

Airway (Bronchial) Patterns |
99 |
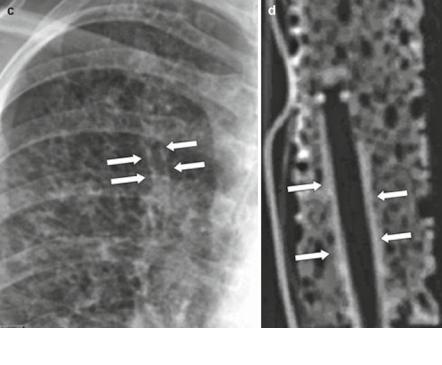
Fig. 4.75c, d Tram tracks in our patient (left image, c) and experimental analog with straw and sponge (right image, d)
one straw in oblique (right). The CT image shows the increased attenuation of the tape-wrapped straw mimicking bronchial wall thickening.
Side-by-side comparison of the in vivo tram track sign on the left and the experimental analog on the right. The arrows point to the thickened bronchiole walls seen in the CF patient, created in the same fashion by a straw wrapped in tape producing a thick wall around a hollow tube inside the sponge.
Figure 4.76a shows a CT of the chest in a patient with bronchiectasis, with obvious signet ring signs indicating bronchial dilation relative to the pulmonary arteries.
Figure 4.76b, c show the experimental model image using the sponge. There are two parallel straws of different diameters, the smaller having been filled with radioopaque material to simulate adjacent vessel, the large straw with air to represent enlarged bronchiole.
Bronchiolar
Radiological signs of a small airway obstruction are airway (“alveolar”) nodules, irregular in size, shape, and distribution; and, small, irregular lucencies. You can see a “Tree-in-bud” appearance on CT. This looks like branches of trees in the spring that start budding, typically only seen on CT.

100 |
4 Abnormal Lung Patterns |
Fig. 4.76a CT of bronchial dilation (bronchus is larger than the companion artery). Note the tracheomalacia of the carina
b |
c |
Fig. 4.76b, c Experimental model of enlarged bronchiole; the signet ring sign in the patient (b, left image) and the sponge (c, right image)
Potential differential diagnoses include the following:
•Infectious – viral, mycoplasmal, MAI, (Mycobacterium avium-intracellulare) fungal
•Allergic – hypersensitivity pneumonitis (HP): centrilobular nodules
•Toxic – especially: chlorine, phosgene, oxides of nitrogen
•Post-transplant
•Idiopathic
An overview of bronchiolar chest imaging patterns is available online at the Radiology Assistant website [10].
Case 4.21
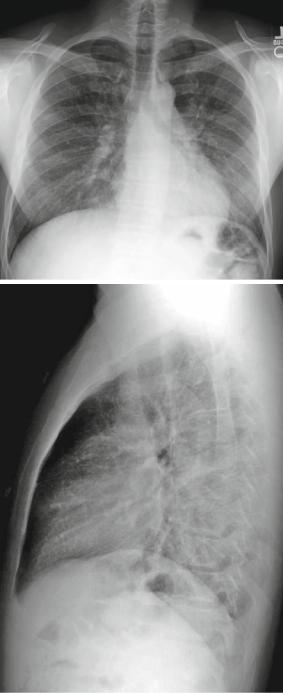
Figure 4.77 is that of a 34-year-old male with cough and dyspnea and no history of occupational exposures.
Airway (Bronchial) Patterns |
101 |
|
|
|
|
Fig. 4.77a, b CXRs of |
a |
|
bronchiolar pattern |
||
|
||
demonstrating a tracheogram |
|
|
(an air-bronchogram of the |
|
|
trachea) due to surrounding |
|
|
airway opacities |
|
b
102
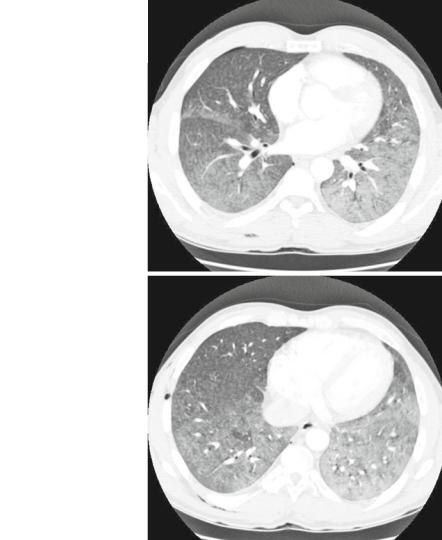
Fig. 4.77c, d HRCT of above case showing diffuse ground-glass and tree-in-bud opacities with suggestion of micronodules
4 Abnormal Lung Patterns
c
d
Findings: Bilateral, diffuse ground glass and scattered opacities causing a tracheogram (especially on left).
Pattern: Airway, specifically diffuse alveolar (centrilobular) nodular opacities. Other patterns considered: consolidative (alveolar opacities, however, can see vessels) and interstitial (nodular).
Differential
•Infectious – viral or atypical or idiopathic pneumonia
•Allergic – hypersensitivity pneumonitis
•Toxic
•Post-transplant

Airway (Bronchial) Patterns |
103 |
The following high resolution (HR) CT of the above case shows diffuse groundglass and tree-in-bud opacities with a suggestion of micronodules.
Diagnosis: Extrinsic allergic alveolitis (Hypersensitivity pneumonitis)
One needs a high index of suspicion to narrow to this differential diagnosis. This emphasizes why a good occupational and/or hobby exposure history is necessary since this process often manifests subtle findings.
Etiology: Sensitization to repeated inhalational exposure of organic antigens. These organic antigens include a variety of sources (dairy, grain and wood products, animal dander or proteins, and water reservoir vaporizers). The most common
a
b
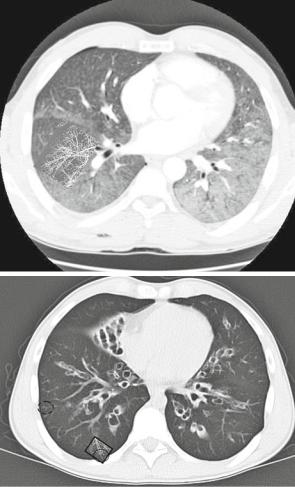
Fig. 4.78 (a, b) Demonstrates a color photograph of a tree-in-bud in the spring. This image was converted to black and white and inverted to help show CT findings (photo and processing by Dr. Folio). (c) This is a immunocompromised child with severe bronchiectasis and infectious bronchiolitis manifesting as centrilobular tree-in-bud opacities. (d) is a collage with the photo of an actual tree-in-bud, superimposed over the right lower lobe (outlined in black rectangle) to demonstrate similarity of the tree-in-bud finding and the origin of the term. Note how the blurry tree-in- bud in the patient (dotted circle) is similar in appearance to the imported photo
104 |
|
4 Abnormal Lung Patterns |
Fig. 4.78 |
(continued) |
c |
|
|
d
antigens are thermophilic actinomycetes and avian proteins. The most common diseases are farmer’s lung and bird fancier’s lung. Combination of clinical, radiographic, and pulmonary function tests. Bronchioalveolar lavage can suggest diagnosis. Biopsy may be needed in some cases. A great reference for HRCT findings is the University of California San Francisco Chest Primer [11].
The following should help the beginning radiology student to understand the tree-in-bud finding.