

новая папка / 80
.pdfAnatomy: Abdomen
Kidneys
GROSS ANATOMY
Overview
•Kidneys are paired, bean-shaped, retroperitoneal organs
○Function: Remove excess water, salts, and wastes of protein metabolism from blood
Anatomic Relationships
•Lie in retroperitoneum, within perirenal space, surrounded by renal fascia (of Gerota)
•Each adult kidney is ~ 9-14 cm in length, 5 cm in width
•Both kidneys lie on quadratus lumborum muscles, lateral to psoas muscles
Internal Structures
•Kidneys can be considered hollow with renal sinus occupied by fat, renal pelvis, calyces, vessels, and nerves
•Renal hilum: Where arteryenters, vein and ureter leave renal sinus
•Renal pelvis: Funnel-shaped expansion of upper end of ureter
○Receives major calyces (infundibula) (2 or 3), each of which receives minor calyces (2-4)
•Renal papilla: Pointed apex of renal pyramid of collecting tubules that excrete urine
○Each papilla indents a minor calyx
•Renal cortex: Outer part, contains renal corpuscles (glomeruli, vessels), proximal portions of collecting tubules and loop of Henle
•Renal medulla: Inner part, contains renal pyramids, distal parts of collecting tubules, and loops of Henle
•Vessels, nerves, and lymphatics
○Artery
–Usually 1 for each kidney
–Arise from aorta at about L1-L2 vertebral level
○Vein
–Usually 1 for each kidney
–Lies in front of renal artery and renal pelvis
○Nerves
–Autonomic from renal and aorticorenal ganglia and plexus
○Lymphatics
–To lumbar (aortic and caval) nodes
IMAGING ANATOMY
Overview
•Well-defined retroperitoneal bean-shaped structures, which move withrespiration
Internal Contents
•Renal capsule
○Normal kidneys are well-defined due to presence of renal capsule and are less reflective thansurrounding fat
•Renal cortex
○Renal cortex has reflectivity that is less than adjacent liver or spleen
○If renal cortex brighter than normal liver (echogenic), then high suspicion of renal parenchymal disease
•Medullary pyramids
○Medullary pyramids are less reflective than renal cortex
•Corticomedullary differentiation
○Margin between cortex and pyramids is usually welldefined in normal kidneys
○Margin between cortex and pyramids maybe lost in presence of generalized parenchymal inflammation or edema
•Renal sinus
○Echogenic due to fat that surrounds blood vessels and collecting systems
○Outline of renal sinus is variable, from smooth to irregular
○Renal sinus fat may increase in obesity, steroid use, and sinus lipomatosis
○Renal sinus fat may decrease in cachectic patients and neonates
○If sinus echoes are indistinct in noncachectic patient, tumor infiltration or edema should beconsidered
•Collecting system (renal pelvis and calyces)
○Not usually visible in dehydrated patient
○May be seen as physiological "splitting" of renal sinus echoes in patients with a full bladder undergoing diuresis
○Physiological "splitting" of renal sinus echoes is common in pregnancy
–Cause of dilatation of pelvicalyceal system may be due to mechanical obstruction by enlarging uterus, hormonal factors, increased blood flow, and parenchymal hypertrophy
–May occur as early as 12 weeks into pregnancy
–Seen in up to 75% of right kidneys at 20 weeks into pregnancy, less common on left side, thought to be due to cushioning of ureter from gravid uterus by sigmoid colon
–Obvious dilatation of pelvicalyceal system can be seen in 2/3 of patients at 36 weeks
–Changes usually resolve within 48 hours after delivery
○Possible obstruction can be excluded by performing post micturition images of collecting system
–AP diameter of renal pelvis in adults should be < 10 mm
•Renal arteries
○Normal caliber 5-8 mm
○2/3 of kidneys are supplied by single renal artery arising from aorta
○1/3 of kidneys are supplied by 2 or more renal arteries arising from aorta
–Main renal artery may be duplicated
–Accessory renal arteries may arise from aorta superior or inferior to main renal artery
–Accessory renal arteries may enter kidney either in hilum or at poles
–Extrahilar accessory renal arteries may arise from ipsilateral renal artery, ipsilateral iliac artery, aorta, or retroperitoneal arteries
○Spectral Doppler
–Open systolic window, rapid systolic upstroke occasionally followed by secondary slower rise to peak systole with subsequent diastolic delay but persistent forward flow in diastole
–Continuous diastolic flow is present due to low resistance in renal vascular bed
–Low resistance flow pattern is also present in intrarenal branches
44
Kidneys
–Normal peak systolic velocity (PSV) 75-125 cm/s, not more than 180 cm/s
□ > 200 cm/s is abnormal
–Resistive index (RI) is (peak systolic velocity - end diastolic velocity)/peak systolic velocity; normal < 0.7
–Pulsatility index (PI) is (peak systolic velocity - end diastole velocity)/mean velocity, normal < 1.8
•Renal veins
○Normal caliber 4-9 mm
○Formed from tributaries that coalesce at renal hilum
○Right renal vein is relatively short and drains directly into IVC
○Left renal vein receives left adrenal vein from above and left gonadal vein from below
○Left renal vein crosses midline between aorta and superior mesenteric artery
○Spectral Doppler
–Normal PSV 18-33 cm/s
–Spectral Doppler in right renal vein mirrors pulsatility in IVC
–Spectral Doppler in left renal vein may show only slight variability of velocities consequent upon cardiac and respiratory activity
Size
•Bipolar length is found by rotating transducer around its vertical axis such that the longest craniocaudal length can be identified
•Normal size between 10-15 cm
•Volume measurements
○May be more accurate, but is time consuming
○3D ellipsoidal formula can be used for volume estimation
– Length x AP diameter x transverse diameter x 0.5
○Consistency and changes in volume over time more important
ANATOMY IMAGING ISSUES
Imaging Recommendations
•Right kidney
○Liver used as acoustic window
○Transducer placed in subcostal or intercostal position
○Varying degree of respiration is useful
○Raising patient's right side and scanning laterally/posterolaterally may be useful
•Left kidney
○More difficult to visualize due to bowel gas from small bowel and splenic flexure
○Usually easier to search for left kidney using posterolateral approach with left side raised
○Full right lateral decubitus with pillow under right flank and left arm extended above head may be useful in difficult cases
–Spleen can be used as acoustic window for imaging upper pole of left kidney
○Posterior approach
–Useful for intervention procedures (renal biopsy, nephrostomy)
–Image quality may be impaired by thick paraspinal muscles and ribs shadowing
•Renal arteries
○Origins best seen from midline anterior approach
○Right renal artery can usually be followed from origin to kidney
○Left renal artery often requires posterolateral coronal transducer scanning position for visualization
•Renal veins
○Best seen on transverse scan from anterior approach
○May also be seen on coronal scan from posterolateral coronal
Key Concepts
•Accessory renal vessels
○Must be accounted for in planning surgery (e.g., resection, transplantation)
○Often are best seen using multidetector row CT, magnetic resonance angiogram, or digital subtraction angiography rather than ultrasound
EMBRYOLOGY
Embryologic Events
•Congenital anomalies of renal number, position, structure, and form are very common
○Often accompanied by anomalies of other systems
○VATER acronym: Vertebral, anorectal, tracheoesophageal, radial ray, renal
○Congenital absence of kidney
○Anomalies of position (ectopia) are common
○Anomalies of structure
–Congenitally large septum of Bertin (lobar dysmorphism); asymptomatic
–Fetal lobulations (lobation), single or multiple indentations of lateral renal contours
–Partial duplication: Commonly results in enlarged kidney with 2 separate hila, 2 ureters (may join downstream or join bladder separately); duplex kidney = bifid renal pelvis, single ureter
Abdomen Anatomy:
45
Anatomy: Abdomen
Kidneys
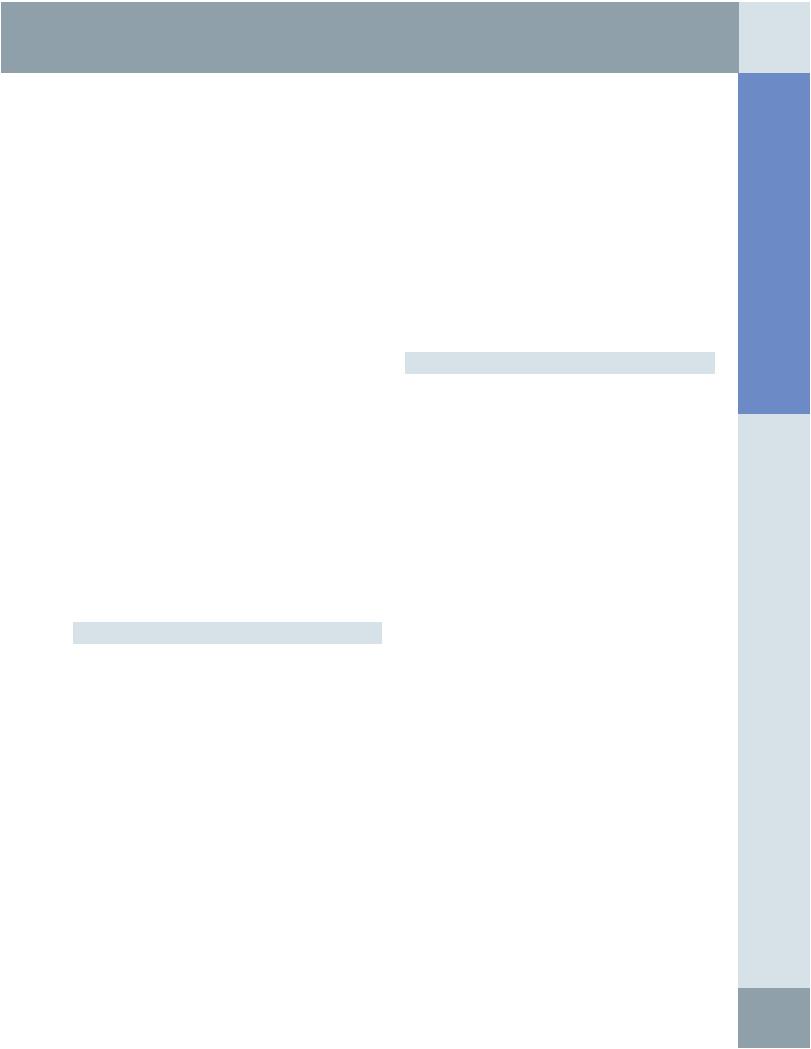
KIDNEYS IN SITU
Right adrenal vein
Renal veins
Right gonadal vein
Capsule (incised & peeled back)
Inferior phrenic vessels
Left inferior adrenal vessels
Left gonadal vein
Superior mesenteric artery
Gonadal arteries
Inferior mesenteric artery
Renal artery
Renal vein
Renal pelvis
(Top) The kidneys are retroperitoneal organs that lie lateral to the psoas and "on" the quadratus lumborum muscles. The oblique course of the psoas muscles results in the lower pole of the kidney lying lateral to the upper pole. The right kidney usually lies 1-2 cm lower than the left, due to inferior displacement by the liver. The adrenal glands lie above and medial to the kidneys, separated by a layer of fat and connective tissue. The peritoneum covers much of the anterior surface of the kidneys. The right kidney abuts the liver and the hepatic flexure of the colon and duodenum, while the left kidney is in close contact with the pancreas (tail), spleen, and splenic flexure. (Bottom) The fibrous capsule is stripped off with difficulty. Subcapsular hematomas do not spread far along the surface of the kidney, but compress the renal parenchyma, unlike most perirenal collections.
46
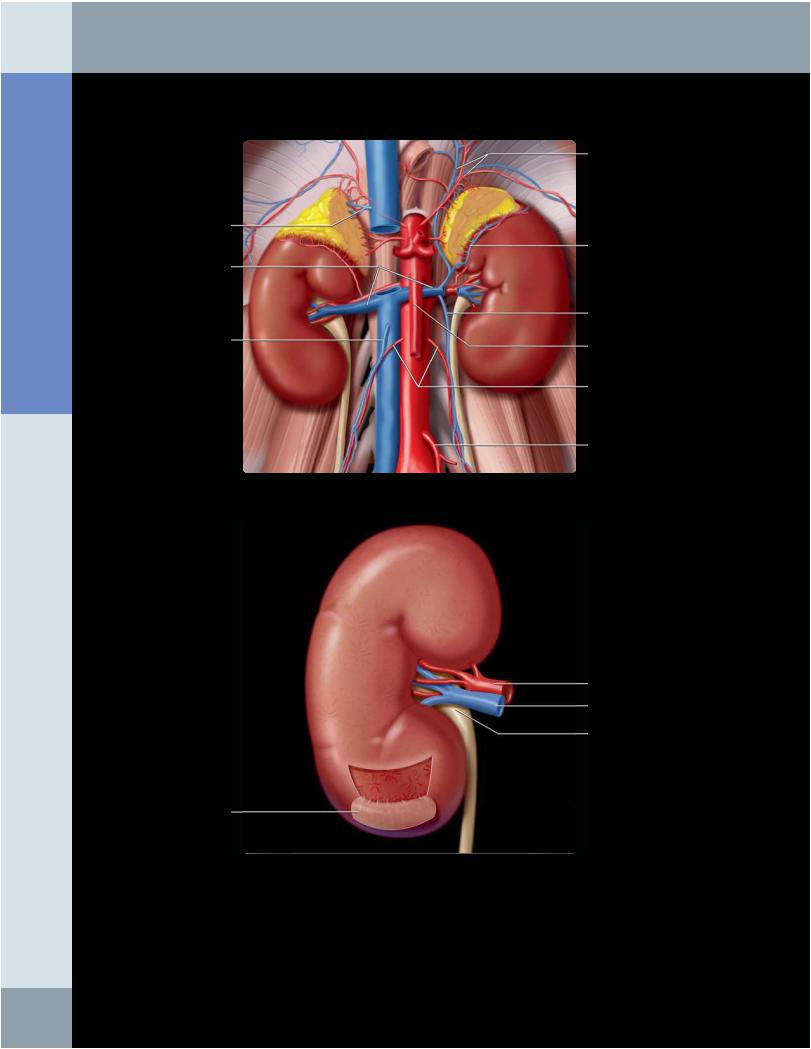
Adrenal
Cortical column (of
Bertin)
Inferior adrenal artery
Superior segmental artery
Posterior segmental artery
Renal artery
Inferior segmental artery
Pelvic & ureteric branches
Renal papilla
Kidneys
KIDNEY ARTERIES AND INTERIOR ANATOMY
Arcuate arteries
Interlobar arteries
Interlobular arteries
Anterior superior segmental artery
Anterior inferior segmental artery
Renal pyramid
Renal cortex
Abdomen Anatomy:
The kidney is usually supplied by a single renal artery, the 1st branch of which is the inferior adrenal artery. It then divides into 5 segmental arteries, only 1 of which (the posterior segmental artery) passes dorsal to the renal pelvis. The segmental arteries divide into the interlobar arteries that lie in the renal sinus fat. Each interlobar artery branches into 4 to 6 arcuate arteries that follow the convex outer margin of each renal pyramid. The arcuate arteries give rise to the interlobular arteries that lie within the renal cortex, including the cortical columns (of Bertin) that invaginate between the renal pyramids. The interlobular arteries supply the afferent arterioles to the glomeruli. The arterial supply to the kidney is vulnerable, as there are no effective anastomoses between the segmental branches, each of which supplies a wedge-shaped segment of parenchyma.
47
Anatomy: Abdomen
Kidneys
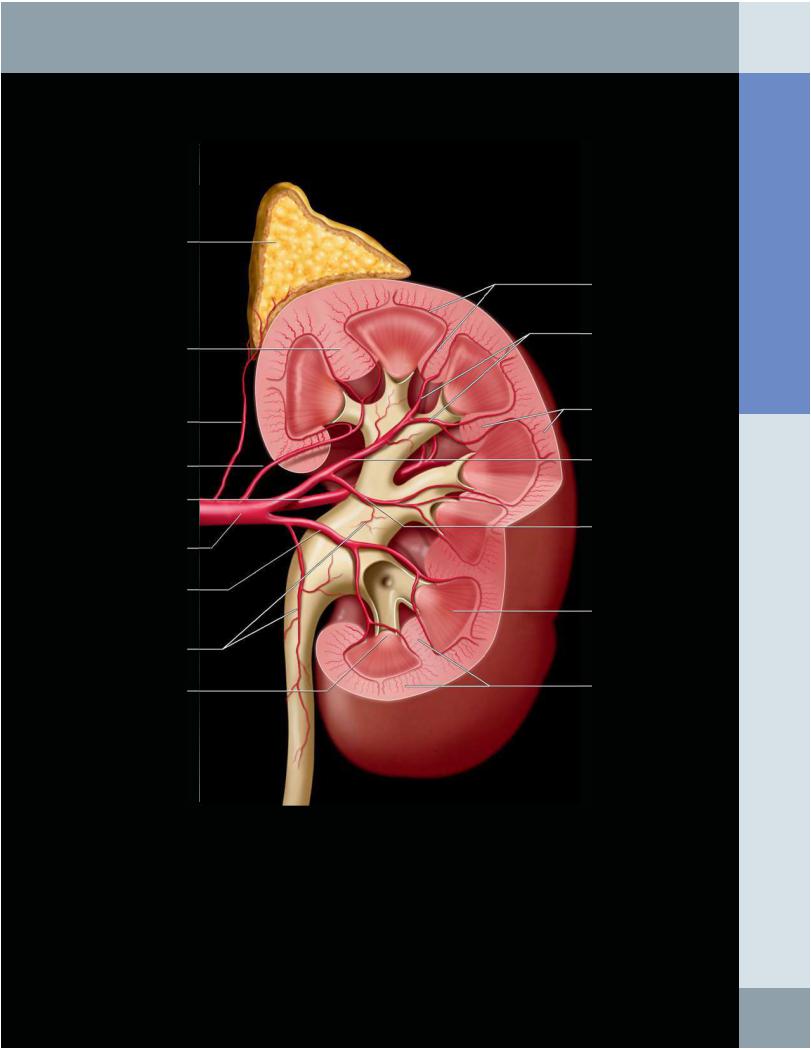
CT UROGRAM
12th rib |
Minor calyces |
|
Major calyces
Renal pyramids
Renal pelvis
Ureter
Urinary bladder
A coronal reconstruction of a series of axial CT sections can be viewed as a surface-rendered 3D image to simulate an excretory urogram. The window levels and work station controls have been set to optimally display the renal collecting system. The color scale is arbitrary; in this case, opacified urine is displayed as white. Less dense urine within the renal tubules in the pyramids and the diluted urine within the bladder are displayed as red. The CT scan was obtained in suspended inspiration, resulting in caudal displacement of the kidneys. In the supine position at quiet breathing, the upper poles of the kidneys usually lie in front of the 12th ribs.
48
Kidneys
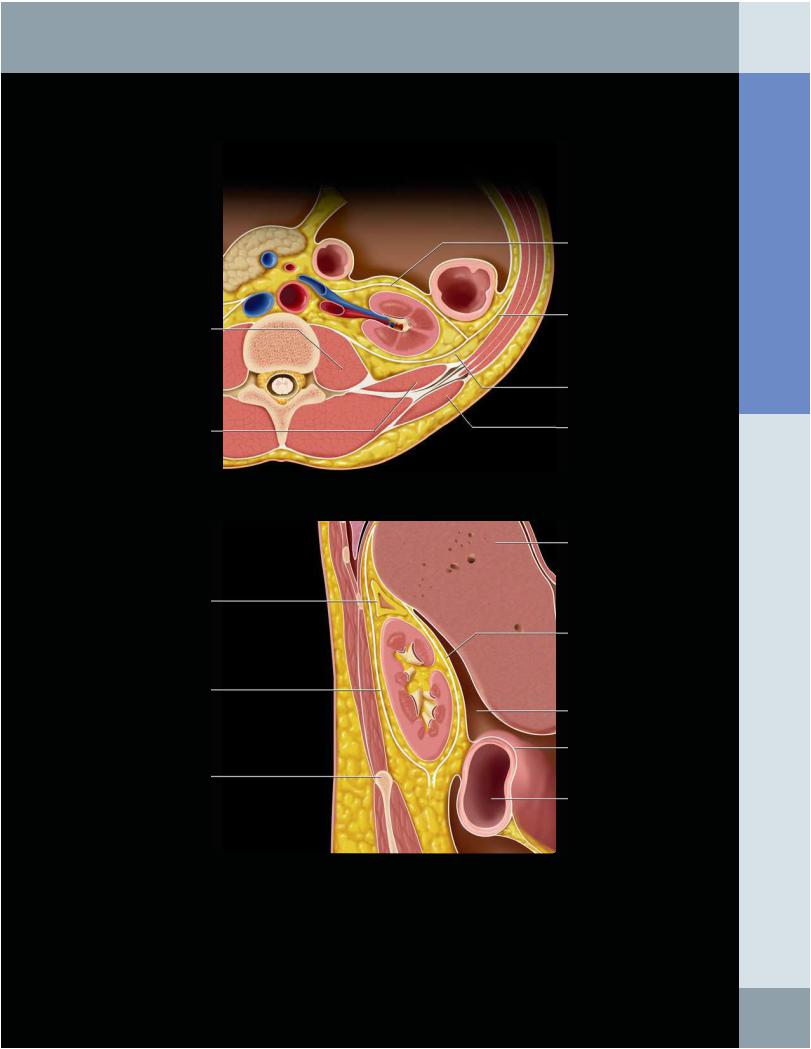
RENAL FASCIA AND PERIRENAL SPACE
Psoas (major) muscle
Quadratus lumborum muscle
Adrenal gland
Posterior renal fascia
Iliac crest
Anterior renal fascia
Lateroconal fascia
Posterior renal fascia
Latissimus dorsi muscle
Liver
Anterior renal fascia
Hepatorenal fossa (Morison pouch)
Peritoneum
Transverse colon
(Top) The anterior and posterior layers of the renal fascia envelope the kidneys and adrenals along with the perirenal fat. Medial to the kidneys, the course of the renal fascia is variable (and controversial). The posterior layer usually fuses with the psoas or quadratus lumborum fascia. The perirenal spaces do not communicate across the abdominal midline. However, the renal and lateroconal fasciae are laminated structures that may be distended with fluid collections to form interfascial planes that do communicate across the midline and also inferiorly to the extraperitoneal pelvis. (Bottom) A sagittal section through the right kidney shows the renal fascia enveloping the kidney and adrenal gland. Inferiorly, the anterior and posterior renal fasciae come close together at about the level of the iliac crest. Note the adjacent peritoneal recesses.
Abdomen Anatomy:
49
Anatomy: Abdomen
Kidneys
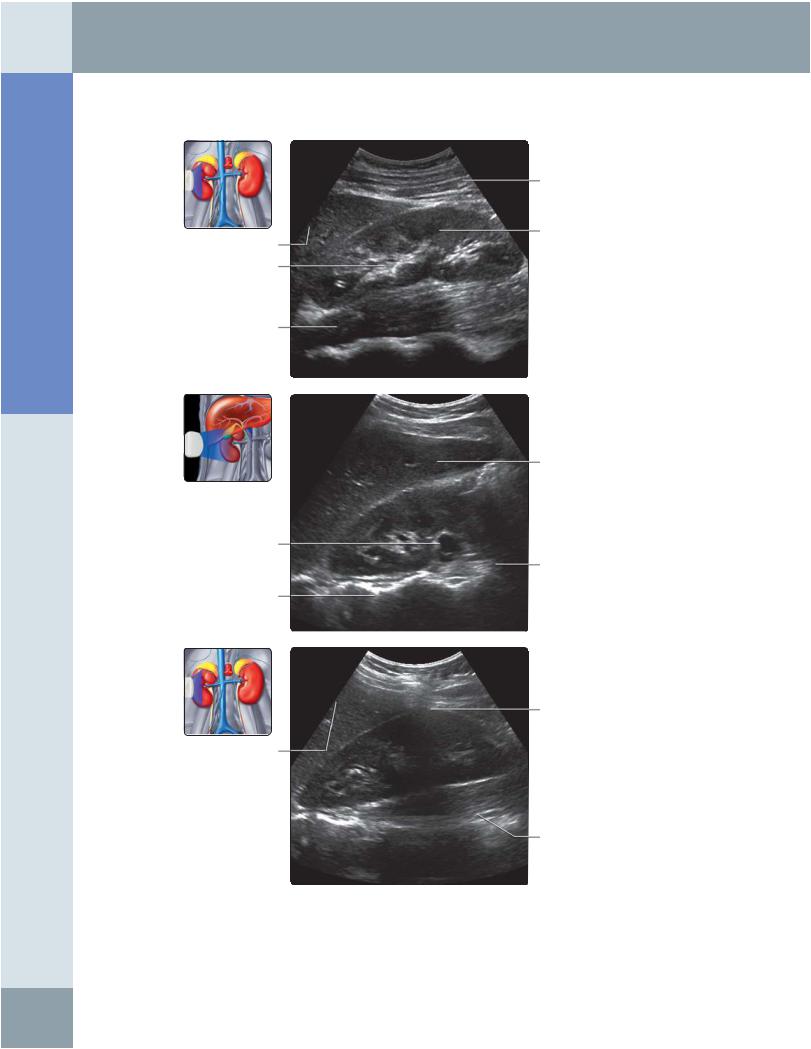
RIGHT KIDNEY, ANTERIOR ABDOMEN SCAN
Oblique muscles
Medullary pyramid
Right lobe of liver
Renal sinus
Psoas muscle
Right lobe of liver
Right main renal vein
Psoas muscle
Vertebral bodies
Shadowing from rib
Right lobe of liver
Right psoas muscle
(Top) Longitudinal grayscale ultrasound of the right kidney using the liver as an acoustic window is shown. This approach usually provides excellent visualization of the right kidney and is useful for measuring bipolar renal length. (Middle) Longitudinal oblique grayscale ultrasound of the right kidney using the liver as an acoustic window with the view obtained with a bit more medial angulation (when compared with the previous image). (Bottom) Longitudinal oblique grayscale ultrasound of the right kidney using the liver as an acoustic window with the view obtained with more lateral angulation (when compared with the previous 2 images) cuts through the renal parenchyma on the lateral aspect of the right kidney. Note that the echogenic sinus is not demonstrated and that there is shadowing from ribs.
50
Right hemidiaphragm
Renal cortex
Pelvicalyceal system
Right kidney
Right main renal vein
Right hemidiaphragm
Right kidney
Kidneys
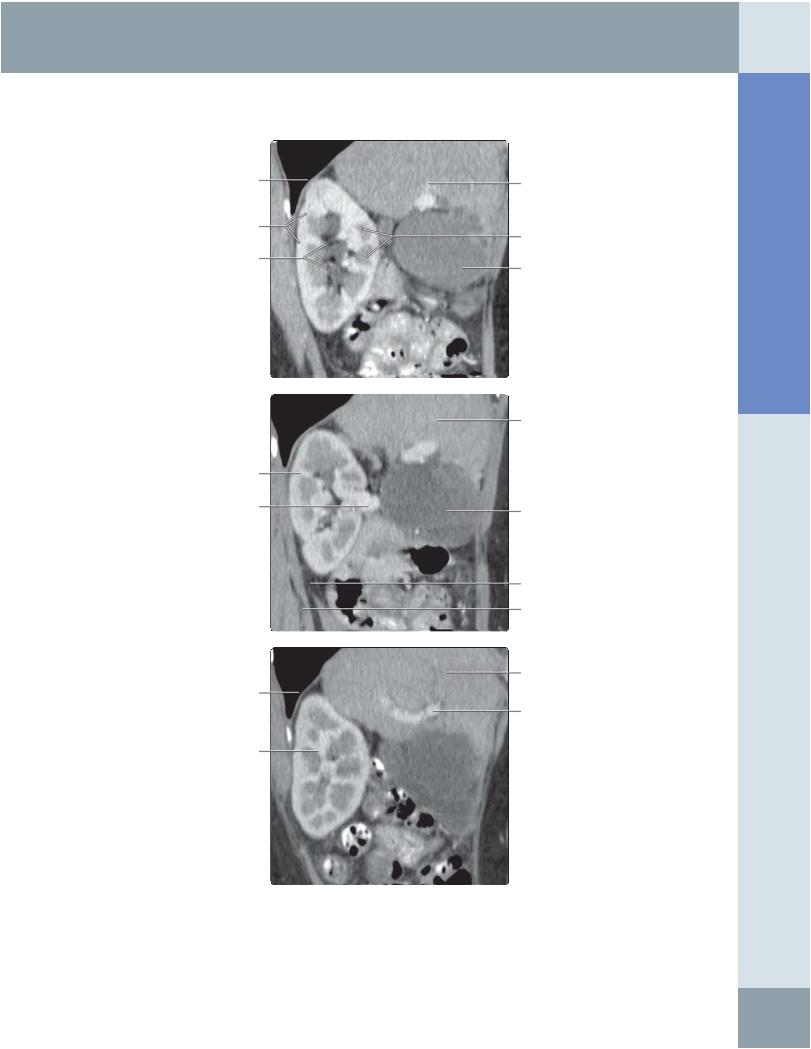
RIGHT KIDNEY, CT CORRELATION
Right lobe of liver
Renal medullary pyramids
Gallbladder
Right lobe of liver
Gallbladder
Perinephric fat
Right psoas muscle
Right lobe of liver
Right portal vein
Abdomen Anatomy:
(Top) Correlative longitudinal CT multiplanar reconstruction image of the right kidney through planes that are commonly used when examining the patient with ultrasound. Like ultrasound, multidetector row CT now allows evaluation of kidneys in many planes; however, ionizing radiation and the use of intravenous contrast are its limiting factors, particularly in children. (Middle) Correlative longitudinal oblique CT multiplanar reconstruction image of the right kidney cutting through the right renal vein is shown. The plane of this image is angulated more medially when compared with the previous image. (Bottom) Correlative longitudinal oblique CT multiplanar reconstruction image of the right kidney cutting through the right portal vein with the plane of this image is angulated more laterally when compared with the previous 2 images.
51
Anatomy: Abdomen
Kidneys
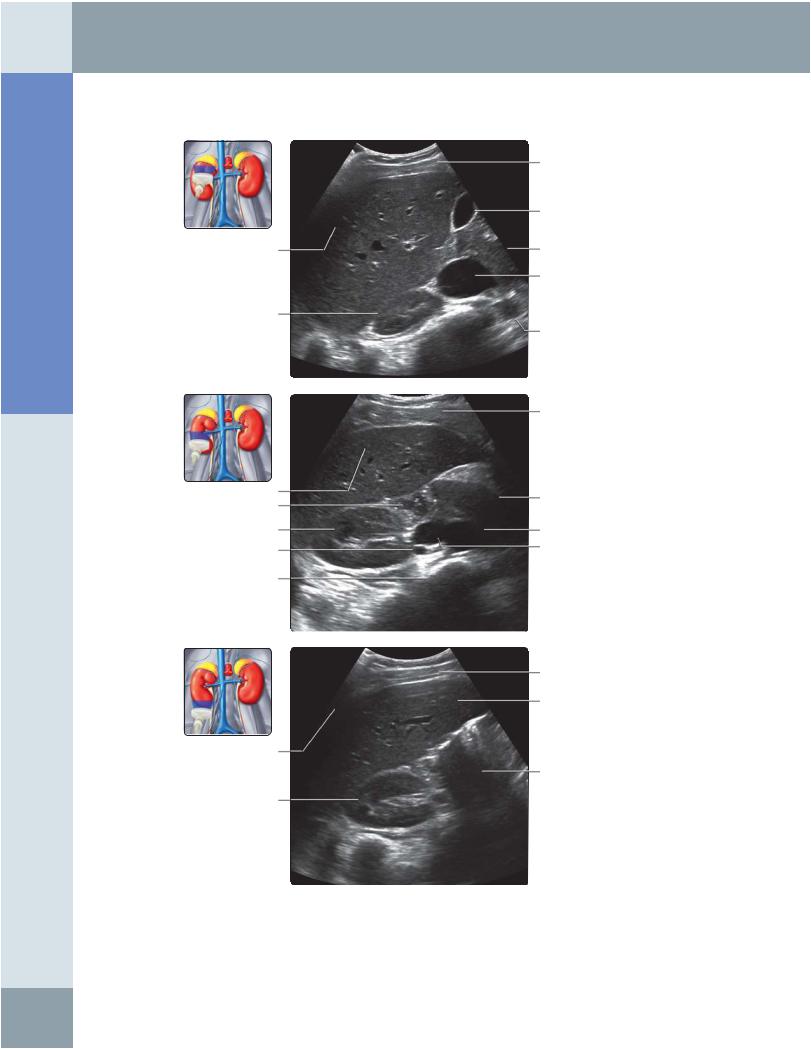
RIGHT KIDNEY, ANTERIOR ABDOMEN SCAN
Right lobe of liver
Right kidney
Right lobe of liver
Duodenum
Pyramid
Right renal artery
Vertebra
Shadowing from rib
Right kidney
Subcutaneous fat
Gallbladder
Head of pancreas
Inferior vena cava
Aorta
Subcutaneous fat
Pancreas
Aorta
Inferior vena cava
Subcutaneous fat
Right lobe of liver
Bowel gas
(Top) Transverse grayscale ultrasound of the upper pole of the right kidney is shown. (Middle) Transverse grayscale ultrasound of the mid pole of the right kidney shows the renal hilum with the renal vein. Note that the pelvicalyceal system within the renal sinus echoes is not usually visible in the normal individual. (Bottom) Transverse grayscale ultrasound of the lower pole of the right kidney. The renal parenchymal echogenicity is less than the adjacent liver or spleen. If the renal parenchyma is brighter than normal liver, renal parenchymal disease should be suspected.
52
Kidneys
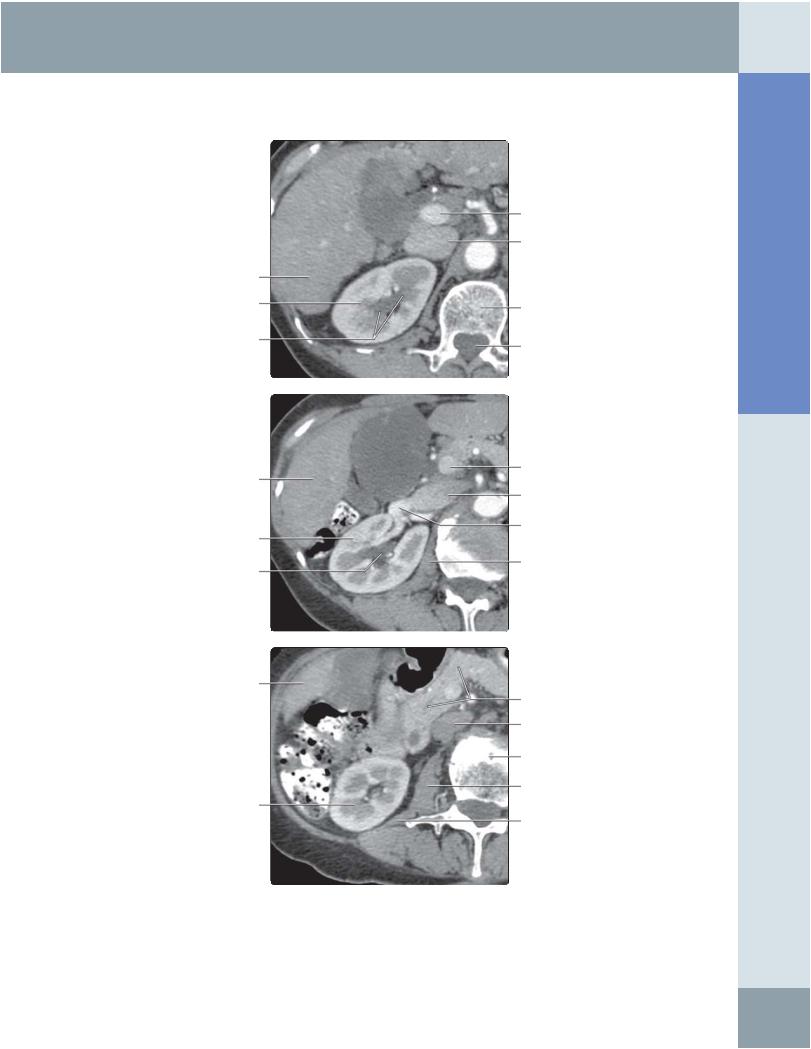
RIGHT KIDNEY, CT CORRELATION
Right lobe of liver
Right kidney
Pelvicalyceal system
Right lobe of liver
Right kidney
Pelvicalyceal system
Right lobe of liver
Right kidney
Portal vein
Inferior vena cava
Vertebral body
Spinal canal
Portal vein
Inferior vena cava
Right renal vein
Right psoas muscle
Pancreas
Inferior vena cava
Vertebral body
Right psoas muscle
Quadratus lumborum
(Top) The 1st in a series of 3 correlative transverse CT images of the right kidney, from the upper pole through the kidney to the lower pole, is shown through planes commonly used when examining the patient with ultrasound. This image shows the upper pole of the right kidney. Multidetector row CT with examination in different phases, following intravenous contrast injection, allows superb differentiation between the renal cortex and medulla. (Middle) Correlative transverse CT of the mid pole of the right kidney shows the renal hilum with the renal vein. (Bottom) Correlative transverse CT image of the lower pole of the right kidney.
Abdomen Anatomy:
53