

новая папка / 80
.pdfAnatomy: Abdomen
Bowel
COLON AND ANUS
Transverse colon
Hepatic flexure
Ascending colon
Cecum
Appendix
Rectum
Urinary bladder
Prostate
External anal sphincter
Taenia coli
Splenic flexure
Superior mesenteric artery
Descending colon
Inferior mesenteric artery
Sigmoid
Rectum
Muscularis propria of rectum
Internal anal sphincter
Anal canal
(Top) Graphic shows the colon in situ. The transverse colon has been retracted upward to demonstrate the arterial supply of the colon from the superior and inferior mesenteric arteries. The SMA supplies the colon from the appendix through the splenic flexure, and the inferior mesenteric artery (IMA) supplies the descending colon through the rectum. Note the band of smooth muscle (taenia coli) running along the length of the intestine, which terminates in the vermiform appendix; these result in sacculations/haustrations along the colon, giving it a segmented appearance. (Bottom) Graphic shows the longitudinal section of a male pelvis. The anus is the external opening of the rectum and terminal end of the GI tract. The internal anal sphincter (IAS) is a thin involuntary muscle deep to the submucosa. The external anal sphincter is thicker, encircles the IAS, and is under voluntary control.
74
Bowel
Abdominal wall
Left hepatic vein
Gastro esophageal junction
Vertebral body
Abdominal wall
Left lobe of liver
Aorta
Vertebral body
Subcutaneous adipose tissue
Rectus muscle
STOMACH
Left lobe of liver
Stomach fundus
Collapsed body of stomach
Tail of pancreas
Anterior wall of stomach
Rugae
Posterior wall of stomach
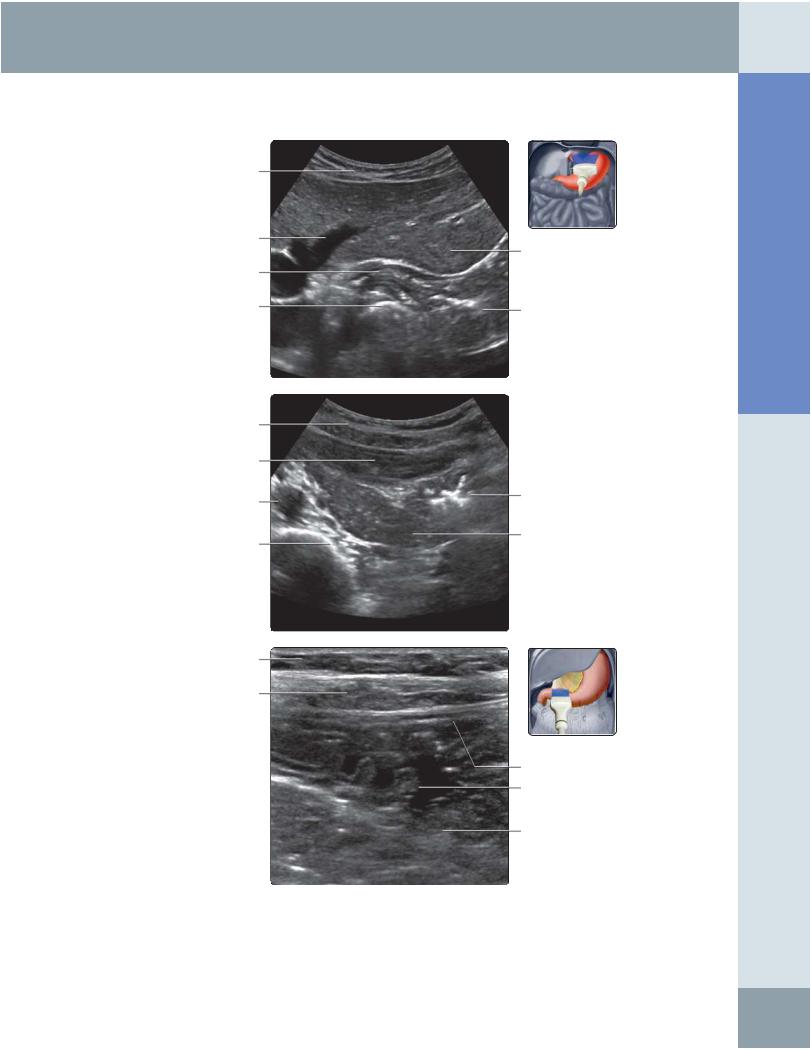
(Top) Transverse oblique ultrasound at the epigastric region shows the gastroesophageal (GE) junction, which can be traced to the fundus of the stomach. Note the relationship to the adjacent structures. (Middle) Transverse oblique ultrasound through the left upper quadrant shows the collapsed stomach body with the rugal folds. Echogenic gas is seen between the rugae. The tail of the pancreas is seen posterior to the stomach, and the left lobe of the liver is anterior to the stomach. (Bottom) High-resolution transverse ultrasound through the epigastric region shows the gastric body tapering to the gastric antrum. Note the gastric folds (rugae). The stomach wall shows the gut signature.
Abdomen Anatomy:
75
Anatomy: Abdomen
Bowel
GASTRODUODENAL REGION/DUODENUM
Subcutaneous adipose tissue
Left lobe of liver
Inferior vena cava
Abdominal wall
Superior mesenteric vein
Uncinate process of pancreas
D3
D2/D3 junction
Inferior vena cava
3rd part of duodenum (D3)
Inferior vena cava
Abdominal wall musculature
Pylorus
Duodenal bulb (D1)
Pancreas
Aorta
Gastric antrum
Superior mesenteric artery
D3/D4 junction
Aorta
Abdominal wall
Inferior mesenteric artery origin
Aorta
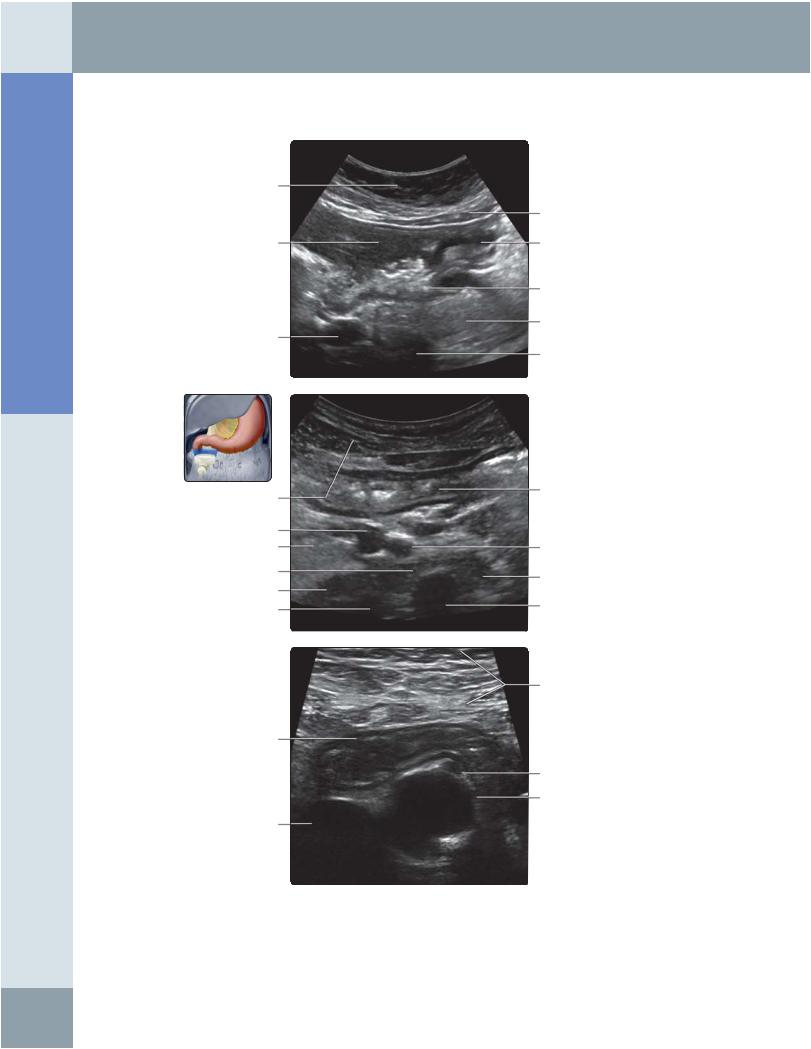
(Top) Transverse oblique ultrasound through the epigastric region shows the pylorus with the hypoechoic prominent muscular wall leading to the duodenal bulb. (Middle) Transverse ultrasound through the upper abdomen shows the gastric antrum anteriorly compressed by the curvilinear probe and collapsed 3rd part of the duodenum (D3) posteriorly. The SMA and the superior mesenteric vein (SMV) are seen in the plane in between. The inferior vena cava (IVC) and aorta are seen posterior to the D3. (Bottom) Axial midline high-resolution ultrasound through the upper abdomen shows fluid distended in the D3 located across, in the upper retroperitoneum. Note the aorta and IVC posterior to the D3. Gut signature is seen in the wall of the D3.
76
Bowel
SMALL BOWEL
Rectus muscle
Jejunal loops
Valvulae conniventes
Rectus muscle
Ileum
Jejunum with valvulae conniventes
Right rectus muscle
Anterior bowel wall
Ileal segment
Posterior bowel wall
Psoas muscle
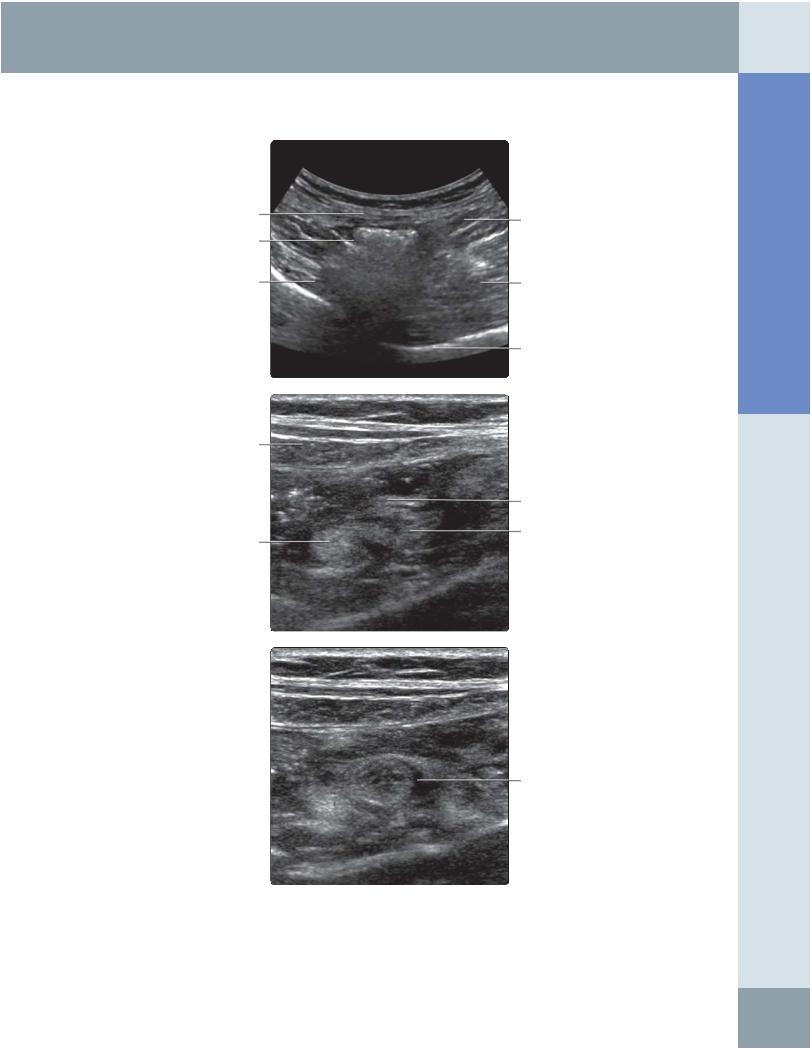
(Top) Transverse oblique ultrasound through the left flank shows jejunal loops with mucosal folds, valvulae conniventes. (Middle) Transverse ultrasound through the lower abdomen close to midline shows jejunal ileal transition from a segment with folds to a segment with no folds. (Bottom) Sagittal oblique ultrasound through the right lower quadrant (RLQ) shows a normal ileal segment. Note the lack of folds and a normal gut signature in the wall.
Abdomen Anatomy:
77
Anatomy: Abdomen
Bowel
SMALL BOWEL AND LARGE BOWEL
Cecum
Terminal ileum
Right iliopsoas complex
Cecum anterior wall
Ileocecal junction
Cecum posterior wall
Jejunal loops
Psoas muscle
Right common iliac artery
Right common iliac vein
Terminal ileum
Abdominal wall musculature
Descending colon
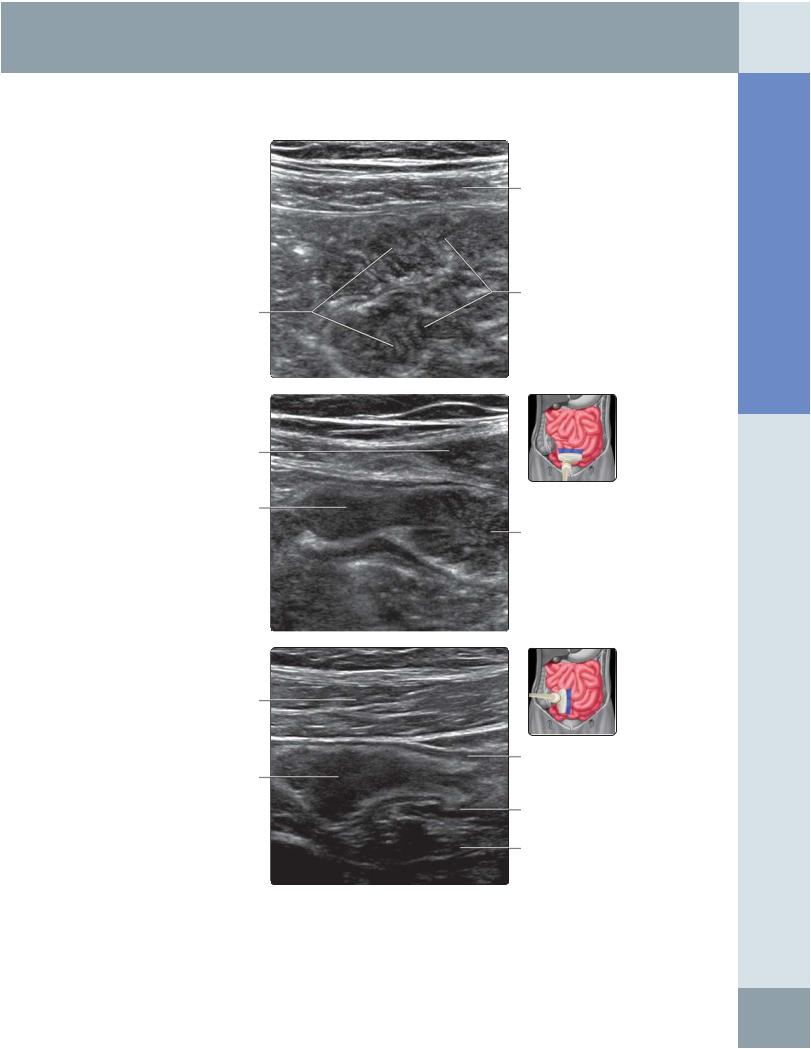
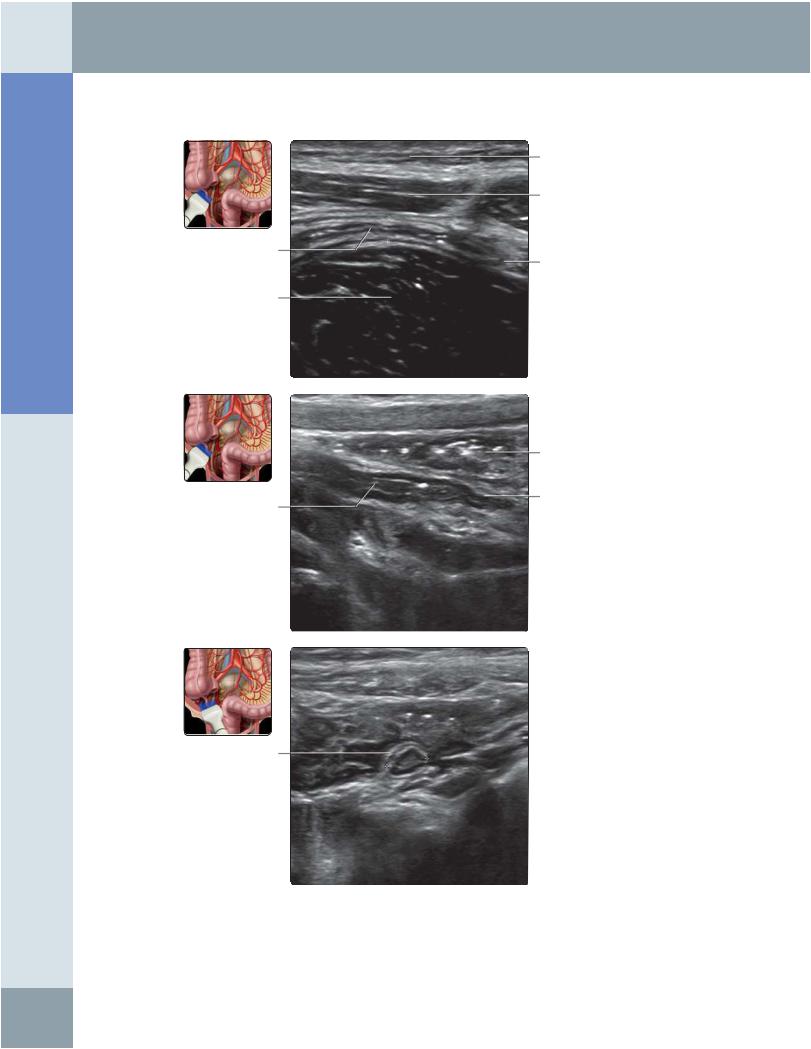
(Top) Transverse oblique ultrasound through the right iliac fossa (RIF) with graded compression shows a compressed, normal terminal ileum (between the abdominal wall musculature anteriorly and psoas muscle posteriorly) leading to the cecum. (Middle) Transverse high-resolution ultrasound through the RIF in the same patient shows the ileocecal junction and the ileocecal valve. (Bottom) Transverse ultrasound through the left iliac fossa (LIF) shows a short-axis view of the descending colon with gut signature. Medial to the descending colon, normal jejunal loops can be seen with valvulae conniventes.
78
Abdominal wall musculature
Cecum
Iliacus muscle
Abdominal wall musculature
Posterior lip of ileocecal junction
Bowel
ILEOCECAL JUNCTION
Terminal ileum
Psoas muscle
Iliac blade
Anterior lip of leocecal junction
Ileocecal junction
Ileocecal valve en face
Abdomen Anatomy:
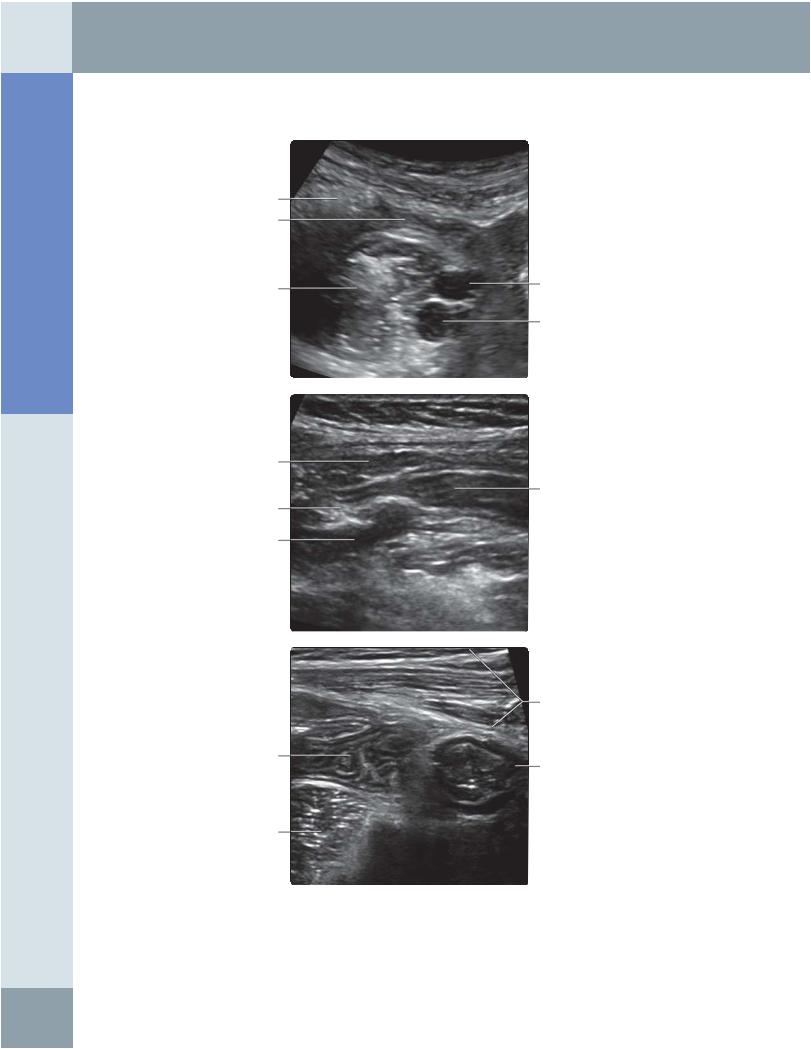
(Top) Transverse ultrasound through the RIF shows the cecum, which is represented by curvicurvilinear echogenicity with posterior reverberation. Note the terminal ileum compressed by the curvicurvilinear probe between the abdominal wall musculature and the iliopsoas complex posteriorly. (Middle) High-resolution transverse ultrasound through the RIF shows echogenic (fatty) lips of a normal ileocecal valve. (Bottom) Oblique right sagittal ultrasound through the RIF in the same patient shows the ileocecal junction end on.
79
Anatomy: Abdomen
Bowel
APPENDIX
Subcutaneous adipose tissue
Abdominal wall musculature
Appendix
Tip of appendix
Psoas muscle
Abdominal wall
Tip of appendix
Appendix
Short axis of normal appendix
(Top) Coronal oblique ultrasound through the RIF shows a long-axis normal appendix with a stratified mural appearance. Note the absence of peri appendicular inflammatory changes. (Middle) Transverse oblique ultrasound through the RIF shows a blind-ending tubular structure with a gut signature representing the long-axis view of a normal appendix. (Courtesy A. Law, MD.) (Bottom)
Transverse oblique ultrasound through the RIF shows the short-axis view of a normal appendix with preservation of gut signature. Note the normal appearance of peri appendicular fat. (Courtesy A. Law, MD.)
80
Bowel
LARGE BOWEL
Abdominal wall musculature
Haustra of ascending colon
Abdominal wall
Transverse colon
Posterior reverberation artefact from gas in transverse colon
Abdominal wall musculature
Outer muscular layer of colon
Descending colon
Posterior reverberation artefact
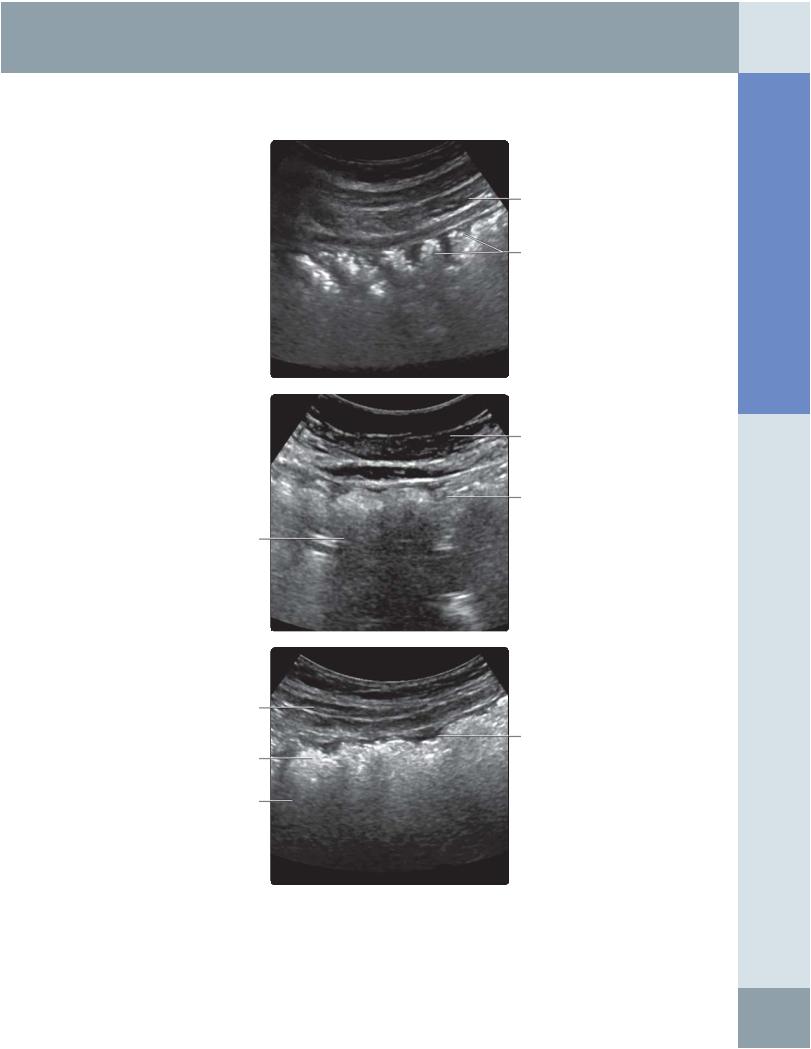
(Top) Right sagittal ultrasound shows a normal ascending colon with curvicurvilinear arcs of echogenicity from luminal gas/feces reflecting the normal haustra pattern. (Middle) Transverse ultrasound through the epigastric region close to the midline shows the normal haustral pattern of intraluminal gas/feces within the horizontally lying transverse colon. Note the posterior reverberation artifact from a gas-filled colon. (Bottom) Left sagittal ultrasound through the left side of the abdomen shows the descending colon represented by arcs of echogenicity with posterior reverberation artifacts due to gaseous contents of the colon. Note the normal haustral pattern. Images obtained with curvilinear probe or linear probe with virtual convex are better for orientation of anatomy within the peritoneal cavity.
Abdomen Anatomy:
81
Anatomy: Abdomen
Bowel
LARGE BOWEL
Abdominal wall musculature
Abdominal wall
Compressed lumen
Psoas muscle
Loops of pelvic loops of small bowel
Muscularis propria layer
Long-axis view of collapsed descending colon
Muscularis propria layer
Submucosal layer
Muscularis mucosa
Compressed lumen
Muscularis propria layer
Sigmoid colon
Iliacus muscle in pelvic wall
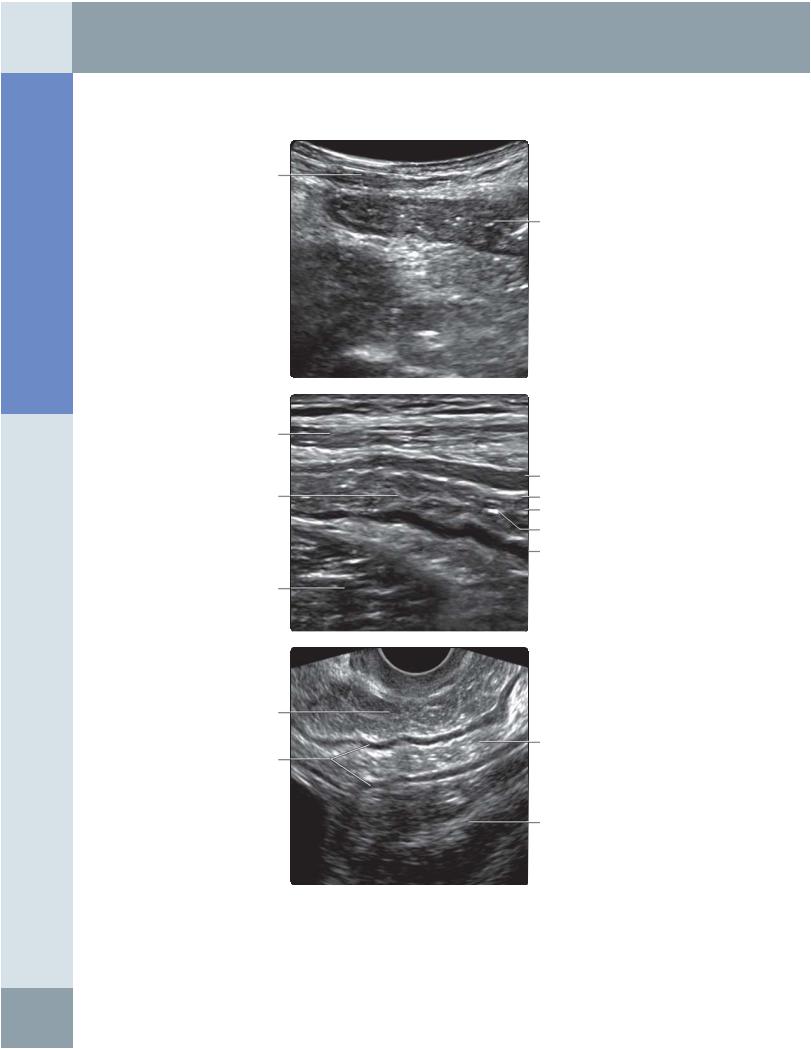
(Top) Left sagittal ultrasound shows the normal descending colon in a collapsed state and compressed by the ultrasound probe. Note the gut signature. This is an alternative appearance to the descending colon when it is collapsed and empty. (Middle) High-resolution left sagittal ultrasound obtained with a higher frequency linear probe from the same patient shows the collapsed descending colon with gut signature. The hypoechoic outer layer represents the muscularis propria layer. (Bottom) Transvaginal ultrasound shows the sigmoid colon and pelvic loops of small bowel. Note the hypertrophied outer muscularis propria layer of the sigmoid colon, seen in patients with irritable bowel syndrome and early diverticular disease.
82
Bowel
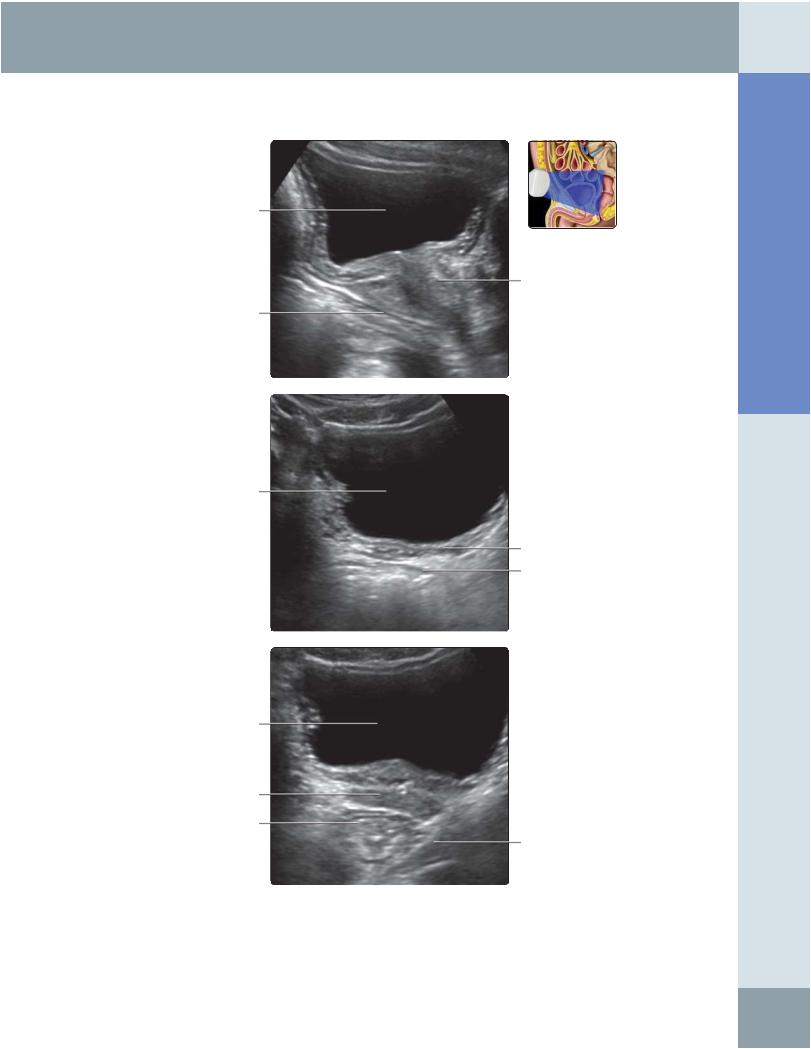
RECTOSIGMOID REGION
Urinary bladder
Prostate gland
Anterior wall of rectosigmoid
Bladder
Seminal vesicles
Anterior wall of rectum
Bladder
Base of prostate gland
Lower rectum
Puborectalis
(Top) Midline sagittal ultrasound in a male patient shows the anterior wall of the rectosigmoid region and its relationship to the prostate gland anteriorly. (Middle) Transverse ultrasound through the pelvis in the same patient (with cystic fibrosis) shows the anterior wall of the rectosigmoid region and its relationship to the seminal vesicles anteriorly (note the small seminal vesicles seen here). (Bottom) Transverse ultrasound at a lower level in the same patient shows the lower rectum, pelvic floor, and anterior relationship to the prostate gland.
Abdomen Anatomy:
83