to the anterior junction line, may also be seen.