

новая папка / 80
.pdfAnatomy: Abdomen
Biliary System
RIGHT HEPATIC LOBE
Right hepatic lobe
Middle hepatic vein
Inferior vena cava
Heart
Portal triad
Right kidney
Psoas
Rectus muscle
Gallbladder
Duodenum
Portal vein
Rectus musculature Right hepatic lobe
Portal triad
Gallbladder
Inferior vena cava
Aorta
Spine
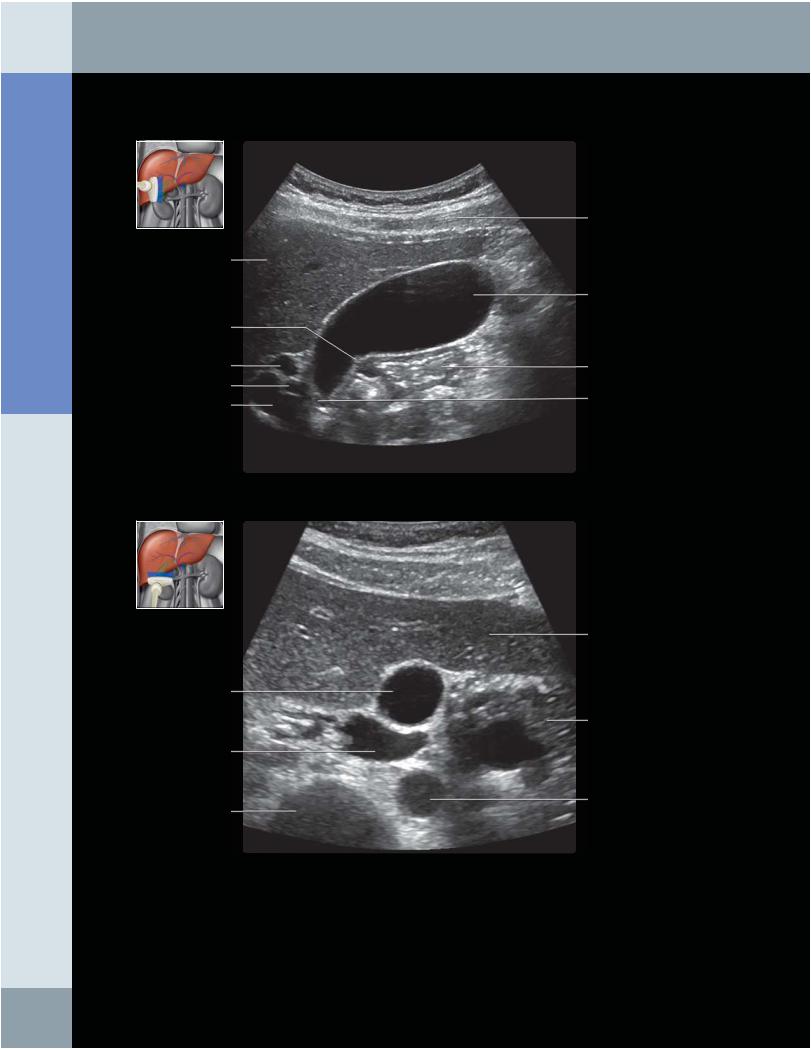
(Top) Subcostal, longitudinal ultrasound shows the right hepatic lobe and gallbladder with patient in the left lateral decubitus position. Ideally, a patient must fast for at least 4 hours to allow for adequate gallbladder distension. (Bottom) Subcostal, transverse ultrasound of the right hepatic lobe demonstrates its anatomical relationships with major vessels and the right kidney. The intrahepatic bile ducts are localized within the portal triads, which are visible by the prominent echogenic walls of the portal veins in these triads. The portal triad contains the portal vein, bile duct, and hepatic artery. Normally, the intrahepatic bile ducts and hepatic arteries are not readily visible unless they are dilated.
24

Biliary System
LEFT HEPATIC LOBE
Right rectus muscle
Inferior vena cava
Rectus musculature
Portal triad
Left hepatic vein
Inferior vena cava
Heart
Portal triad
Portal triad
Left hepatic vein
Left hepatic lobe Portal triad
Gallbladder
Portal vein
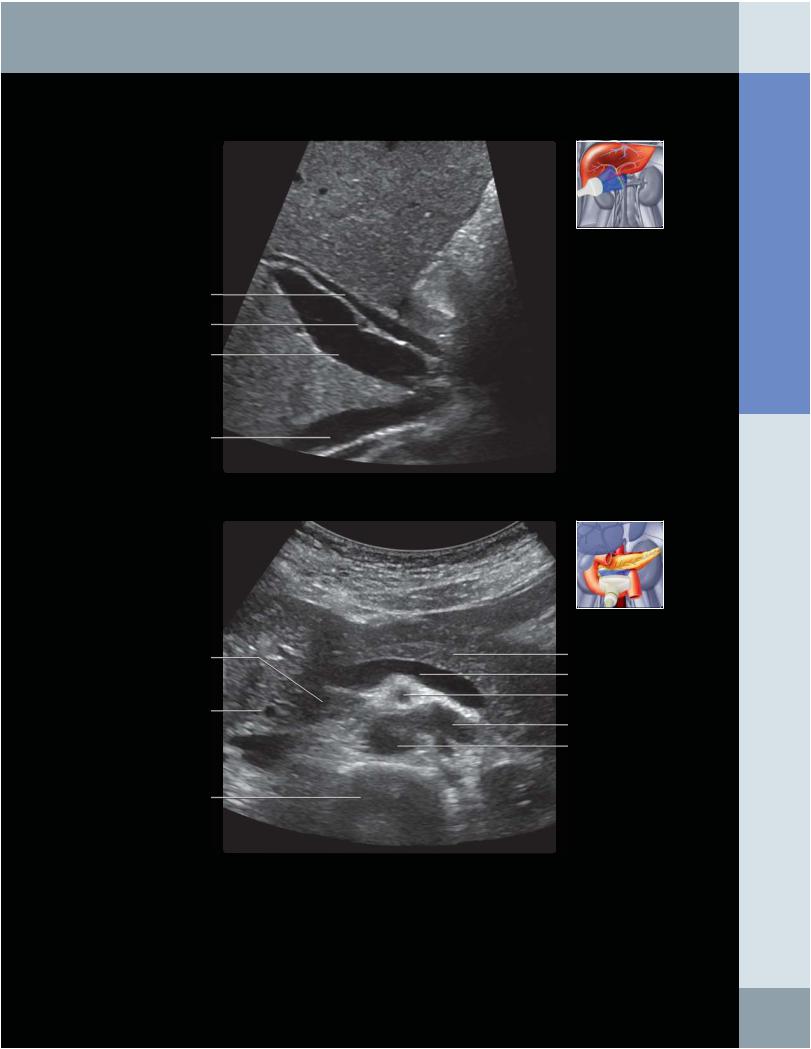
(Top) Subxiphoid, transverse grayscale ultrasound of the left hepatic lobe shows the left hepatic vein and several portal triads. The portal triads are identified by the prominent echogenic walls of the portal veins. The portal triad contains a portal vein, a bile duct, and a hepatic artery. The hepatic artery and bile duct are not readily visible unless they are dilated. (Bottom) Longitudinal ultrasound of the left hepatic lobe near the confluence of the left hepatic vein with the inferior vena cava is shown. Portal triads are recognizable by the prominent walls of the portal veins.
Abdomen Anatomy:
25
Anatomy: Abdomen
Biliary System
GALLBLADDER
Right hepatic lobe
Junctional fold
Common hepatic duct Hepatic artery Main portal vein
Gallbladder
Inferior vena cava
Vertebral body
Right rectus muscle
Gallbladder
Duodenum
Cystic duct
Left hepatic lobe
Stomach
Aorta
(Top) Subcostal, longitudinal grayscale ultrasound shows the gallbladder with patient in the left lateral decubitus position. The gallbladder is distended with bile, causing increased transmission of echoes. A patient must fast for at least 4 hours to allow for adequate gallbladder distension. (Bottom) Transverse ultrasound of a distended gallbladder in left lateral decubitus position is shown. The gallbladder is best evaluated if the patient has fasted at least 4 hours, ideally 8-12 hours.
26
Biliary System
COMMON BILE DUCT
Common bile duct
Hepatic artery
Main portal vein
Inferior vena cava
Abdomen Anatomy:
Head of pancreas |
Body of pancreas |
|
|
|
Splenic vein |
|
Superior mesenteric artery |
Common bile duct |
|
|
Left renal vein |
|
Aorta |
Vertebral body |
|
(Top) Subcostal, longitudinal oblique ultrasound shows the common bile duct and the portal vein in the hepatoduodenal ligament. The common bile duct is normally identified anterior to the portal vein. The distal common bile duct pierces the pancreatic head. Also demonstrated is the hepatic artery, which normally traverses between the portal vein and common bile duct. (Bottom) Transverse ultrasound at the level of the pancreas demonstrates the distal common bile duct as it pierces the pancreatic head. Overlying bowel gas may obscure this area; positioning the patient upright or in a left lateral decubitus position may help visualization.
27
Anatomy: Abdomen
Biliary System
RIGHT INTRAHEPATIC DUCTS
Portal vein
Right hepatic lobe
Intrahepatic duct
Posterior branch of right portal vein
Intrahepatic bile duct
Intrahepatic bile duct
Portal vein Inferior vena cava
Main portal vein
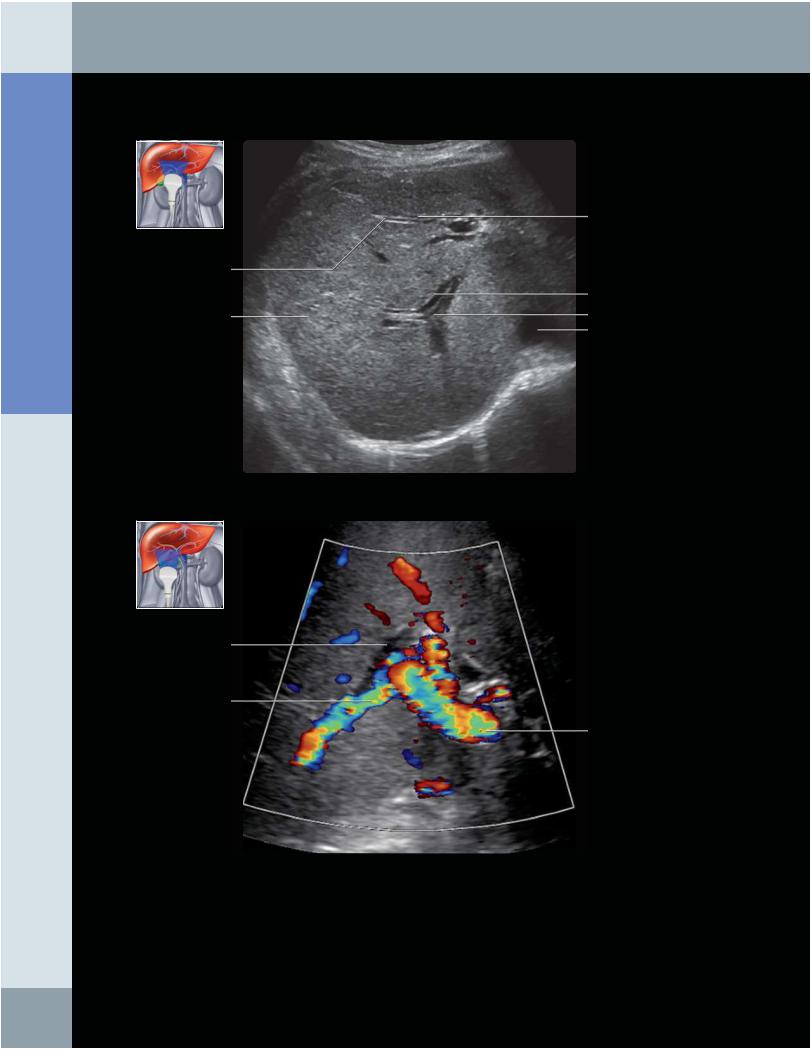
(Top) Transverse ultrasound through the right hepatic lobe in a patient with biliary obstruction demonstrates dilated right intrahepatic bile ducts. Normally, intrahepatic ducts are not readily visualized unless they are dilated. Parallel linear hypoechoic structures are not normally seen in the liver, and this may represent a dilated bile duct or dilated hepatic artery adjacent to the normally visualized portal venous structure in the portal triad. (Bottom) Transverse color Doppler ultrasound through the right hepatic lobe in a patient with biliary obstruction demonstrates dilated right intrahepatic bile ducts. Normally, intrahepatic ducts are not readily visualized unless they are dilated. Color Doppler ultrasound helps to determine whether the dilated structure is a dilated hepatic artery or dilated bile duct.
28
Portal venous branch
Inferior vena cava
Aorta
Portal venous branch
Biliary System
LEFT INTRAHEPATIC DUCTS
Left hepatic lobe
Intrahepatic duct
Left hepatic lobe
Intrahepatic ducts
Abdomen Anatomy:
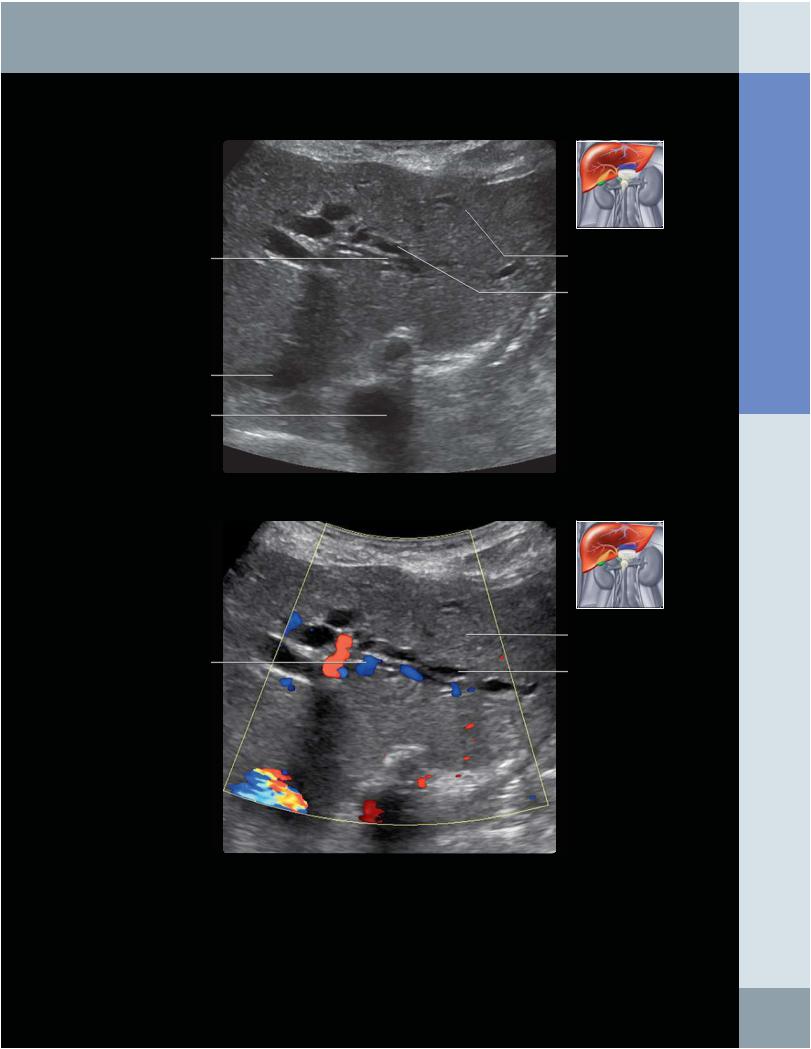
(Top) Transverse ultrasound through the left hepatic lobe in a patient with biliary obstruction demonstrates dilated left intrahepatic bile ducts. Normally, intrahepatic ducts are not readily visualized unless they are dilated. (Bottom) Transverse color Doppler ultrasound through the left hepatic lobe in a patient with biliary obstruction demonstrates dilated left intrahepatic bile ducts. Normally, intrahepatic ducts are not readily visualized unless they are dilated. Color Doppler ultrasound is helpful to determine whether the dilated structure is vascular or biliary, as dilated hepatic arteries can be mistaken for dilated bile ducts. The absence of flow allows one to determine that these are biliary in origin.
29
Anatomy: Abdomen
Spleen
GROSS ANATOMY
Overview
•Spleen is largest lymphatic organ
○Normal size is variable; no universal consensus
–Generally, normal adult spleen considered 12 cm length x 4 cm thickness x 7 cm width
–Length = longest diameter in longitudinal plane; thickness = transverse measurement from hilum; width = longest transverse diameter
–Splenic index (product of length, thickness, and width): Normally 120-480 cm³
–Size correlates with height and can exceed these limits in tall, healthy people
○Functions
–Manufactures lymphocytes, filters blood (removes damaged red blood cells and platelets)
–Acts as blood reservoir: Can expand or contract in response to changes in blood volume
•Histology
○Soft organ with fibroelastic capsule entirely surrounded by peritoneum, except at splenic hilum
○Trabeculae: Extensions of capsule into parenchyma; carry arterial and venous branches
○Pulp: Substance of spleen; white pulp = lymphoid nodules; red pulp = sinusoidal spaces containing blood
○Splenic cords (plates of cells) lie between sinusoids; red pulp veins drain sinusoids
•Relations and vessels
○Spleen contacts posterior surface of stomach and is connected via gastrosplenic ligament (GSL)
–GSL is left anterior margin of lesser sac; carries short gastric and left gastroepiploic arteries and venous branches to spleen
○Contacts pancreatic tail and surface of left kidney and is connected by the splenorenal ligament (SRL)
–SRL is left posterior margin of lesser sac (omental bursa); carries splenic arterial and venous branches to spleen
○Splenic vein runs in groove along dorsal surface of pancreatic bodyand tail
–Receives inferior mesenteric vein (IMV)
–Combined splenic vein and IMV join superior mesenteric vein to form portal vein
○Splenic artery arises from celiac axis in 90%; 8% directly from aorta; often very tortuous
IMAGING ANATOMY
Internal Contents
•Echo pattern
○Homogenous, similar to liver
○Echogenicity: Pancreas > spleen > liver > kidney
•Architecture
○Radiating pattern of segmental arteries and veins
○Splenic vein
–Normal diameter 5-10 mm; peak systolic velocity (PSV): 9-18 cm/s
–Splenic vein at midline is useful landmark for locating pancreas; pancreas lies anterior to splenic vein
–Diameter increases between 50-100% from quiet respiration to deep inspiration; increase of < 20% suggests portal hypertension
–Spectral Doppler waveform typically shows band-like flow profile with minimal respiratory fluctuations
○Splenic artery
–Low-resistance waveform; tortuosity of vessel results in turbulence and spectral broadening
–Normal diameter: 4-8 mm; PSV: 25-45 cm/sec
ANATOMY IMAGING ISSUES
Imaging Recommendations
•Patient positioned supine or right decubitus position (left side up) with left arm raised
•Place transducer parallel to ribs in 10th or 11th intercostal space at left midaxillary line, searching for best window
○Due to rib angle this results in oblique view, which by convention is called longitudinal or transverse (depending on transducer orientation)
○Transverse US view of spleen does not correlate directly to axial CT view
•End expiration may be helpful; lung base may obscure spleen in full inspiration
•Spleen poorly accessed from posterior (obscured by left lung base), anterior, or subcostal approach (obscured by stomach and colon)
•Assess splenic vein at hilum and midline for patency and flow direction
Key Concepts
•Spleen has highly variable size and shape
○Easily indented and displaced by masses and even loculated fluid collections
EMBRYOLOGY
Practical Implications
•Accessory spleen (splenunculus, splenule):Found in 1030% of population
○Usually small, near splenic hilum
○Can enlarge and simulate mass, especially after splenectomy
○Ectopic intrapancreatic splenule can mimic pancreatic tail mass; should not be more than 3 cm from tail tip
•Wandering spleen: Spleen may be on long mesentery; found in any abdominopelvic location; risk of torsion
•Asplenia and polysplenia (heterotaxy syndromes)
○Situs ambiguus; rare congenital conditions of altered left/right orientation of organs; associated with cardiovascular anomalies, intestinal malrotation, etc.
•Splenosis: Peritoneal implantation of splenic tissue after traumatic splenic injury, can mimic polysplenia
SELECTED REFERENCES
1.Benter T et al: Sonography of the spleen. J Ultrasound Med. 30(9):1281-93, 2011
2.Kim SHet al:Intrapancreaticaccessory spleen:findings on MRImaging, CT, US and scintigraphy, pathologicanalysis. Korean J Radiol. 9(2):162-74, 2008
3.Gillen MA: The spleen.InMcGahan JP,Goldberg BB (eds)Diagnostic Ultrasound, 2nd ed, New York, NY: Informa Healthcare:2008: 801-822
4.Applegate KE et al: Situs revisited: Imaging of the heterotaxy syndrome. RadioGraphics 19:837-852, 1999
30
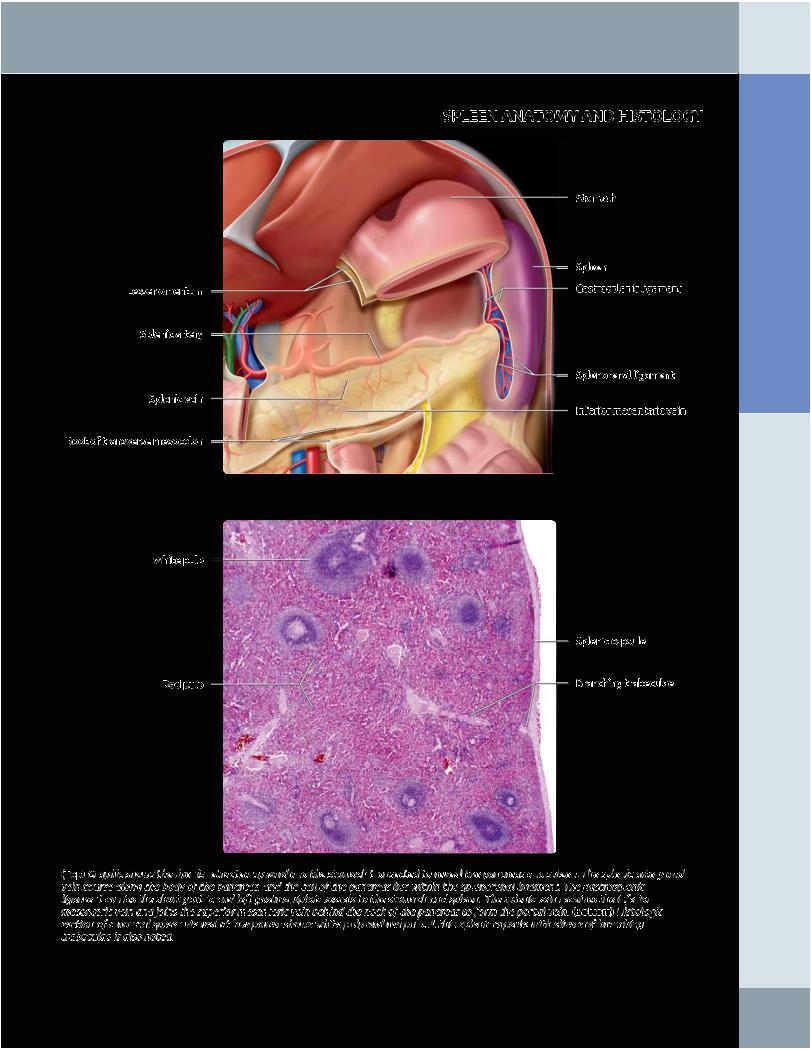
Lesser omentum
Splenic artery
Splenic vein
Root of transverse mesocolon
White pulp
Red pulp
Spleen
SPLEEN ANATOMY AND HISTOLOGY
Stomach
Spleen
Gastrosplenic ligament
Splenorenal ligament
Inferior mesenteric vein
Splenic capsule
Branching trabeculae
(Top) Graphic shows the liver is retracted upward and the stomach transected to reveal the pancreas and spleen. The splenic artery and vein course along the body of the pancreas, and the tail of the pancreas lies within the splenorenal ligament. The gastrosplenic ligament carries the short gastric and left gastroepiploic vessels to the stomach and spleen. The splenic vein receives the inferior mesenteric vein and joins the superior mesenteric vein behind the neck of the pancreas to form the portal vein. (Bottom) Histologic section of a normal spleen viewed at low power shows white pulp and red pulp. A thin splenic capsule with slivers of branching trabeculae is also noted.
Abdomen Anatomy:
31
Anatomy: Abdomen
Spleen
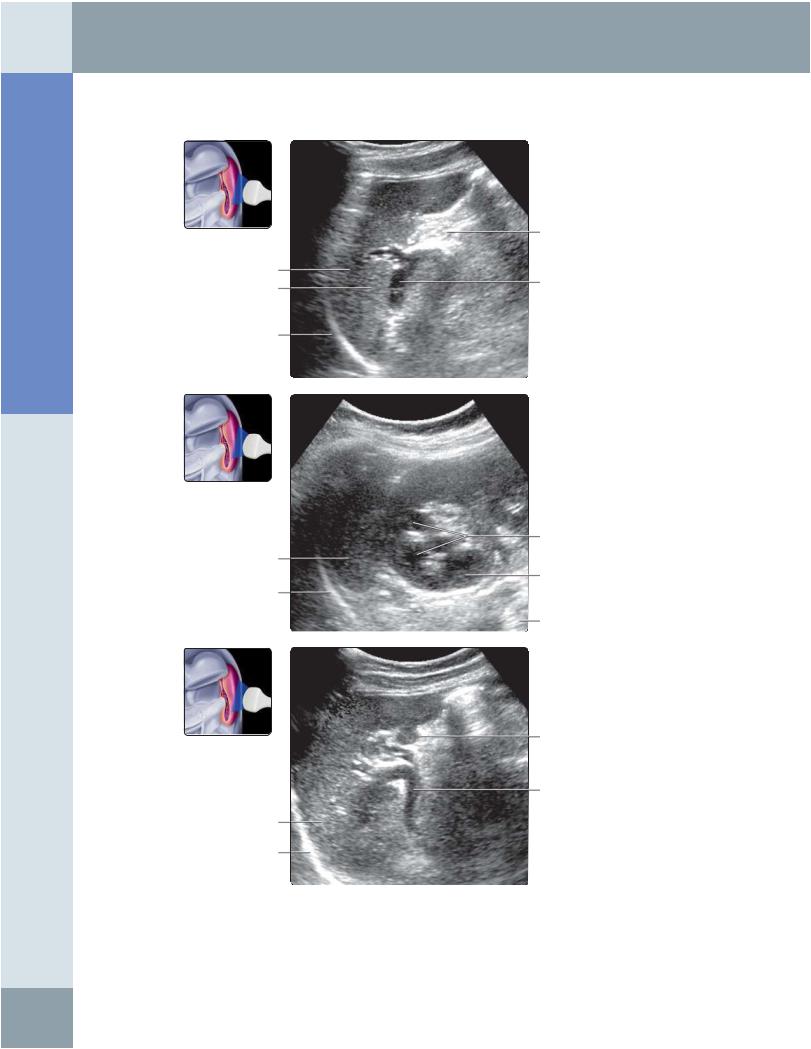
SPLEEN ANATOMY
Spleen Tail of pancreas
Left hemidiaphragm
Spleen
Left hemidiaphragm
Spleen
Left hemidiaphragm
Fat in splenic hilum
Splenic vein
Renal pyramids
Left kidney
Left psoas muscle
Accessory spleen
Splenic vein
(Top) Longitudinal oblique grayscale ultrasound shows the spleen from a posterolateral intercostal approach. The patient is positioned in the right lateral decubitus position with examination during full expiration. Note that the tail of the pancreas can be imaged using the spleen as an acoustic window. (Middle) Longitudinal oblique ultrasound shows the spleen and its relationship to the upper pole of the left kidney with the transducer placed parallel to the intercostal space. (Bottom) Longitudinal oblique grayscale ultrasound of a splenule (accessory spleen) is shown. Splenules are rounded, well-defined masses commonly found (10-30% of population) in or near the splenic hilum. They are homogeneous and isoechoic to the splenic parenchyma.
32
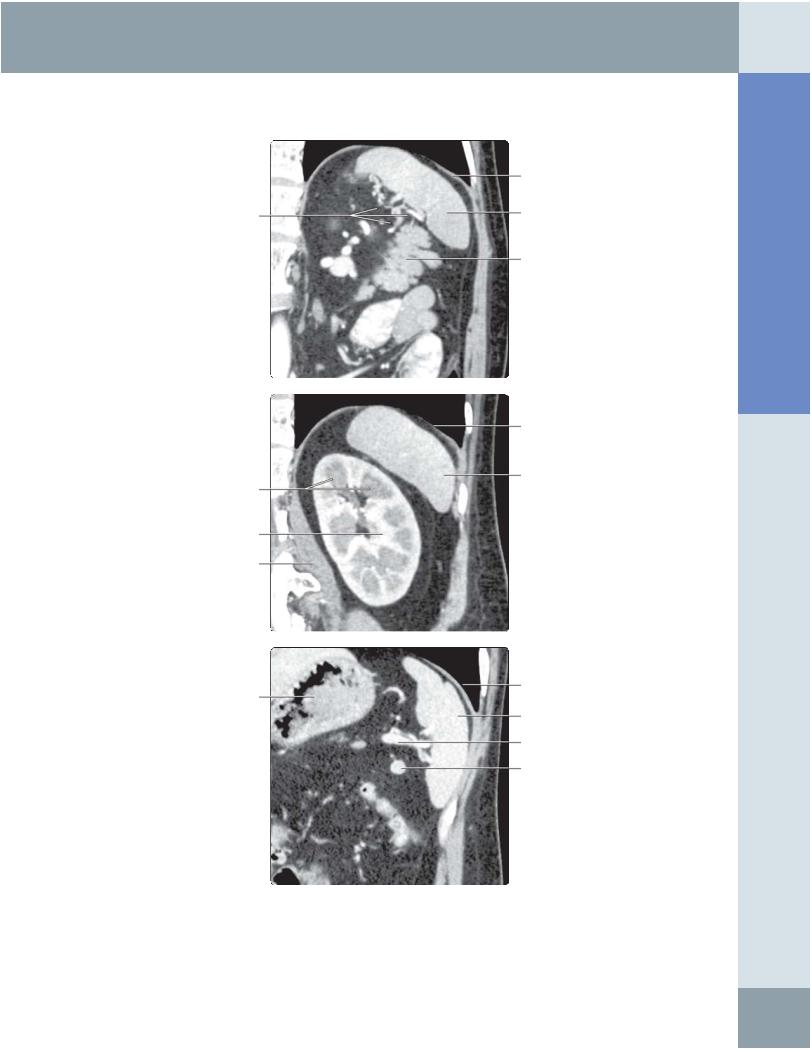
Fat in splenic hilum
Renal pyramids
Left kidney
Left psoas muscle
Stomach
Spleen
CT CORRELATION
Left hemidiaphragm
Spleen
Tail of pancreas
Left hemidiaphragm
Spleen
Left hemidiaphragm
Spleen
Splenic vein
Accessory spleen
Abdomen Anatomy:
(Top) Oblique correlative multiplanar reconstruction CT of the spleen is shown. Note the fat around the splenic hilum and the extension of the pancreatic tail towards the splenic hilum. This allows the pancreatic tail to be visualized by ultrasound using the spleen as an acoustic window. (Middle) Oblique correlative multiplanar reconstruction CT shows the relationship between the spleen and the kidney. (Bottom) Oblique correlative multiplanar reconstruction CT of the accessory spleen in the splenic hilum is shown. The accessory spleen simulates the appearance of a normal spleen on imaging; this identical appearance prevents it from being mistaken for pathology.
33