

новая папка / 80
.pdfAnatomy: Abdomen
Liver
GROSS ANATOMY
Overview
•Liver is largest gland and largest internal organ (average weight: 1,500 grams)
○Functions
–Processes all nutrients (except fats) absorbed from GI tract; conveyed via portal vein
–Stores glycogen, secretes bile
○Relations
–Anterior and superior surfaces are smooth and convex
–Posterior and inferior surfaces are indented by colon, stomach, right kidney, duodenum, inferior vena cava (IVC), gallbladder
○Covered by peritoneum 
– Nonperitoneal posterior superior surface
Nonperitoneal posterior superior surface
–Porta hepatis: Portal vein, hepaticartery, and bile duct are located within hepatoduodenal ligament
○  Extends from liver to anterior abdominal wall
Extends from liver to anterior abdominal wall
– Separates right and left 

– 
–Carries  (ligamentum teres),
(ligamentum teres), 
○Ligamentum  Remnant of ductus venosus
Remnant of ductus venosus
–
•Vascular anatomy (unique dual afferent blood supply)
○Portal vein
–Carries  from gut and
from gut and 
 from pancreas to liver along with oxygen (contains 40% more oxygen than systemic venous blood)
from pancreas to liver along with oxygen (contains 40% more oxygen than systemic venous blood)
–  to liver ○ Hepatic artery
to liver ○ Hepatic artery
– Supplies 20-25% of blood
– 
–Variations are common, including arteries arising from
○Hepatic veins
–Usually 3 (right, middle, and left)
–Many variations and accessory veins
–Collect blood from liver and return it to IVC at confluence of hepatic veins just 
○
–At all levels of size and subdivision, branches of hepatic artery, portal vein, and bile ducts travel together
–Blood flows into  from
from 
 of hepatic artery and portal vein →
of hepatic artery and portal vein →  (detoxify blood and produce bile) → bile collects into ducts, blood collects into central veins → hepatic veins
(detoxify blood and produce bile) → bile collects into ducts, blood collects into central veins → hepatic veins
•Segmental anatomy of liver
–Each receives secondary or tertiary branch of hepatic artery and portal vein
–Each is drained by its own bile duct (intrahepatic) and hepatic vein branch
○Caudate lobe = 
–Has 

○Left lobe
–Lateral superior = segment 2
– 
○Right lobe
–Anterior inferior = segment 5
–Posterior inferior = segment 6
–Posterior superior = segment 7
–Anterior superior = segment 8
IMAGING ANATOMY
Internal Contents
•Capsule
○  well defined
well defined
•
○ Contains segments 2, 3, 4A, and 4B ○ 
– 
○ 
– 
○Liver parenchyma echoes are 
•Right lobe
○Contains segments 5, 6, 7, and 8
○Liver parenchymal echoes similar to left lobe
○Sections of right lobe show same basic shape, though right lobe is usually larger than left
•Caudate lobe
○Longitudinal scan
–Almond-shaped structure posterior to left lobe
○Transverse scan
–Seen as extension of right lobe
•Portal veins
○Have thicker reflective walls than hepatic veins; portal veins have fibromuscular walls
○Wall reflectivity also depends on angle of interrogation; portal veins cut at more oblique angle may have less apparent wall
○Can be traced back towards porta hepatis
○Normal portal flow is hepatopetal on color Doppler; absent or reversal of flow may be seen in portal hypertension
○Normal velocity 13-55 cm/s
○Portal waveform has undulating appearance due to variations with cardiac activity and respiration
○Branches run in transverse plane
○Hepatic portal vein anatomy is variable
•Hepatic veins
4
Liver
○Appear as echolucent defects within liver parenchyma with no reflective wall: Large sinusoids with thin or absent wall
○Branches enlarge and can be traced towards IVC
○Flow pattern has a triphasic waveform
–Resulting from transmission of right atrial pulsations into veins
□A wave: Atrial contraction
□S wave: Systole (tricuspid valve moves toward apex)
□D wave: Diastole
○Right hepatic vein
–Runs in coronal plane between anterior and posterior segments of right hepatic lobe
○Middle hepatic vein
–Lies in sagittal or parasagittal plane between right and left hepatic lobe
○Left hepatic vein
–Runs between medial and lateral segments of left hepatic lobe
–Frequently duplicated
○1 of 3 major branches of hepatic veins may be absent
–Absent right hepatic vein ~ 6%
–Less commonly middle and left hepatic vein
•Hepatic artery
○Flow pattern has low-resistance characteristics with large amount of continuous forward flow throughout diastole
–Normal velocity 30-70 cm/s
–Resistive index ranges 0.5-0.8, increases after meal
○Common hepatic artery usually arises from celiac axis
○Classic configuration: 72%
–Celiac axis → common hepatic artery → gastroduodenal artery and proper hepatic artery → latter gives rise to right and left hepatic artery
○Variations from classic configuration
–Common hepatic artery arising from SMA (replaced hepatic artery): 4%
–Right hepatic artery arising from SMA (replaced right hepatic artery): 11%
–Left hepatic artery arising from left gastric artery (replaced left hepatic artery): 10%
•Bile ducts
○Normal peripheral intrahepatic bile ducts are too small to be demonstrated
○Normal right and left hepatic ducts measuring a few millimeters are usually visible
○Normal common duct
–Most visible in its proximal portion just caudal to porta hepatis: Less than 5 mm
–Distal common duct should typically measure < 6-7 mm
–In elderly, generalized loss of tissue elasticity with advancing age leads to increase in bile duct diameter: < 8 mm (somewhat controversial)
ANATOMY IMAGING ISSUES
Imaging Recommendations
•Transducer
○2.5-5 MHz curvilinear or vector transducer is generally most suitable
○Higher frequency linear transducer (i.e., 7-9 MHz) useful for evaluation of liver capsule and superficial portions of liver
•Left lobe
○Subcostal window with full inspiration generally most suitable
•Right lobe
○Subcostal window
–Cranial and rightwards angulation useful for visualization of right lobe below dome of hemidiaphragm
–Can sometimes be obscured by bowel gas
○Intercostal window
–Usually gives better resolution for parenchyma without influence from bowel gas
–Right lobe just below hemidiaphragm may not be visible due to obscuration from lung bases
–Important to tilt transducer parallel to intercostal space to minimize shadowing from ribs
Imaging Pitfalls
•Because of variations of vascular and biliary branching within liver (common), it is frequently impossible to designate precisely boundaries between hepatic segments on imaging studies
CLINICAL IMPLICATIONS
Clinical Importance
•Liver ultrasound often first-line imaging modality in evaluation for elevated liver enzymes
○Diffuse liver disease, such as hepatic steatosis, cirrhosis, hepatomegaly, hepatitis, and biliary ductal dilatation, are well visualized with ultrasound
○Documentation of patency of portal vein, hepatic vein waveforms, and hepatic arterial velocities are helpful in evaluation for etiologies of elevated liver function tests
•Liver metastases are common
○Primary carcinomas of colon, pancreas, and stomach are common
–Portal venous drainage usually results in liver being initial site of metastatic spread from these tumors
○Metastases from other non-GI primaries (breast, lung, etc.) commonly spread to liver hematogenously
•Primary hepatocellular carcinoma
○Common worldwide
–Risk factors include chronic viral hepatitis B or C, alcoholic cirrhosis, or nonalcoholic steatohepatitis
–Ultrasound commonly used for screening and surveillance in patients at risk for development of hepatocellular carcinoma (HCC) typically at 6 month intervals
SELECTED REFERENCES
1.Heller MT et al: The role of ultrasonography in the evaluation of diffuse liver disease. Radiol Clin North Am.52(6):1163-75, 2014
2.McNaughton DAet al:Doppler US of the liver made simple. Radiographics. 31(1):161-88, 2011
3.Kruskal JB et al: Optimizing Doppler and color flow US: application to hepaticsonography.Radiographics. 24(3):657-75, 2004
Abdomen Anatomy:
5
Anatomy: Abdomen
Liver
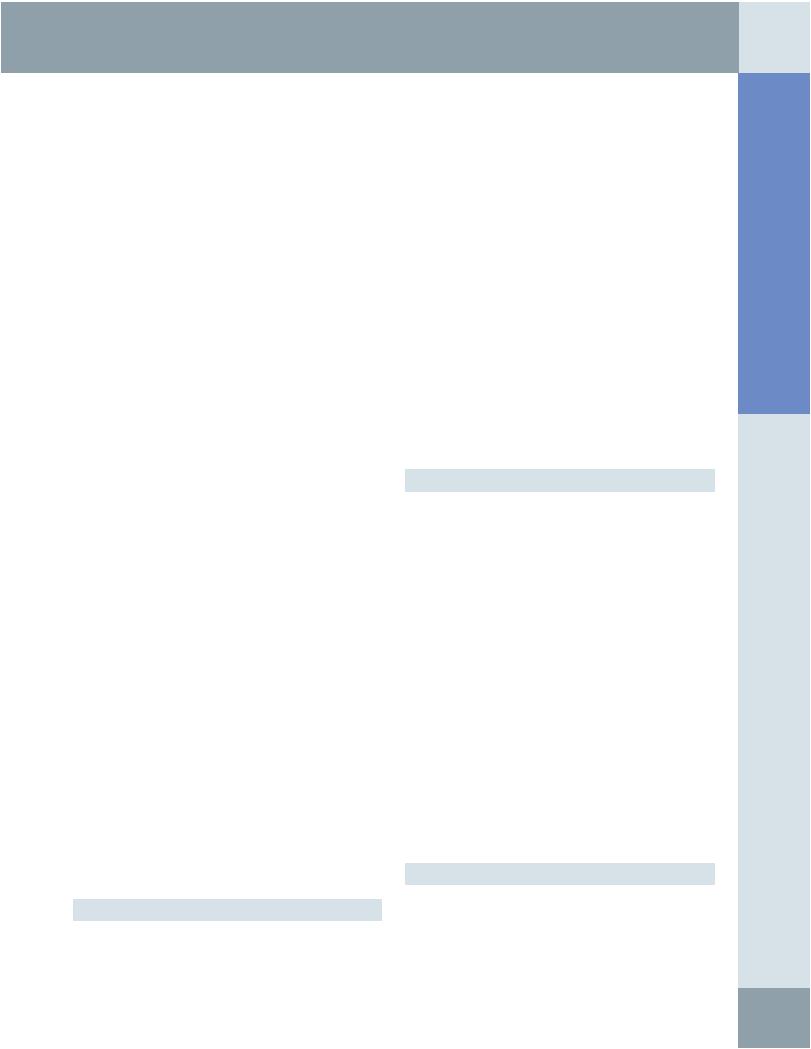
HEPATIC VISCERAL SURFACE
Coronary ligament
Right triangular ligament
Gallbladder
Gallbladder
Porta hepatis
Right renal impression
Bare area
Diaphragm
Left triangular ligament
Falciform ligament
Ligamentum teres
Falciform ligament
Gastric impression
Fissure for ligamentum venosum
Inferior vena cava
(Top) The anterior surface of the liver is smooth and molds to the diaphragm and anterior abdominal wall. Generally, only the anterior/inferior edge of the liver is palpable on a physical exam. The liver is covered with peritoneum, except for the gallbladder bed, porta hepatis, and the bare area. Peritoneal reflections form various ligaments that connect the liver to the diaphragm and abdominal wall, including the falciform ligament, the inferior edge that contains the ligamentum teres, and the obliterated remnant of the umbilical vein. (Bottom) This graphic shows the liver inverted, which is somewhat similar to the surgeon's view of the upwardly retracted liver. The structures in the porta hepatis include the portal vein (blue), hepatic artery (red), and the bile ducts (green). The visceral surface of the liver is indented by adjacent viscera. The bare area is not easily accessible.
6
Liver
Coronary ligament
Adrenal gland
Right triangular ligament
Falciform ligament
Left triangular ligament
Ligamentum venosum
Lateral segment (left lobe)
Falciform ligament
Medial segment (left lobe)
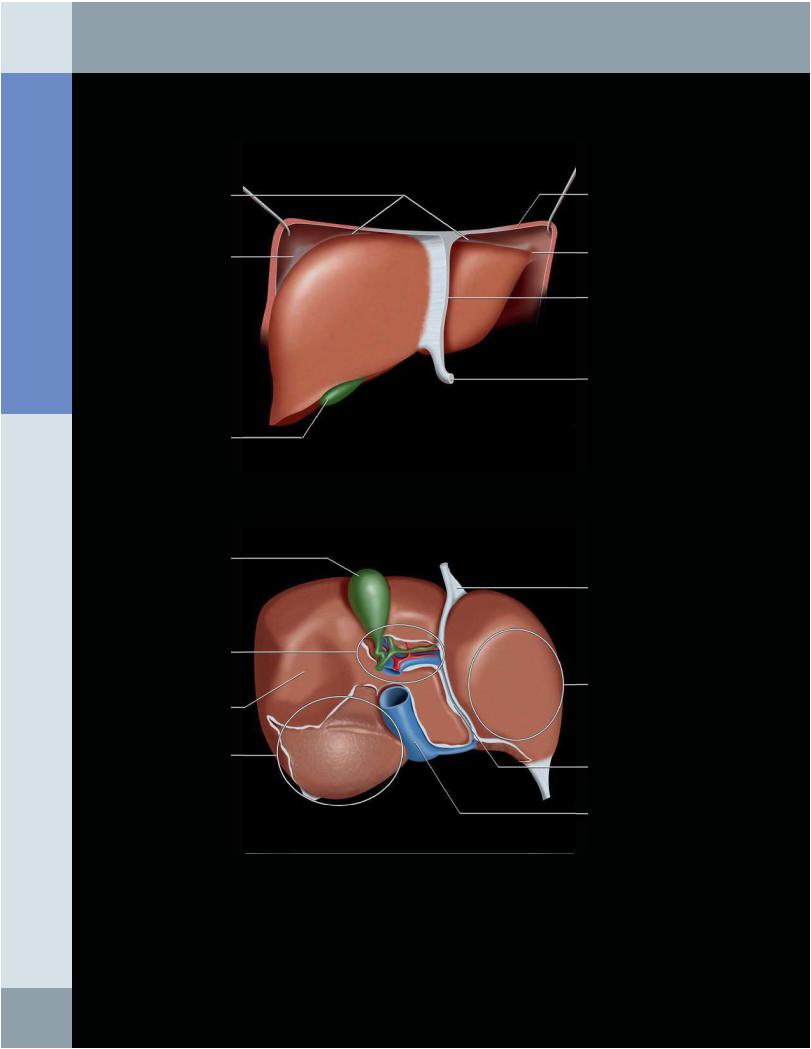
HEPATIC ATTACHMENTS AND RELATIONS
Falciform ligament
Left triangular ligament
Lesser omentum
Coronary ligament
Sulcus for IVC
Right triangular ligament
Right lobe
(Top) The liver is attached to the posterior abdominal wall and diaphragm by the left and right triangular and coronary ligaments. The falciform ligament attaches the liver to the anterior abdominal wall. The bare area is in direct contact with the right adrenal gland, kidney, and inferior vena cava (IVC). (Bottom) Posterior view of the liver shows the ligamentous attachments. While these may help to fix the liver in position, abdominal pressure alone is sufficient, as evidenced by orthotopic liver transplantation, after which the ligamentous attachments are lost without the liver shifting position. The diaphragmatic peritoneal reflection is the coronary ligament whose lateral extensions are the right and left triangular ligaments. The falciform ligament separates the medial and lateral segments of the left lobe.
Abdomen Anatomy:
7
Anatomy: Abdomen
Liver
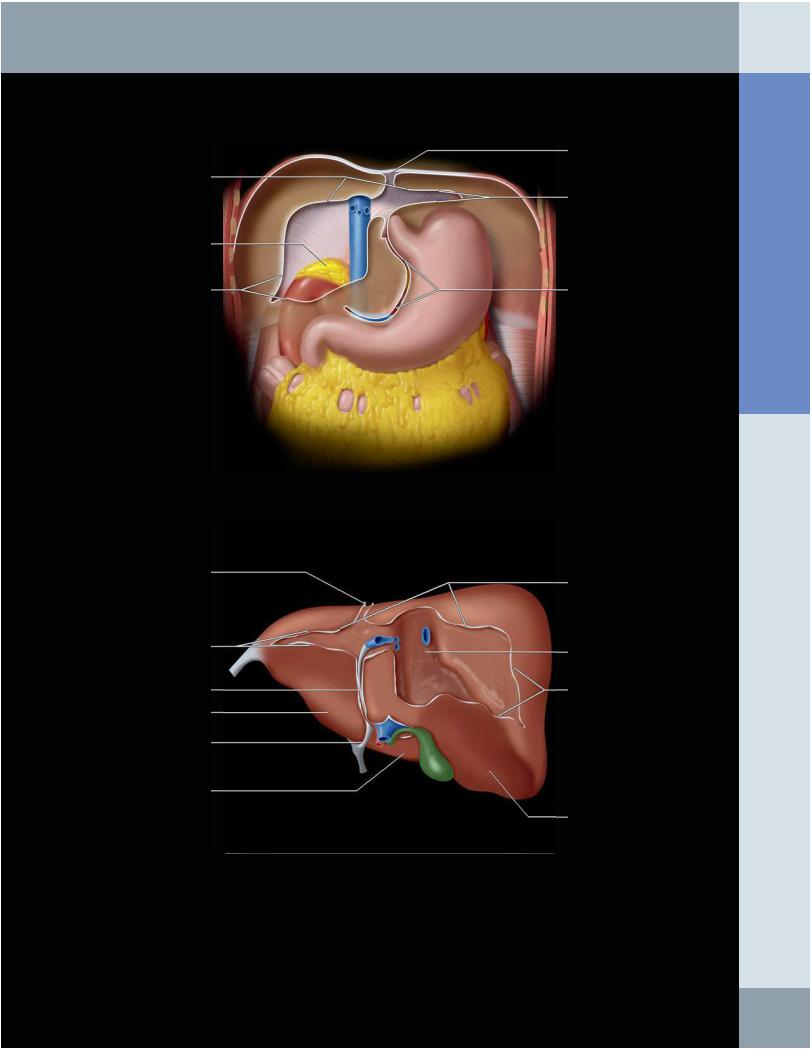
HEPATIC VESSELS AND BILE DUCTS
Right hepatic vein (separates anterior and posterior segments of right lobe of liver)
Right hepatic duct
Right portal vein
Right hepatic artery
Common hepatic duct
Cystic duct
Gallbladder
Common bile duct
Left hepatic vein (separates medial and lateral segments of left lobe of liver)
Middle hepatic vein (separates right and left lobes of liver)
Left hepatic duct
Left portal vein
Left hepatic artery
IVC
Main portal vein
This graphic emphasizes that at every level of branching and subdivision, the portal veins, hepatic arteries, and bile ducts course together, constituting the "portal triad." Each segment of the liver is supplied by branches of these vessels. Conversely, hepatic venous branches lie between hepatic segments and interdigitate with the portal triads, but never run parallel to them.
8

Liver
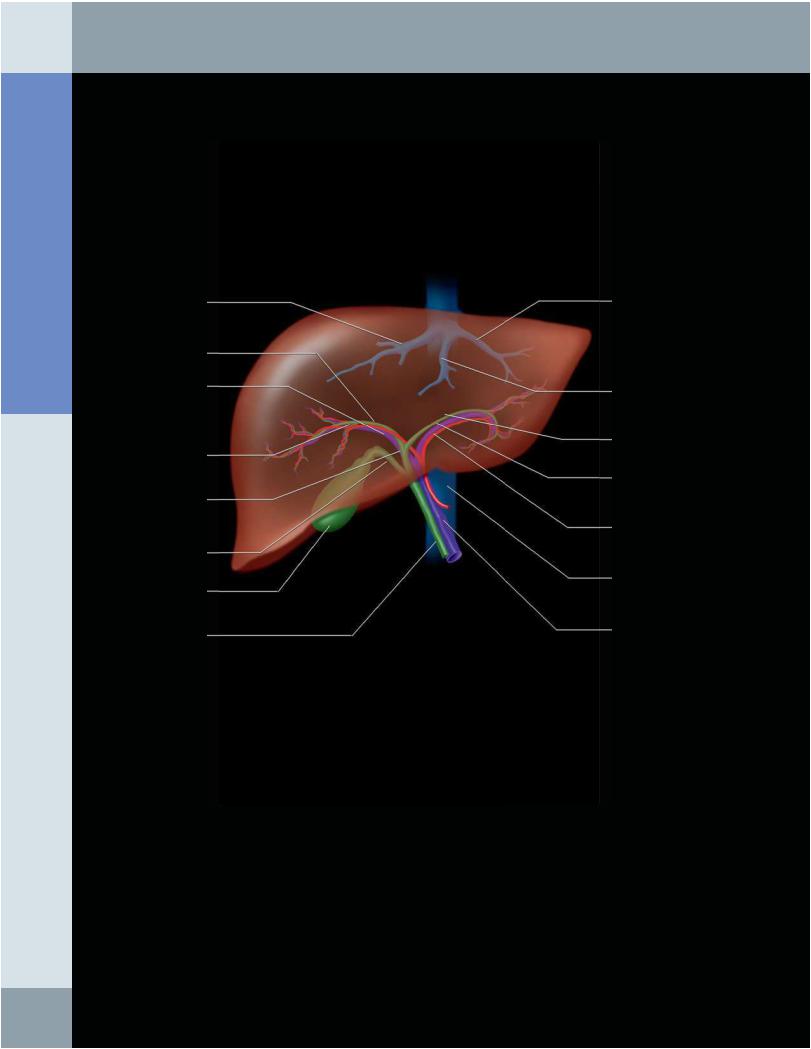
HEPATIC SEGMENTS
Segment 8 |
Segment 4A |
|
|
|
Segment 2 |
Segment 7 |
Segment 3 |
|
|
|
Falciform ligament |
Segment 6
Segment 4B
Segment 5
Segment 4B
Segment 5
Segment 6
Segment 3
Segment 1
Segment 2
Segment 7
Segment 4A
(Top) The 1st of 2 graphics demonstrating the segmental anatomy of the liver in a somewhat idealized fashion is shown. Segments are numbered in a clockwise direction, starting with the caudate lobe (segment 1), which cannot be seen on this frontal view. The falciform ligament divides the lateral (segments 2 and 3) from the medial (segments 4A and 4B) left lobe. The horizontal planes separating the superior from the inferior segments follow the course of the right and left portal veins. An oblique vertical plane through the middle hepatic vein, gallbladder fossa ,and IVC divides the right and left lobes. (Bottom) Inferior view of the liver shows that the caudate is entirely posterior, abutting the IVC, ligamentum venosum, and porta hepatis. In this view, a plane through the IVC and gallbladder approximately divides the left and right lobes.
Abdomen Anatomy:
9
Anatomy: Abdomen
Liver
TRANSVERSE VIEW OF LEFT LOBE OF LIVER
|
Subcutaneous fat |
|
|
Segment 3 |
|
Rectus abdominis muscle |
Pancreas |
|
Segment 4b |
||
Splenic vein |
||
|
||
Falciform ligament |
Left renal artery |
|
|
||
Portal vein |
Aorta |
|
|
||
IVC |
Spine |
|
|
|
Ligamentum venosum |
Rectus abdominis muscle |
|
Falciform ligament |
Pancreas |
Left portal vein |
|
IVC |
Aorta |
Middle hepatic vein |
|
Rectus abdominis muscle
Portal vein branch
Left hepatic vein
Middle hepatic vein
Right hepatic vein
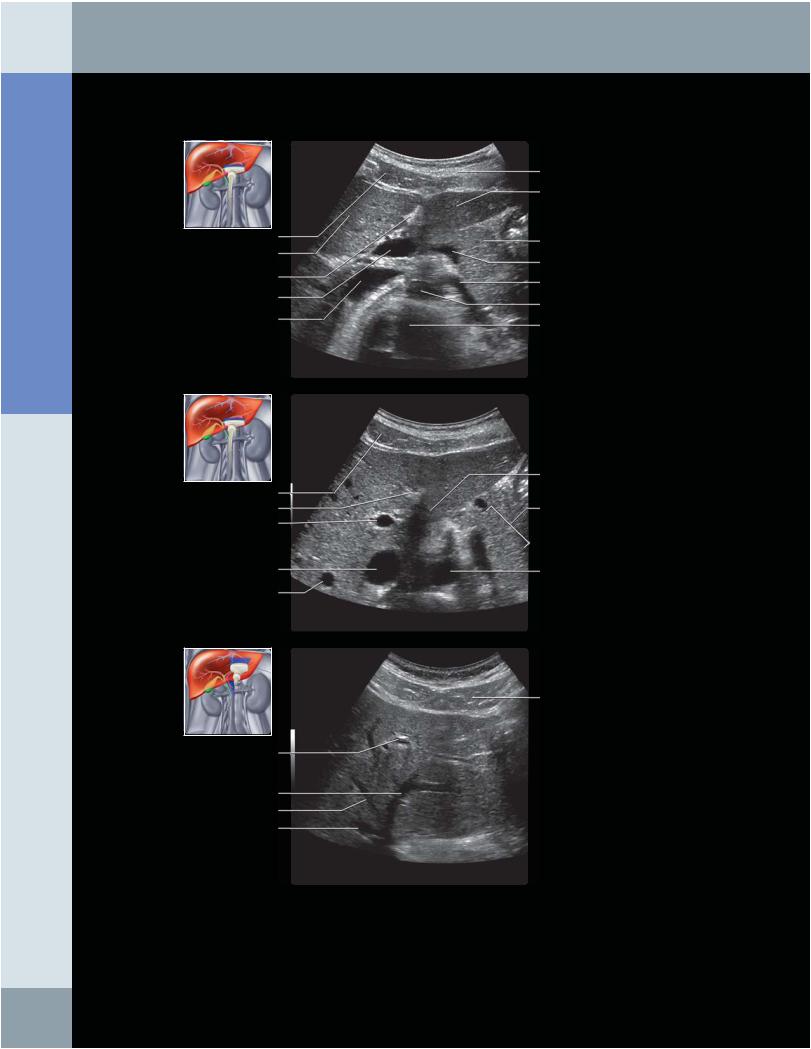
(Top) Transverse grayscale ultrasound of the left lobe of the liver is shown, centered at the level of the falciform ligament and pancreas. (Middle) Transverse grayscale ultrasound of the left lobe of the liver is shown. (Bottom) Transverse grayscale ultrasound of the left lobe of the liver is shown, centered at the level of the left hepatic vein.
10
Liver
Rectus abdominis muscle
Left portal vein
Middle hepatic vein
IVC
RIght hepatic vein
Rectus abdominis muscle
Left portal vein
IVC
Rectus abdominis
Left portal vein
Middle hepatic vein Right portal vein
Right hepatic vein
IVC
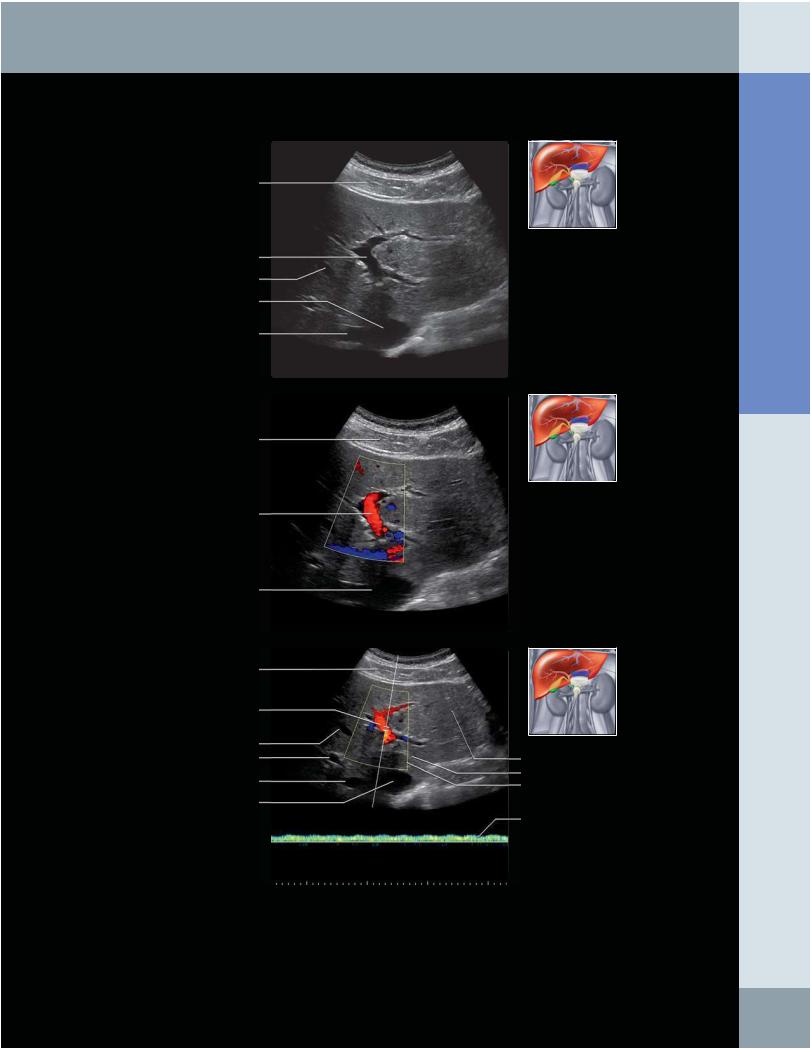
LEFT LOBE OF LIVER: LEFT PORTAL VEIN
Left lobe lateral segment
Ligamentum venosum
Caudate lobe
Spectral tracing of left portal vein
(Top) Transverse grayscale ultrasound of the left lobe of the liver is shown, centered at the left portal vein. (Middle) Transverse color Doppler ultrasound of the left lobe of the liver is shown, centered at the level of the left portal vein. Flow in the left portal vein is directed towards the transducer, indicating that the flow is hepatopetal and therefore normal. (Bottom) Spectral tracing of the left portal vein on this transverse pulsed Doppler ultrasound shows that the flow is monophasic, directed towards the transducer, with a mildly undulating waveform related to slight transmission of the cardiac cycle, which is a normal appearance for the portal vein.
Abdomen Anatomy:
11
Anatomy: Abdomen
Liver
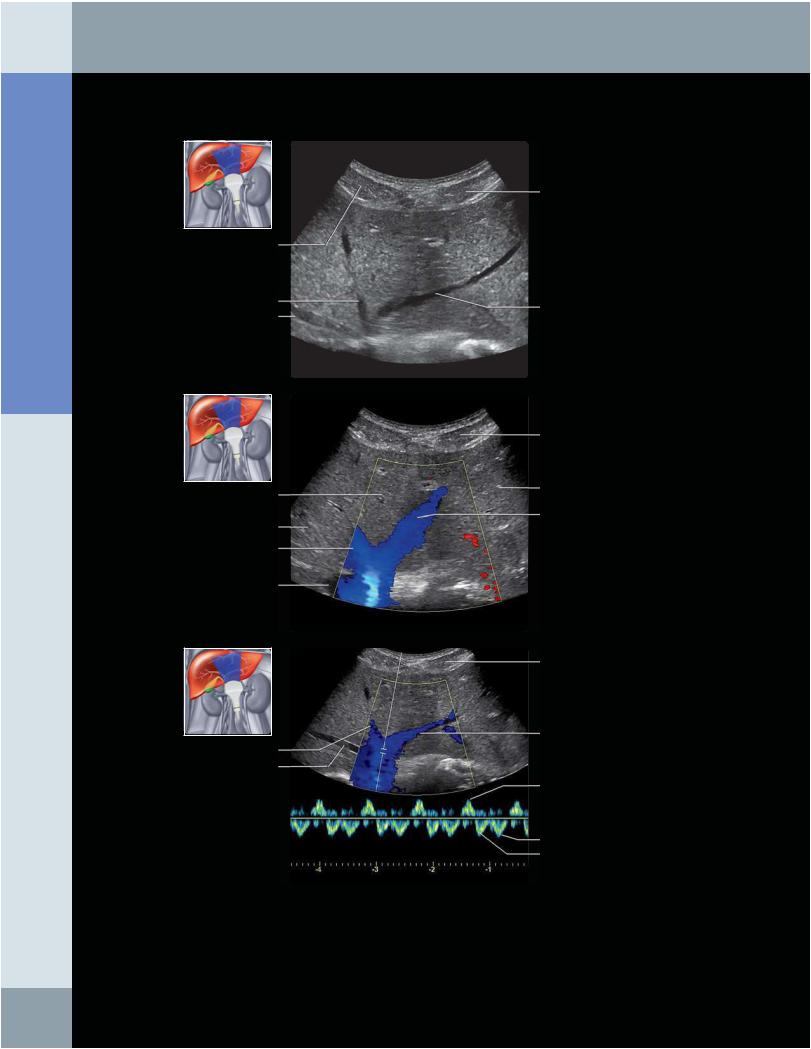
LEFT LOBE OF LIVER: LEFT HEPATIC VEIN
Right rectus abdominis muscle
Middle hepatic vein
Right hepatic vein
Segment 8
Segment 7
Middle hepatic vein
IVC
Middle hepatic vein
Right hepatic vein
Left rectus abdominous muscle
Left hepatic vein
Left rectus abdominis muscle
Segment 2
Left hepatic vein
Left rectus abdominis muscle
Left hepatic vein
A wave
D wave
S wave
(Top) Transverse grayscale ultrasound of the liver centered at the left hepatic lobe shows the right, middle, and left hepatic veins as they join into the intrahepatic IVC. (Middle) Transverse color Doppler ultrasound of the liver, centered at the confluence of the hepatic veins, shows that the flow direction is away from the transducer, directed towards the IVC. (Bottom) Spectral tracing the left hepatic vein near the confluence with the IVC shows a characteristic triphasic waveform pattern, which represents reflection of cardiac motion.
12
Liver
Abdominal muscle
Diaphragm
Heart
Heart
Aorta
Left portal vein
Heart
Left hepatic vein
Junction of IVC and right atrium
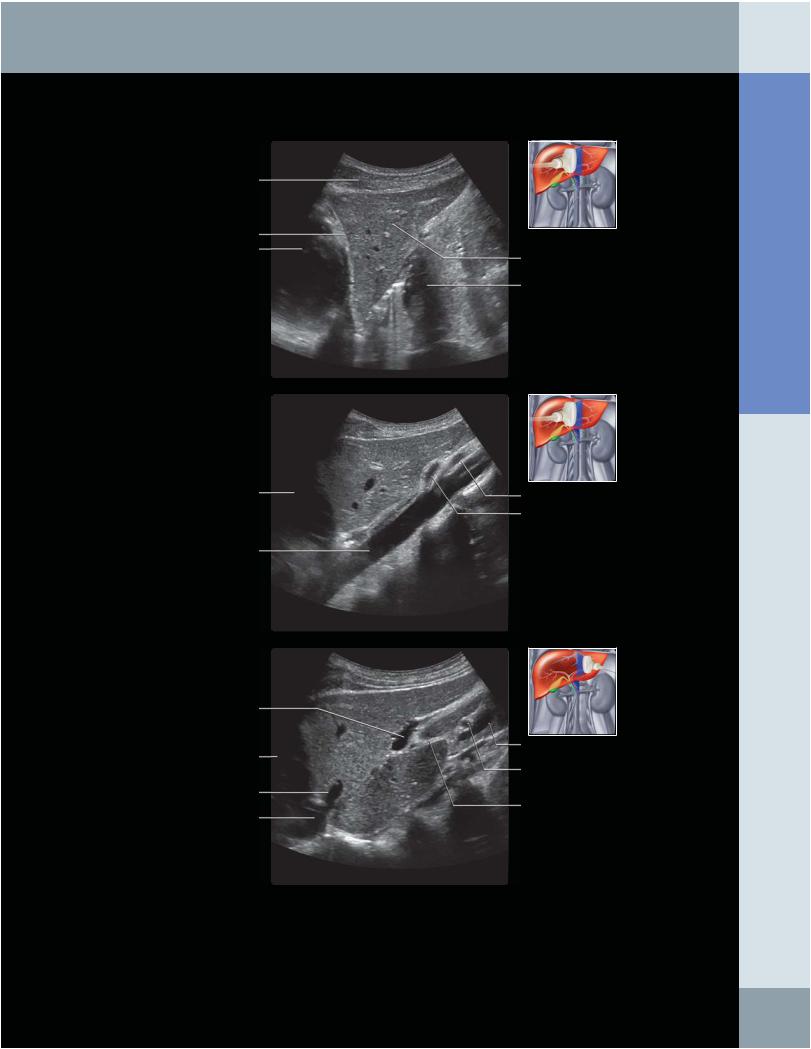
LEFT LOBE OF LIVER: LONGITUDINAL VIEW
Left lateral liver
Stomach
Superior mesenteric artery
Celiac artery
Portal vein
Hepatic artery
Falciform ligament
(Top) Longitudinal grayscale ultrasound of the left lobe of the liver shows a triangular-shaped cross section. The heart is partially visualized above the diaphragm. (Middle) Longitudinal grayscale ultrasound view of the left lobe of the liver at the level of the aorta shows the aorta posterior to the liver, the celiac artery, and superior mesenteric artery arising from the aorta. (Bottom) Longitudinal grayscale ultrasound of the left lobe of the liver shows the left hepatic vein and left portal vein in cross section.
Abdomen Anatomy:
13