

Cardiology / English / Internal_diseases_propedeutics._Part_II._Diagnostics_of_cardiovascular_diseases
.pdfa)displacement of right border of relative dullness of heart to the right;
b)the offset of the left border of relative dullness of heart to the left;
c)the displacement of the upper borders of relative dullness of the heart upward;
d)accentuated waist of heart;
e)waist smoothed heart.
39.DESCRIBE THE APEX BEAT IN A PATIENT WITH AORTIC VALVE INSUFFICIENCY IN THE STAGE OF COMPENSATION (3 ANSWERS): a) enhanced apex beat;
b) weakened apex beat;
c) displacement apex beat to the left;
g) shifting apex beat to the left and down (the sixth to seventh intercostal space); d) no significant bias apex beat;
e) apex beat diffuse.
40.HOW TO CHANGE THE PERCUS SHAPE OF THE HEART IN A PATIENT WITH AORTIC VALVE STENOSIS IN THE STAGE OF COMPENSATION (ONE ANSWER)?
a) displacement of right border of relative dullness of heart to the right; b) significant shift of the left border of the heart to the left;
c) the offset the upper border of the heart upward;
d) the absence of significant displacements of the heart boundaries.
41.WHICH 3 OF THE FOLLOWING COMPLAINTS ARE CHARACTERISTIC IN FOR PATIENT SUFFERING FROM AORTIC VALVE INSUFFICIENCY (3ANSWERES)?
a) dyspnea during physical exertion and in the supine position;
b) pain in the heart area and behind the breastbone radiating to the left arm and under the shoulder blade;
c) persistent sensations of faults in work of heart ("chaotic rhythm"); d) swelling of the feet (more towards evening);
e) dizziness and (sometimes) momentary fainting during physical load; f) dyspnea and unproductive cough with streaks of blood at night;
g) heartbeat, feeling of pulsation in the whole body.
42.DESCRIBE THE PULSE IN A PATIENT WITH AORTIC VALVE INSUFFICIENCY (GIVE ONE ANSWER).
91
a)high and imminent ("galloping" – pulse Corrigan) ;
b)low and slow;
c)scarce (pulsus deficience);
d)different (pulsus difference).
43.SPECIFY 2 MAIN DIAGNOSTIC AUSCULTATION SIGNS OF THE AORTIC VALVE STENOSIS (RHEUMATIC ETIOLOGY):
a) strengthening II tone of the aorta;
b) the weakening of the II tone over the aorta;
c) systolic murmur in the second intercostal space to the right of the sternum and at the point Botkin, performed in the vessels of the neck;
d) systolic murmur at the apex
44.WHAT ARE 2 VALIDLY DISTINGUISH CHARACTERISTIC OF PAIN SYNDROME DEVELOPING IN A PATIENT WITH MYOCARDIAL INFARCTION FROM ANGINAL PAIN IN A PATIENT WITH ANGINA?
a) localization of pain;
b) nature of pain (pressure, burning, etc.); c) irradiation;
d) the duration of the pain;
e) the relationship of pain to physical load;
f) the relationship of pain to the taking nitroglycerin; g) the relationship of pain to take validol.
45.WHICH 3 OF THE FOLLOWING SIGNS ARE THE MOST INFORMATIVE FOR RECOGNITION OF ACUTE MYOCARDIAL INFARCTION (MI)?
a) a history of clinical manifestations of IHD (angina, myocardial infarction etc.); b) onset of the disease with prolonged chest pain, not stoped nitroglycerin;
c) the beginning of disease with rise in temperature, cough and the appearance of intense sweep-ing pain in the left 1/2 of the thorax, worse on inspiration;
d) increasing the left border of the relative dullness of the heart; e) the weakening of the heart sounds;
f) fluctuations in blood pressure;
g) appearance of ECG pathological Q wave (or QS complex) or of changes in ST segment or T wave;
h) appearance of ECG signs of atrial fibrillation and increase of alkaline phosphatase activity in blood serum on the 2nd day of illness;
92
i) increasing the activity of aspartic (and/or alanine) transaminase in the blood serum on
the 2nd day.
46.IN SOME CASES, THE Q-WAVE ON ECG IS CONSIDERED TO BE PATHOLOGICAL?
a) its amplitude (depth) is greater than 1/4 of the amplitude of the tine's; b) its amplitude exceeds 1/4 of the amplitude of the R wave;
c) its amplitude is less than 1/4 of the amplitude of the R wave; d) right (a) and (b);
e) its duration is greater than 0, 04; f) its duration is 0.02 s.
47.WHAT ARE 3 LABORATORY AND INSTRUMENTAL TEST MAY BE USEFULL TO CONFIRM THE DIAGNOSIS OF ACUTE MYOCARDIAL?
a) defining in the dynamics of leukocyte count and value of the erythrocyte sedimentation rate (a General blood test);
b) determine the dynamics in the number of lymphocytes and platelets (General analysis of blood);
c) the sample with physical exercise (Bicycle ergometry, the test for "treadmill"); d) echocardiography;
e) phonocardiography;
f) radionuclide study of the heart (myocardial scintigraphy).
48.HOW TO CHANGE THE VOLUME OF THE II HEART SOUND IN THE SECOND INTERCOSTAL SPACE TO THE RIGHT OF THE STERNUM IN A PATIENT WITH HYPERTENSION DISEASE?
a) decreases;
b) will increase; c) will not change.
49.WHAT IS THE CHANGE OF THE HEART CAN REVEAL IN A PATIENT WITH HYPERTENSION WHO HAS A LONG HISTORY (SINGLE ANSWER)?
a) left ventricular hypertrophy;
b) hypertrophy of the right ventricle; C) hypertrophy of both ventricles.
93
50. 3 SPECIFY THE CONDITION, THE RISK OF WHICH INCREASES
SUBSTANTIALLY IN PATIENTS WITH HYPERTENSION:
a)chronic inflammatory lung diseases;
b)ischemic heart disease (angina, myocardial infarction);
c)diabetes mellitus;
d)rheumatism;
e)acute violations of cerebral circulation (brain stroke);
f)atherosclerosis of the aorta and its branches;
g)myocarditis.
94

Application
Fig.1. Mitral incompetence
Fig.2. The position of the apical four-chamber hearts: a color Dop pler study of the early diastolic filling of the left v entricle. Registers a unidirectional movement of blood in the pulmonary veins, left atriu m and left ventricle towards the apex o f the heart. LV — left
95
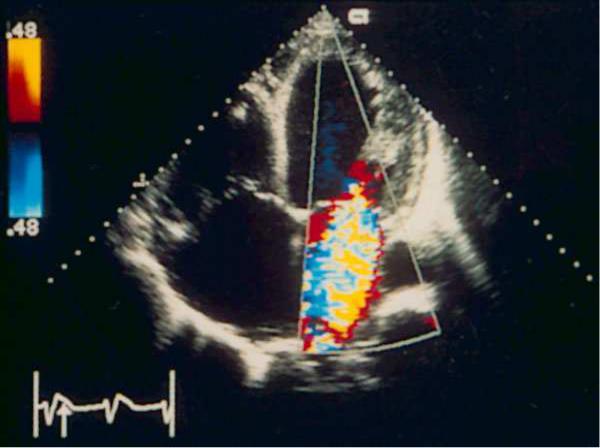
ventricle, LA — left atrium, RV — right ventricle, RA — right atrium, RSPV — right superior pulmonary vein.
Fig.3 The position of the apical four-chamber hearts. Color Doppler study systolic. Severe mitral insufficiency. The jet has a large diameter at the level of the cusps of the mitral valve, the flow reaches the opposite wall of the left atrium occupies almost all the left atrium and enters the pulmonary veins — these trait s characterize severe mitral regurgitation.
96

Fig.4. Mitral stenosis
Fig.5.Aortic incompetence
97
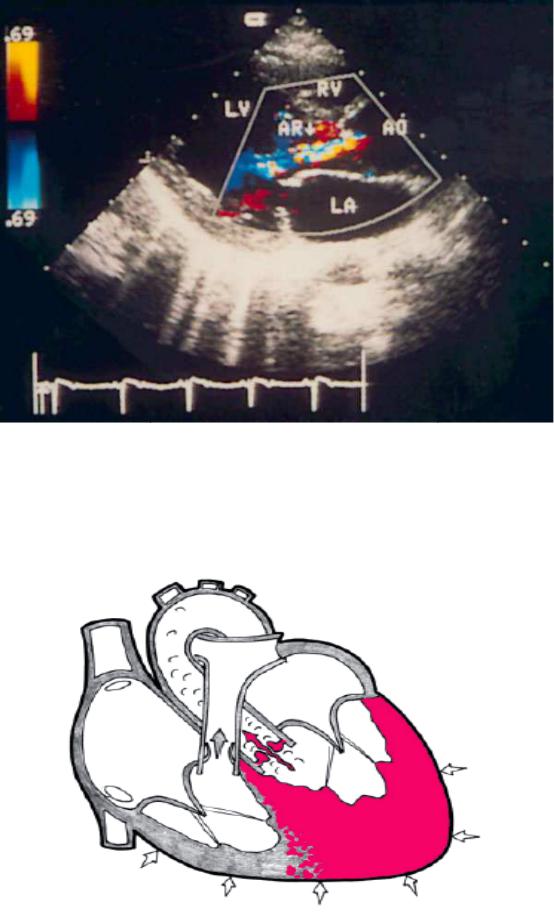
Fig.6. Aortic regurgitation, the severity — from small to moderat e. Color Doppler study of the position of the parasternal long axis of left ventricle. Motley regulatorului flow begins at the level of closin g of the flaps of the aortic valve. LV — left ventricle, LA — left atrium, RV — right ventricle, Ao — ascending aorta, AR — aortic regurgitation.
Fig.7.Aortic stenosis
98
References:
1.Избранные вопросы пропедевтики внутренних болезней: издание для студентов и практикующих врачей. Часть 1/ В.А. Семенов, В.в. гноевых, Е.А.
Черкашина, А.Ю. Смирнова; под. Ред. Проф. В.В. Гноевых.- Ульяновск, 2014.- 208с.
2.Internal diseases propedeutics / Ivashkin V.T., Okhlobystin A.V. - М. : ГЭОТАР-
Медиа, 2014.- 176 с.;
3.Пропедевтика внутренних болезней. Учебно-методическое пособие. Часть VI. Introduction to internal diseases. Manual. Part VI. / Ослопов В.Н., Садыкова А.Р.,
Карамышева И.В. – Казань: КГМУ, 2006. - 75 с.
99
100