

Cardiology / English / Internal_diseases_propedeutics._Part_II._Diagnostics_of_cardiovascular_diseases
.pdfIn any case, the stethoscope must be moved step-by-step slowly from area to area to «not to omit» any important finding in the presence of pathology, while listening to the heart.
The heart auscultation: heart sounds abnormalities
Phase of ventricular systole is the asynchronous contraction, isovolumic (isometric) contraction, the exile (fast and slow).
Phase of diastole ventricular – izovolemic reductio n, quick blood circulation, slow blood circulation.
I tone – systolic, consists of:
a)the valve component vibrations of the valves atrioventricular valves in the phase izovolemic reduction.
b)muscular component – vibration of ventricular my ocardium in the phase izovolemic reduction.
C)the vascular component of oscillations of the initial segment of the aorta and pulmonary trunk in tension with their blood during the exile
II tone – diastolic, comprises:
a)the valve component vibrations of the valves the semilunar valves of the aorta and the pulmonary trunk when closed in early diastole
b)the vascular component oscillations of the walls of the aorta and the pulmonary trunk at the beginning of diastole.
The aortic component is almost always normal and disease precedes pulmonary, because aortic valve closes slightly before the valve LA.
III tone – vibrations during rapid passive filling of the ventricles with blood from the Atria during diastole (using a 0.12-0.15 from the beginning of the II tone)
The IV tone is ventricular filling in late diastole due to active contraction of Atria. III and IV the normal tones are heard only in children and young lean people,
especially on the left side, clearly recorded on the FCG. Identification of III and IV tones from middle aged persons and the elderly – patholog y.
In clinical practice the following changes of heart sounds may be met:
31
1.Volume change of the main sounds (S1 and S2);
2.Splitting (doubling) of the main sounds;
3.Appearing of additional sounds: S3 and S4, mitral valve opening snap (OS), additional systolic sound (click) and the so-called pericardium tone.
Diminished first heart sound. The first heart sound may be diminished by the following reasons:
1.incomplete closure of atrioventricular valves (for example, in mitral or tricuspid incompetence),
2.sharp slowing down of ventricle contraction and increase of intraventricular pressure due to myocardial contractile capacity decrease in patients with cardiac insufficiency and acute myocardial lesion.
3.significant slowing down of hypertrophic ventricle contraction, for example, in aortic stenosis;
4.unusual position of atrioventricular valves cusps just before the beginning of isovolumetric ventricular contraction.
Accentuating of S1. There exist two main reasons of accentuating of S1:
1.increase of isovolumetric ventricular contraction rate for example, in tachycardia or thyrotoxicosis, when the rate of all the metabolic processes in the organism, including myocardium, is increased;
2.consolidation of cardiac structures taking part in vibrations and formation of the first sound, for example, in mitral stenosis.
Diminished S2. The main reasons of the second heart sound diminishing are:
1.non-hermetic closure of aortic and pulmonary artery semilunar valves;
2.decreased rate of semilunar valves closure in:
a.heart failure accompanied by decreased rate of ventricles rela-xation;
b.arterial pressure decrease;
3. adhesion and decrease of motility of semilunar valves cusps, for example, in valvular aortic stenosis.
32
Accentuating S2 Enhancing (accent) of the second heart sound on aorta may be
caused by:
1.arterial pressure increasee of various genesis (due to increase of aortic valve cusps shutting rate);
2.consolidation of aortic va lve cusps and aortic walls (atherosclerosis, syphilitic aortitis, etc).
Main reason of S1 split ting is asynchronous closure and vibr ations of mitral (M) and tricuspid (T) valves. Such situation may appear, for example, in case of the right bundle branch block
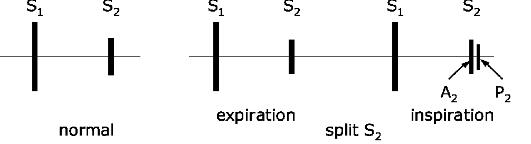
Doubling and splitting of S2 are, as a rule, associated with in crease of blood ejection time of the right ventricle a nd/or decrease of blood ejection time of the left ventricle that leads, respectively, to later appearance of pulmonary component a nd/or earlier appearance of aortic component of S2 (F ig. 17.).
Fig. 17. Physiologic splitting of S2 can usually be detected i n the 2nd left interspace. The pulmonic component o f S2 is usually too faint to be heard at the apex or aortic area, where S2 is single and deriveed from aortic valve closure alone.
Any change of diasto lic ventricular myocardial tonus, rate of its relaxation or increase of atrium volume may lead to appearance of pathologic third heart sound, or protodiastolic gallop rhythm (Fig.18).
33

Fig. 18. Third heart sound occurs early in diastole during rapid ventricular filling. It is later than an opening snap, dull and low in pitch, and heard bes t at the apex in the left lateral decubitus position. The bell of the stethoscope should be used with very light pressure.
The fourth heart sound (S4) (presystolic) may be heard in systemic hypertension and in idiopathic hypertrophic s ubaortic stenosis. It has been attributed to sudden ventricular distention associated with an augmented left atrial contraction and increased left ventricular end-diastolic str etch (Fig. 19). In healthy people phys iologic fourth sound is very soft, low frequent a nd is found rather rarely, predomin antly in children and teenagers. Pathologic accentuation of S4 in adults is named as pre-systolic gallop rhythm.
Fig. 19. Fourth heart sound is an atrial contraction sound that occurs in late diastole, preceding S1. S4 has a dull, low pitch, and heard better with the bell.
The third or fourth heart sounds may be heard in rapid succession with first and second heart sounds (triple r hythm), when the heart rate is fast. T he cadence so produced has been likened to a horse' s gallop, and is called gallop of the thir d (Lup De-da, Lup De-
34
da) or forth heart sound (De La-lup, De La-lup). A gallop or triple rhythm of the third heart sound may be heard in young healthy subjects after exercise. It is an important sign of heart failure from any cause, and it almost always arises from rapidly filling left ventricle. A gallop of the fourth heart sound, unlike that of the third sound, is not a sign of failure but of compensation.
A gallop of all four heart sounds (summation gallop) is sometimes heard in heart failure. Summation gallop is a three-part ventricular rhythm when, in result of sharp shortening of slow filling phase in presence of tachycardia pathologic S3 and S4 merge into one additional sound.
Aortic ejection click is a sharp, brief, high-pitched sound, which occurs soon after the first heart sound (after the closure of the aortic valve). It is best heard in expiration over the aortic area and the apex. It is associated with dilatation of the aorta and can be heard in cases of hypertension, coarctation and atherosclerosis.
Systolic gallop is a three-part rhythm appearing in case of additional short sound, or systolic flap, rise in the period of ventricles systole (between S1 and S2).
A nonejection systolic click is heard together with a systolic murmur in association with mitral valve prolapse. The mitral valve leaflets do not coapt during systole; the posterior cusp prolapses, sometimes indicated by a click, and the ensuing murmur is caused by regurgitation of blood into the left atrium.
In various manuals rhythm of quail is called «quail rhythm». Mitral valve opening snap (OS) appears exclusively in case of mitral stenosis at the moment of mitral valve cusps opening.
In fact, such sounds are emitted by quail. Quail (Latin Coturnix coturnix) is a bird, subfamily partridge, galliformes class (Boehme R.L, V.E. Flint, 1994). «Male sings, the female brings out nestlings, so it is quiet, not showing her nest. Experts claim that not all quails sing the same. They, like humans, have different tone and voice power. Some have clean, loud one, and are heard a mile away, while others are more gentle and pleasant» (Isachenko L. Science and Life, 2006. - № 1).
35
The heart auscultation: heart murmurs
Cardiac murmurs are relatively long lasting sounds appearing during turbulent blood motion. The turbulence appears in case of disturbance of three hemodynamic parameters normal proportion:
1.Diameter of valve ostium or vessel lumen;
2.Blood flow velocity (linear or volume);
3.Blood viscosity.
Murmurs heard above the region of the heart and large vessels are divided into intraand extracardiac.
Intracardiac murmurs.
Intracardiac murmurs are divided into:
1.organic, appearing due to rough organic lesion of valves and other cardiac anatomic structures (interventricular or interatrial septum);
2.functional murmurs based not on rough anatomic structures lesions, but on lesion of valvular functions, blood flow acceleration through anatomically unchanged ostiae or blood viscosity decrease.
Organic murmurs: all the organic intracardiac murmurs appear in presence of narrowing, dilation or other obstacles, for example, parietal thrombus or atherosclerotic patch on aortic wall in cardiac cavities or initial parts of main vessels.
One should give its detailed characteristic, namely, define:
1.murmur relation to cardiac activity phases (systolic, diastolic, etc.) (Fig. 20, 21);
2.region of maximal murmur intensity;
3.murmur transmission;
4.timbre, volume of the murmur;
5.shape of murmur.
For more information look at tables 3,4
36
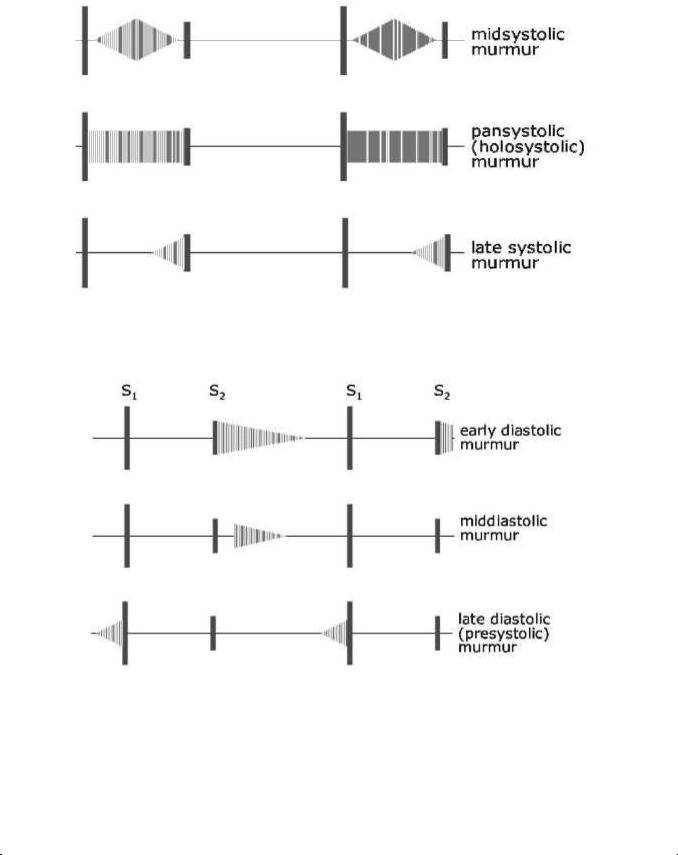
Fig. 20. Main types of systolic murmurs.
Fig. 21. Main types of diastolic murmurs.
Table 3.
Chief systolic murmurs
Time and quality |
Accompanying signs |
|
Interpretation |
|
|
|
|
1. Ejection, harsh midsystolic |
Slow rising pulse, low |
systolic pressure, |
Aortic stenosis |
accentuation or prolonged |
heaving apex beat, systolic thrill, ejection click, |
|
|
|
|
|
|
|
37 |
|
|

|
|
|
|
|
|
|
soft or absent A2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
2. |
Ejection, as above. Loudest |
Jerky pulse, atrial impulse over |
apex, |
lifting |
Hypertrophic |
obstructive |
|||||||||
in left 3rd, 4th interspace |
|
|
apex beat |
|
|
|
|
|
|
cardiomyopathy |
|||||
|
|
|
|
|
|
|
|
|
|||||||
3. Ejection, as above |
|
|
Hyperkinetic |
states, |
aortic |
incompetence, |
Increased flow |
||||||||
|
|
|
|
|
|
|
complete heart block |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
4. Ejection, as above |
|
|
No signs |
|
|
|
|
|
|
Aortic stenosis |
|||||
|
|
|
|
|
|
|
|
|
|
|
|||||
5. |
Ejection, |
over |
pulmonary |
Increases during inspiration |
|
|
|
|
Pulmonary stenosis |
||||||
area |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
6. |
Ejection, |
short, |
over |
Hyperkinetic states, left-to-right |
|
shunt |
(ASD, |
Increased flow |
|||||||
pulmonary area |
|
|
|
VSD) |
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
7. |
Late |
ejection, |
over |
mitral |
Mid-systolic click |
|
|
|
|
|
Mitral valve prolapse |
||||
area |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
8. |
Pansystolic, |
blowing, |
Large volume |
pulse, |
displaced |
and vigorous |
Mitral incompetence |
||||||||
mostly uniform |
|
|
|
apex, right ventricular heave, S3, louder during |
|
|
|||||||||
|
|
|
|
|
|
|
expiration |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
9. |
Pansystolic, as above. Best |
As above plus thrill frequently presents |
|
Ventricular septal defect |
|||||||||||
heard |
over |
left |
|
3rd, |
|
|
|
|
|
|
|
(VSD) |
|
||
4th interspace |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Table 4. |
|
|
|
|
|
|
|
Chief diastolic murmurs |
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|||||||
Time and quality |
|
|
Accompanying signs |
|
|
|
Interpretation |
|
|||||||
|
|
|
|
|
|
||||||||||
1. |
Early diastolic, high- |
Collapsing pulse, Corrigan's sign, |
wide |
Aortic incompetence |
|
||||||||||
pitched, blowing |
|
|
pulse pressure, displaced and vigorous |
|
|
|
|
||||||||
|
|
|
|
|
|
apex |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
2. |
Early diastolic, |
a short, |
Prominent 'a' wave, right ventricular heave |
Graham |
Steell |
murmur |
|||||||||
high-pitched whiff |
|
|
loud P2 |
|
|
|
|
(functional |
pulmonary |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
incompetence) |
|
||
|
|
|
|
|
|
||||||||||
3. |
Mid-diastolic, |
rough, |
Malar flush, small volume pulse, tapping |
Mitral stenosis |
|
||||||||||
rumbling |
|
|
|
|
impulse, right ventricular heave, opening |
|
|
|
|
||||||
|
|
|
|
|
|
snap |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
4. |
Mid-diastolic, |
short,Signs of mitral |
incompetence, VSD |
orInflow (mitral) murmur |
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
38 |
|
|
|
|
|
|
|

following S3 |
|
paten t ductus |
|
|
|
|
|
|
|
|
|
|
|
5. |
Mid-diastolic, |
short, |
Sign s of atrial septal defect (ASD) |
|
Inflow |
(tricuspid) murmur |
over tricuspid area |
|
|
|
|
|
|
|
|
|
|
|
|
|
6. |
Continuous systolic and |
Colla psing pulse, thrill, mitral |
inflow |
Patent |
ductus, aortopulmonary |
|
diastolic, machinery noise |
murm ur |
|
septal defect |
|||
|
|
|
|
|
|
|
Examples of most cha racteristic murmurs in five acquired cardiac defects: mitral incompetence, mitral stenosi s, aortic stenosis, tricuspid incompete nce.
Mitral incompetence is characterized by diminished S1, systo lic murmur appearance and S2 accent at the pulmon ary artery. On PhonoCG decrease of S1 amplitude is marked in significant mitral incompetence due to falling out of S1 v alvular component and overfilling of left ventricle. Minor degree of mitral incompetence isn't accompanied by S1 diminishing. The most imp ortant in mitral incompetence diagn ostics is a presence of systolic murmur with maxi mal intensity at the apex (Application Fig.2). In severe valve disease murmur of considera ble intensity is registered at the left ax illa. Systolic murmur is directly connected with def ect, formed between valve leaflets a nd reverse blood flow (regurgitation) through this chink. Murmur in mitral incompetence begins directly after S1 and has decrescent character. It may occupy all systole (pansy stolic) or part of systole according to the degree of mitral incompetence. Murmur amplitude is more when the defect is pronounced (Fig. 2 2).
Fig. 22. When the mitr al valve fails to close fully in systole, blood regurgitates from left ventricle to left atrium, causing a murmur. S1 is often decrease d. An apical S3 reflects the volume overload on the l eft ventricle.
39

At the pulmonary artery increase of S2 pulmonary compone nt (P2) is noticed, S2 is frequently splitted.
Mitral stenosis: Since a little amount of blood gets into left ventricle and it contracts fast, so S1 at the apex beco mes loud, flapping. Here after S2 the a dditional heart sound – mitral opening snap – is listened. Flapping S1, S2 and openin g snap (OS) create the typical of mitral stenosis m elody called ―quail rhythm (Fig.23). A rumbling diastolic murmur at the apex is typical of mitral stenosis, because there is narrowing down blood flow from the left atrium to the left ventricle on diastole (Application Fig.1). This murmur may occur in the very beginning of diastole, i.e. to be protodiastolic, because due to pressure gradient in atrium and ventricle the blood flow velocity will be higher at the diastole beginning. However, murmur appears only at the end of diastole before the very systole – presystolic murmur, which appears in blood flow acceleration at the end of diastole due to atrial contra ction. There may be presystolic accen tuation and the murmur may be preceded by an opening snap. Exercise and positioning the patient in the left lateral position will accentua te the murmur (Fig.22).
Fig. 23. When the leaflets of the mitral valve thicken, stiffen, and become distorted, the valve fails to open suffic iently in diastole. The resulting murmur has two components: mid-diastolic (during rapid ventricular filling), and presystolic (du ring atrial contraction). S1 is accentuated. An openin g snap (OS) often follows S2 and initia tes the murmur.
As pulmonary hypertension develops, the pulmonary s econd sound becomes accentuated.
Aortic incompetence: o n auscultation diminished S1 at the ap ex is revealed, because during systole there is no pe riod of closed valves. S2 at the aorta is also diminished, and
40