

новая папка / 80
.pdfAnatomy: Abdomen
Spleen
SPLENIC VESSELS
Pancreas
Left renal vein
Inferior vena cava
Left renal vein
Common hepatic artery Portal vein
Inferior vena cava
Left hepatic lobe
Splenic vein
Superior mesenteric artery (SMA)
Aorta
Splenic vein
Superior mesenteric artery
Aorta
Left hepatic lobe
Splenic artery
Splenic vein
Celiac artery
Abdominal aorta
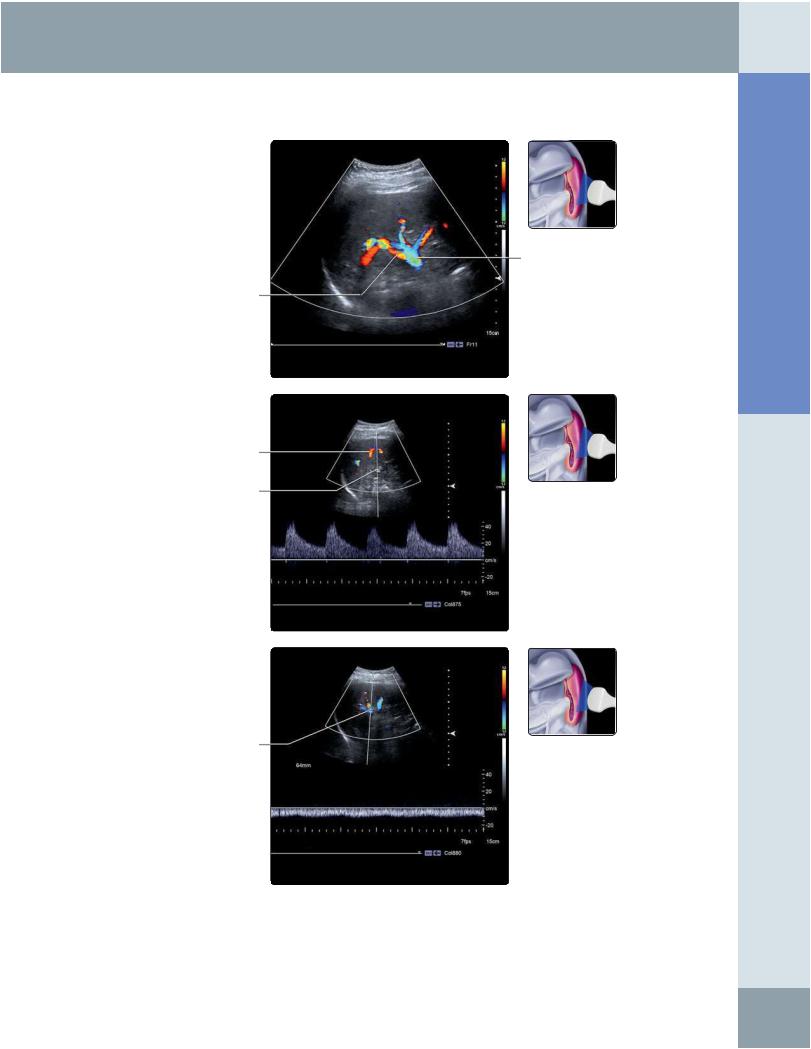
(Top) Midline transverse anterior grayscale ultrasound of the splenic vein is shown. The splenic vein is located deep to the pancreatic body. Note the left renal vein course between the SMA and aorta. (Middle) Color Doppler of the same area shows the normal direction of flow in the splenic vein, towards the liver (hepatopetal). Note the change in color from red to blue, which is due to the position of the transducer, aligned at the midpoint of the vein. Using the information provided by the color bar, the red portion of the splenic vein is blood flowing towards the transducer (away from the spleen), and the blue is blood flowing away from the transducer (towards the the liver). (Bottom) Power Doppler of the upper abdomen at midline shows the origin of the splenic artery from the celiac axis. The celiac artery branches into the splenic artery, common hepatic artery, and left gastric artery (not shown). After its takeoff, the splenic artery typically has a tortuous course. The branching of the celiac axis, as shown in this image, has been referred to as the "seagull" sign.
34
Spleen
SPLENIC VESSELS
Splenic vein
Splenic artery
Segmental arterial branches
Splenic artery
Splenic vein
Abdomen Anatomy:
(Top) Longitudinal oblique color Doppler ultrasound demonstrates the branching of the splenic arteries and veins in the splenic hilum. (Middle) Spectral Doppler waveform of the distal splenic artery at the splenic hilum is shown. Because of a tortuous course, flow in this vessel is typically turbulent. The splenic artery has a low-resistance waveform (ample flow throughout diastole). Normal peak systolic velocity for the splenic artery is 25-45 cm/sec. (Bottom) Spectral Doppler waveform ultrasound of the splenic vein at the hilum shows a typical band-like flow profile with minimal respiratory fluctuations; flow is directed away from the transducer (away from the spleen). Normal peak systolic velocity of the splenic vein is 9-18 cm/sec.
35
Anatomy: Abdomen
Spleen
ANATOMICAL VARIANTS
Splenule
Accessory splenic vessels supplying splenule
Stomach
Splenic artery
Splenic vein
Pancreas
Left kidney
Splenic cyst
Heart
Spleen in right upper quadrant
Spleen
Spleen
Accessory vessels supplying splenule
Splenule
Right diaphragm
Ascites
Right kidney
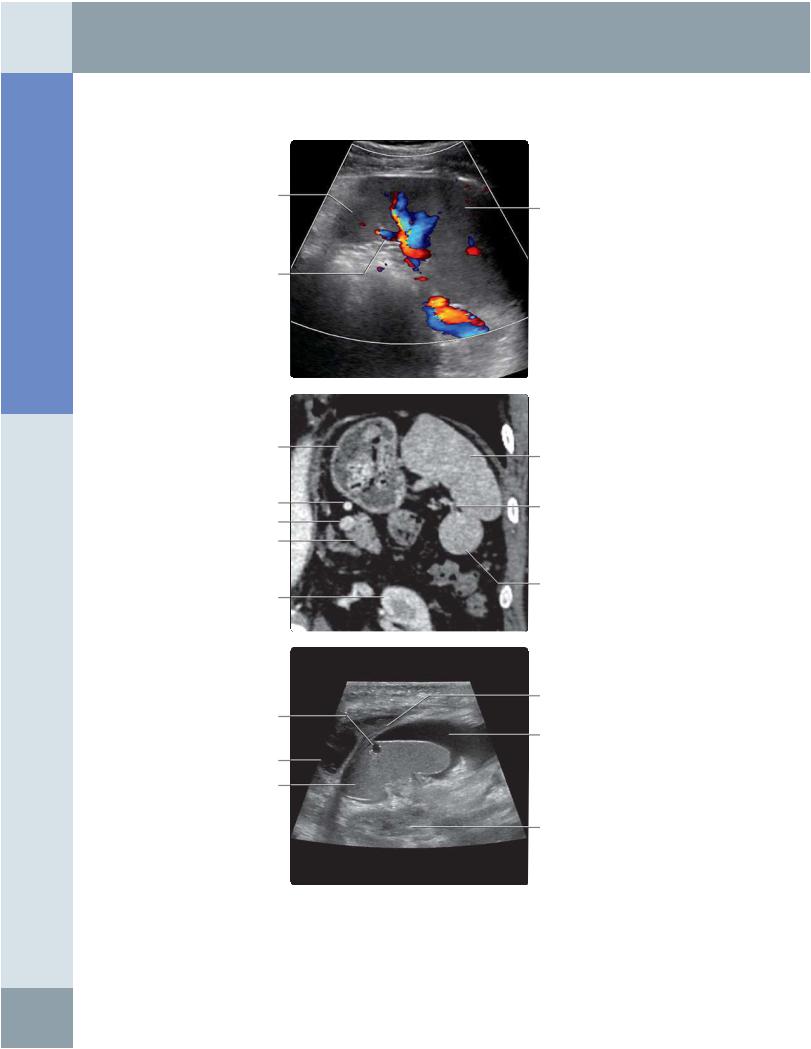
(Top) Longitudinal oblique intercostal color Doppler ultrasound shows a splenule adjacent to the spleen tip. Splenules should have the same echogenicity and echotexture as the spleen, though this may depend on the sonographic window. The identification of vascular supply from the splenic vessels may also aid in identification of a splenule. (Middle) Correlative coronal CECT of the left upper quadrant demonstrates a splenule along the inferior tip of the spleen. Branch vessels from the splenic artery and vein supplying the splenule are visualized. (Bottom) Longitudinal oblique ultrasound of the right upper quadrant in a patient with heterotaxy syndrome (situs ambiguus) demonstrates a right-sided spleen. The classification of heterotaxy syndromes is complex; there is a spectrum ranging from classic asplenia to classic polysplenia. Heterotaxy with polysplenia (i.e., left double-sidedness or left isomerism) may present with multiple spleens (resembling splenules) or a single spleen, as in this case.
36
Spleen
ANATOMICAL VARIANTS
Intercostal muscle
Splenosis
Left kidney
Pancreatic tail
Superior pole of left kidney
Splenosis
Ascites
Splenic cyst
Left-sided liver
Right-sided spleen
Abdomen Anatomy:
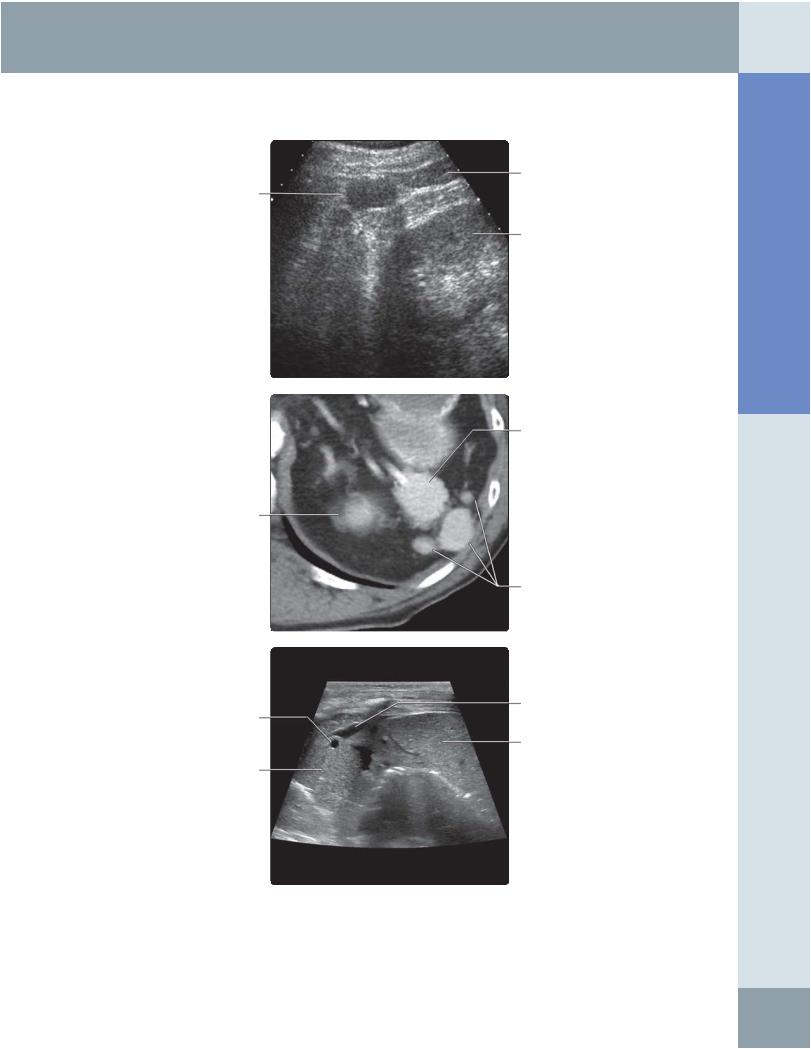
(Top) Longitudinal oblique intercostal grayscale ultrasound through the left upper quadrant shows a round hypoechoic structure adjacent to the upper pole of the left kidney; this represents splenosis. (Middle) Correlative axial CECT through the left upper quadrant in a patient with prior splenic trauma and splenectomy shows residual splenosis. (Bottom) Transverse anterior ultrasound in the setting of heterotaxy with polysplenia demonstrates the relationship between the right-sided spleen and the left-sided liver.
37

Anatomy: Abdomen
Pancreas
GROSS ANATOMY
Overview
•Pancreas: Accessory digestive gland lying in retroperitoneum behind stomach
○Exocrine function: Pancreatic acinar cells secrete pancreatic juice → pancreatic duct → duodenum
○Endocrine: Pancreatic islet cells (of Langerhans) secrete insulin, glucagon, and other polypeptides → portal venous system
Divisions
•Head: Thickest part; lies to right of superior mesenteric artery and vein (SMA, SMV)
○Attached to "C" loop of duodenum (2nd & 3rd parts)
○Uncinate process: Head extension, posterior to SMV
○Bile duct lies along posterior surface of head, joins with pancreatic duct (of Wirsung) to form hepatopancreatic ampulla (of Vater)
○Main pancreatic and bile ducts empty into major papilla in 2nd portion of duodenum
•Neck: Thinnest part; lies anterior to SMA, SMV
○SMV joins splenic vein behind pancreatic neck to form portal vein
•Body: Main part; lies to left of SMA, SMV
○Splenic vein lies in groove on posterior surface of body
○Anterior surface is covered with peritoneum forming back surface of omental bursa (lesser sac)
•Tail: Lies betweenlayers of splenorenal ligament in splenic hilum
Internal Structures
•Pancreatic duct (of Wirsung) runs length of pancreas, turning inferiorly through head to join bile duct
•Accessory pancreatic duct (of Santorini) opens into duodenum at minor duodenal papilla
○Usually communicates with main pancreatic duct
○Variations are common, including a dominant accessory duct draining most pancreatic juice
•Vessels, nerves, and lymphatics
○Arteries to head mainly from gastroduodenal artery
–Pancreaticoduodenal arcade of vessels around head also supplied by SMA branches
○Arteries to body & tail from splenic artery
○Veins are tributaries of SMV and splenic vein → portal vein
○Autonomic nerves from celiac and superior mesenteric plexus
–Parasympathetic stimulation of pancreatic secretion, but pancreatic juice secretion is mostly under hormonal control (secretin, from duodenum)
○Lymphatics follow blood vessels
–Collect in splenic, celiac, superior mesenteric and hepatic nodes
IMAGING ANATOMY
Overview
•Pancreas can be localized on ultrasound by
○Typical parenchymal architecture: Homogeneously isoechoic/hyperechoic echo pattern when compared with overlying liver
○Surrounding anatomical landmarks: Body anterior to splenic vein; neck anterior to SMA/SMV
•Variations in reflectivity related to degree of fatty infiltration; uncinate process and posterior pancreatic head are relatively echo-poor in 25% of subjects (lack of intraparenchymal fat)
ANATOMY IMAGING ISSUES
Imaging Recommendations
•Use 2-5 MHz transducers, or up to 9 MHz for smaller patients
•Techniques to combat overlying stomach and bowel gas include
○Displacement of intervening bowel gas by gentle firm graded compression with transducer
○Overnight fasting or fasting > 6-8 hours
○Non-effervescent fluid can be given orally to fill gastric fundus
–Scanning delayed for a few minutes to allow fluid to settle
–Patient can lie on left side to allow imaging of body and tail of pancreas
–Patient can then be turned right to allow gastric fluid to flow to stomach antrumand duodenum, allowing imaging of head and uncinate process
•CT is preferred imaging modality for imaging of pancreas
•MRCP or ERCP useful for defining pancreatic duct
Imaging Pitfalls
•Ultrasound examination of pancreas is often limited by overlying bowel gas
Key Concepts
•Shape, size, and texture of pancreas are quite variable
○Largest in young adults
○Atrophy and fatty infiltration with age (> 70), obesity, diabetes, corticosteroids, Cushing disease
○Pancreatic duct also becomes more prominent with age (normal < 3 mm diameter)
○Focal bulge or mass effect is abnormal
•Location behind lesser sac
○Acute pancreatitis often results in lesser sac fluid (may mimic pseudocyst)
•Pancreas lies in anterior pararenal space (APS)
○Inflammation (from pancreatitis) easily spreads to duodenum and descending colon; also lie in APS
○Inflammation easily spreads into mesentery and mesocolon; roots of these lie just ventral to pancreas
•Obstruction of pancreatic duct
○Relatively common result of chronic pancreatitis (fibrosis &/or stone occluding pancreatic duct), or pancreatic ductal carcinoma
•Acute pancreatitis
○Relatively common result of gallstone (lodged in hepatopancreatic ampulla causing bile to reflux into pancreas) or damage from alcohol abuse
38
Gastroduodenal artery
Posterior superior pancreaticoduodenal artery
Anterior superior pancreaticoduodenal artery
Base of transverse mesocolon
Duodenum
Pancreas
PANCREAS IN SITU
Stomach (cut & removed)
Spleen
Superior (dorsal) pancreatic artery
Splenic artery
Great pancreatic artery
Transverse colon
Duodeno-jejunal junction
Superior mesenteric artery & vein
Base of small bowel mesentery
Abdomen Anatomy:
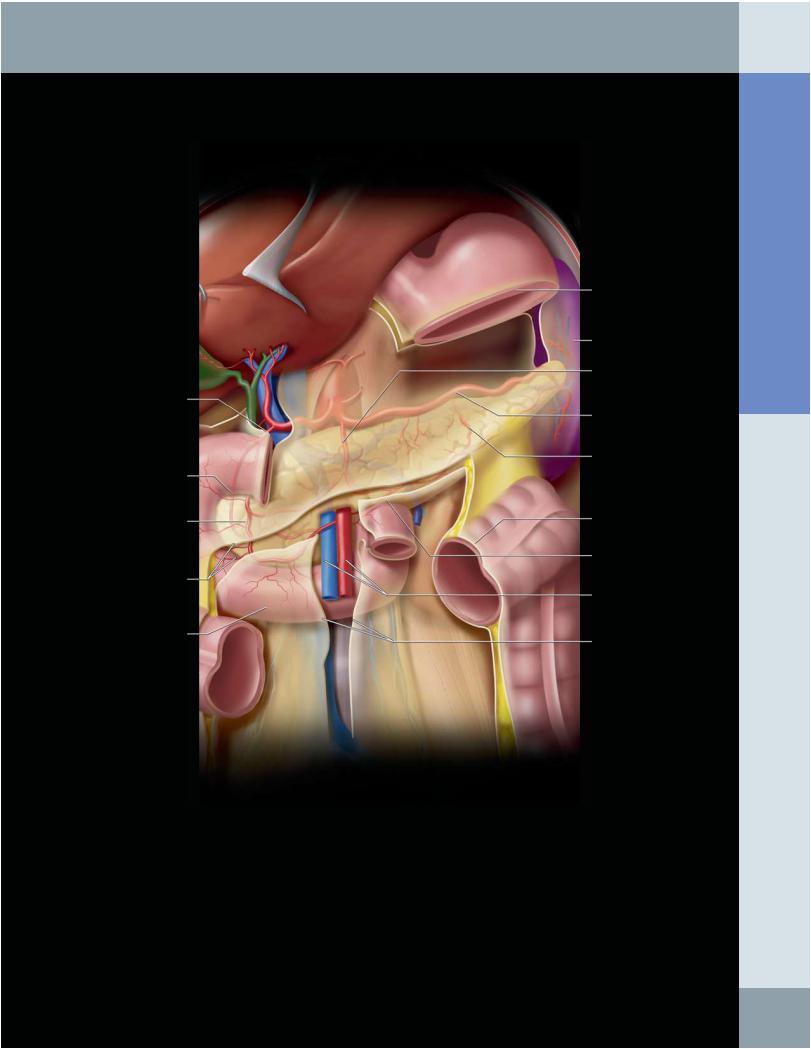
Graphic shows the arterial supply to the body & tail of the pancreas through terminal branches of the splenic artery, which are variable in number & size. The two largest are usually the dorsal (superior) and great pancreatic arteries, which arise from the proximal & distal splenic artery, respectively. The arteries to the pancreatic head and duodenum come from the pancreaticoduodenal arcades that receive flow from the celiac and superior mesenteric arteries. The superior mesenteric vessels pass behind the neck of the pancreas and in front of the third portion of the duodenum. The root of the transverse mesocolon and small bowel mesentery arise from the surface of the pancreas and transmit the blood vessels to the small bowel & transverse colon. The splenic vein runs along the dorsal surface of the pancreas. The splenic vessels and pancreatic tail insert into the splenic hilum.
39
Anatomy: Abdomen
Pancreas
PANCREAS, TRANSVERSE VIEW
Head of pancreas
Gallbladder
Inferior vena cava
Head of pancreas
Inferior vena cava
Aorta
Head of pancreas
Inferior vena cava Uncinate process Abdominal aorta
Body of pancreas
Tail of pancreas
Splenic vein
Superior mesenteric artery
Aorta
Stomach (with fluid)
Body of pancreas Superior mesenteric artery Splenic vein
Tail of pancreas
Left renal artery
Left lobe of liver
Body of pancreas
Superior mesenteric artery
Tail of pancreas
Splenic vein
Left kidney
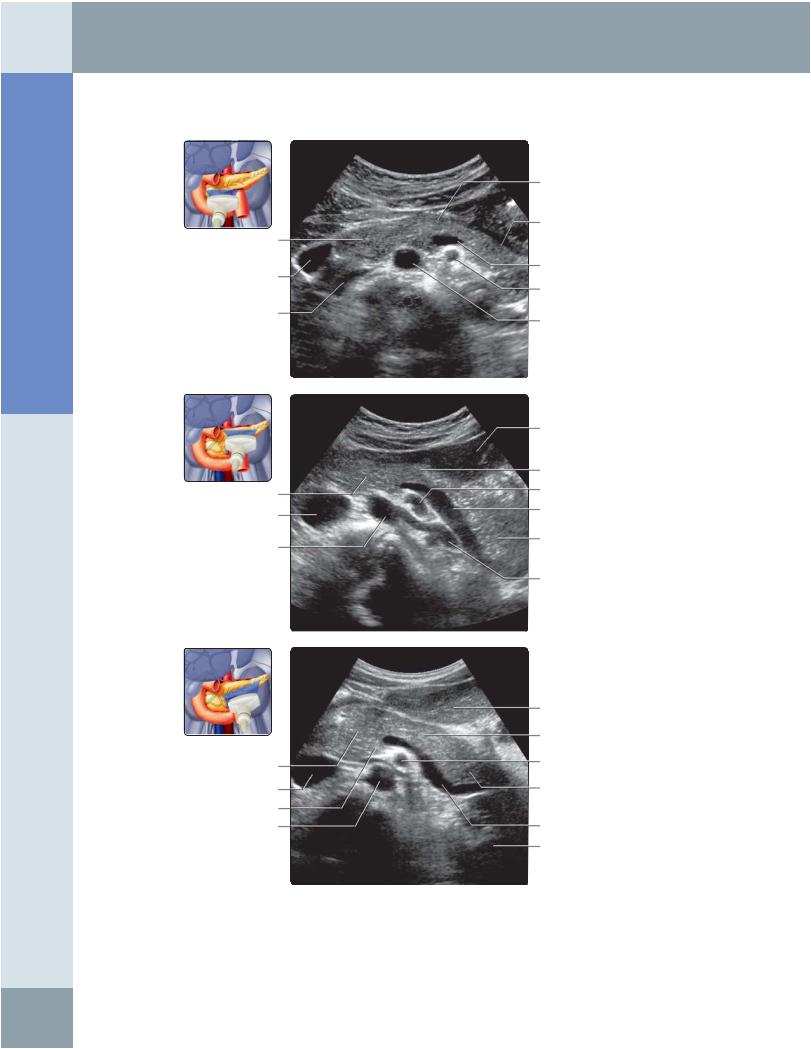
(Top) Transverse transabdominal grayscale ultrasound at the epigastrium is shown. Anatomically, the pancreatic axis from head to tail is directed superiorly and to the left. This lower transverse section demonstrates the bulk of the pancreatic head. (Middle) Transverse transabdominal grayscale ultrasound at the epigastrium is shown, slightly higher than the previous image. Note that the pancreatic body and tail have now come into view. (Bottom) Oblique transabdominal grayscale ultrasound at the epigastrium is shown. The transducer is tilted slightly cranially and laterally to the left to follow the pancreatic axis, thus imaging the pancreas in its entirety. The splenic vein courses along the posterior pancreas and provides an excellent landmark in locating the pancreas. The superior mesenteric artery is more posteriorly located and has a characteristic dot shape as it is imaged end-on.
40
Pancreas
PANCREAS, TRANSVERSE VIEW
Inferior vena cava
Aorta
Inferior vena cava Aorta
Inferior vena cava Aorta
Pancreas
Splenic vein
Superior mesenteric artery
Left renal artery
Pancreas
Superior mesenteric artery
Splenic vein
Superior mesenteric artery
Left renal artery
Splenic vein
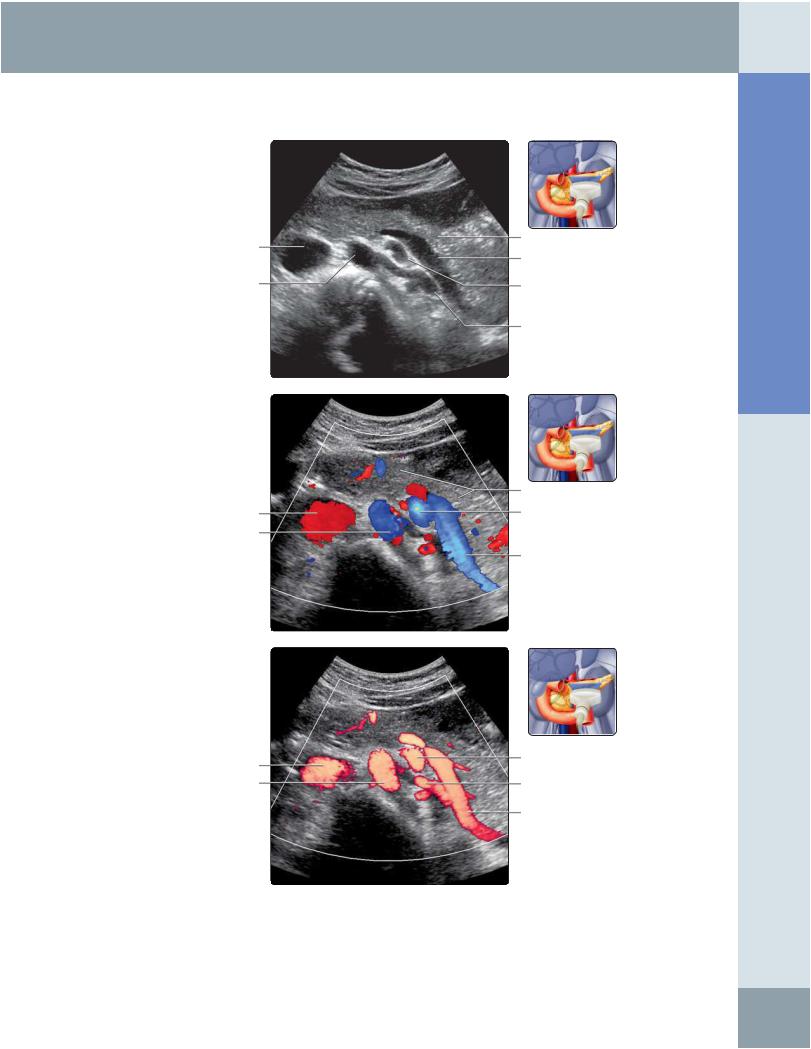
(Top) Transverse subxiphoid grayscale ultrasound shows the left renal artery coursing posterior to the superior mesenteric artery and splenic vein as it descends to enter the left renal hilum. (Middle) Transverse subxiphoid color Doppler ultrasound is shown. This image was taken with a small amount of cranial tilt so that blue indicates flow toward the transducer and red away from the transducer. Note therefore that aortic flow is blue and IVC flow is red. The splenic vein is red in its proximal portion but exhibits blue color distally, owing to its course. The left renal artery is almost at right angles to the transducer and therefore flow is not well seen. (Bottom) Transverse subxiphoid power Doppler ultrasound demonstrates the vessels posterior to the pancreas. Power Doppler is more sensitive for detecting vascular flow but fails to provide information on flow direction.
Abdomen Anatomy:
41
Anatomy: Abdomen
Pancreas
PANCREAS, SAGITTAL VIEW
Gas within duodenum
Left lobe of liver
Left lobe of liver
Celiac trunk
Abdominal aorta
Right rectus muscle
Head of pancreas
Inferior vena cava
Right psoas muscle
Air within gastroduodenal region
Neck of pancreas Superior mesenteric vein
Inferior vena cava
Neck of pancreas
Superior mesenteric vein
Superior mesenteric artery
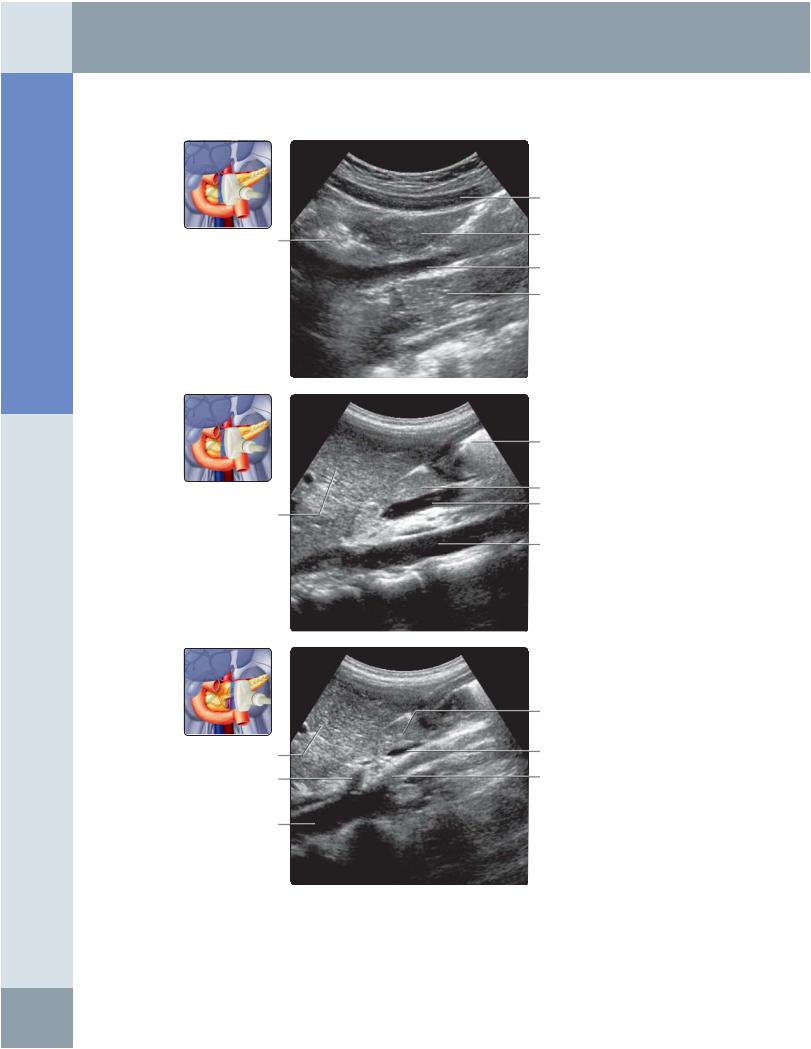
(Top) Longitudinal transabdominal grayscale ultrasound at the epigastrium, right paramedian region, is shown. Note the relationship of the pancreatic head with the posteriorly located inferior vena cava. (Middle) Longitudinal transabdominal grayscale ultrasound at the epigastrium, right paramedian region, is shown continuing medially from the previous image. Note the superior mesenteric vein coming into view; this is a good landmark for locating the neck of the pancreas on the sagittal ultrasound. (Bottom) Longitudinal transabdominal grayscale ultrasound at the epigastrium, right paramedian region, is shown slightly more medial to the previous image. The origin of the superior mesenteric artery arising from the abdominal aorta is brought into view. The SMA is also a useful marker for identifying the neck of the pancreas on sagittal ultrasound.
42
Pancreas
PANCREAS, SAGITTAL VIEW
Left lobe of liver
Superior mesenteric vein
Abdominal aorta
Stomach (with fluid)
Left adrenal gland
Left renal artery
Spleen
Splenic artery
Neck of pancreas
Splenic vein
Superior mesenteric artery
Body of pancreas
Splenic vein
Splenic artery
Left renal vein
Tail of pancreas
Splenic vein
Left kidney
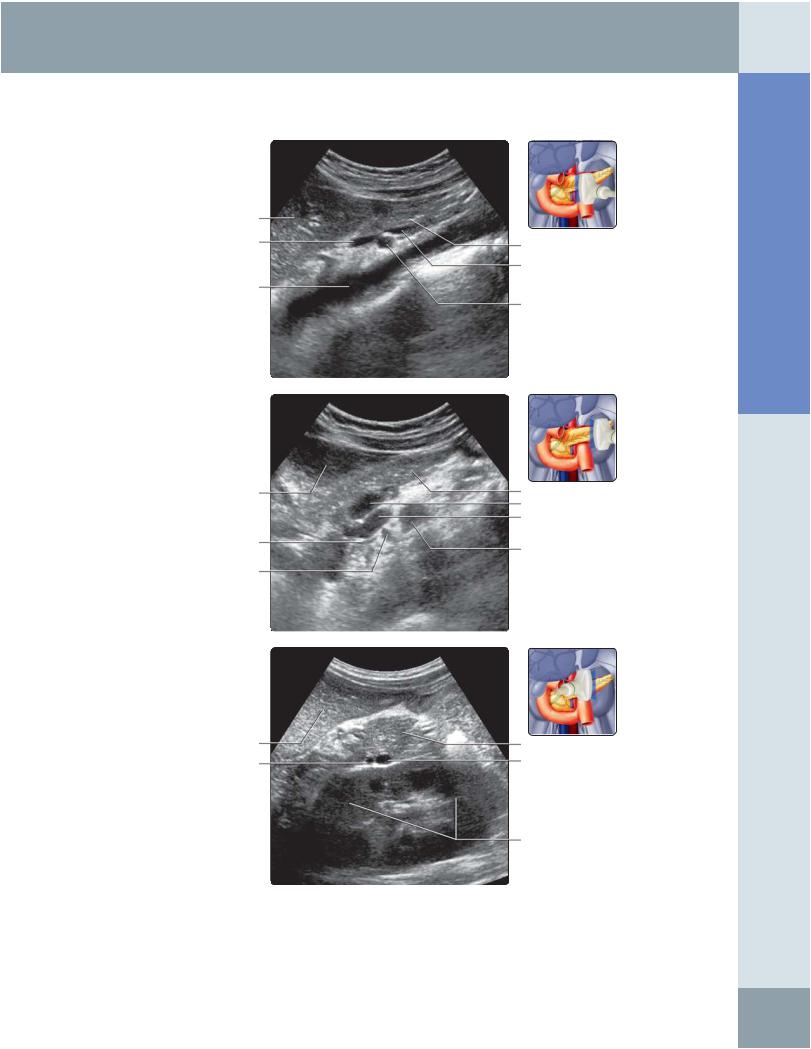
(Top) Longitudinal transabdominal grayscale ultrasound at the midline epigastrium is shown, revealing the SMA that has taken off from the abdominal aorta, its relationship with the splenic vein, and the anteriorly located pancreatic neck. The inferior mesenteric vein joins the splenic vein here. (Middle) Longitudinal transabdominal grayscale ultrasound at the epigastrium, left paramedian region, is shown by sweeping the transducer laterally from the top image. The body of the pancreas lies to the left of the SMA (not shown). The stomach lies superiorly and may be filled with fluid for use as an acoustic window. The splenic vein maintains its course behind the pancreas. (Bottom) Longitudinal transabdominal grayscale ultrasound at the epigastrium is shown, continuing the scan laterally from the middle image. The pancreatic tail is identified between the spleen and the left kidney.
Abdomen Anatomy:
43