


General and Colorectal
CASE 5: SuSpiCiouS mole
history
A 36-year-old Caucasian man presents to his general practitioner concerned that a mole has changed shape and increased in size over the preceding month. It is itchy but has not changed colour or bled. There is no relevant family history. He is fit and well otherwise. As part of his job he spends half the year in California. He smokes five cigarettes per day.
examination
He appears well. Several moles are present over the neck and trunk. All appear benign, except the one he points out that he is concerned about. This is located on the left-hand side of his trunk and is black, measuring 1cm × 1.5cm. The lesion is non-tender with a slightly irregular surface. There is a surrounding pink halo around the lesion. The local lymph nodes are not enlarged. Abdominal, chest and neurological examinations are normal.
Questions
•What is the most likely diagnosis?
•What treatment would you recommend?
•Why is it important to examine the abdomen and chest and assess neurology in such patients?
•What are the risk factors for this condition?
•What factors in the history of such patients would make you concerned?
9
100 Cases in Surgery
ANSWER 5
The patient has malignant melanoma until proven otherwise. An excision biopsy should be recommended with a clear margin of 1–3 mm and full skin thickness. This is then assessed by a histopathologist. If malignant melanoma is confirmed, tumour thickness (Breslow score) and anatomical level of invasion (Clarke’s stage) are ascertained. Both give important prognostic information. Treatment is predominantly surgical with wide local excision. Impalpable lesions should have a 1 cm clear margin and palpable lesions a 2 cm clear margin.
When examining patients with suspicious moles, lymphadenopathy must be sought, as this indicates spread of the malignant melanoma. In such cases, treatment will also include a lymph node dissection +/− radiotherapy, in addition to primary surgical excision. In cases with metastasis, malignant melanoma usually involves the lungs, liver and brain.
!Risk factors for malignant melanoma
•Sun exposure, particularly intermittent
•Fair skin, blue eyes, red or blonde hair
•Dysplastic naevus syndrome
•albinism
•Xeroderma pigmentosum
•Congenital giant hairy naevus
•hutchinson’s freckle
•previous malignant melanoma
•Family history
!Factors in the history that are suggestive of malignant change in a mole
•Change in surface
•itching
•increase in size/shape/thickness
•Change in colour
•bleeding/ulceration
•brown/pink halo (spread into surrounding skin)/satellite nodules
•enlarged local lymph nodes
KEY POINTS
•patients should always be examined for associated lymphadenopathy.
•all specimens should be sent for urgent histological analysis.
10
General and Colorectal
CASE 6: abDominal pain, DiStenSion anD vomiting
history
A 54-year-old man presents to the emergency department with a 4-day history of abdominal distension, central colicky abdominal pain, vomiting and constipation. On further questioning he says he has passed a small amount of flatus yesterday but none today. He has had a previous right-sided hemicolectomy 2 years ago for colonic carcinoma. He lives with his wife and has no known allergies.
examination
His blood pressure and temperature are normal. The pulse is irregularly irregular at 90/min. He has obvious abdominal distension, but the abdomen is only mildly tender centrally. The hernial orifices are clear. There is no loin tenderness and the rectum is empty on digital examination. The bowel sounds are hyperactive and high pitched. Chest examination finds reduced air entry bibasally.

 INVESTIGATIONS
INVESTIGATIONS
|
|
Normal |
haemoglobin |
12.2 g/dl |
11.5–16.0 g/dl |
White cell count |
10.6 × 109/l |
4.0–11.0 × 109/l |
platelets |
435 × 109/l |
150–400 × 109/l |
Sodium |
136 mmol/l |
135–145 mmol/l |
potassium |
3.7 mmol/l |
3.5–5.0 mmol/l |
urea |
6.2 mmol/l |
2.5–6.7 mmol/l |
Creatinine |
77 μmol/l |
44–80 μmol/l |
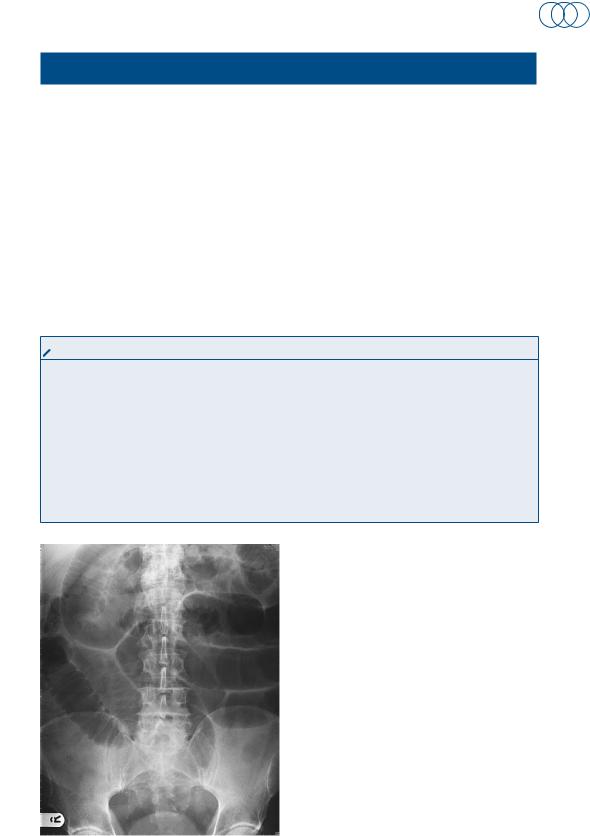
an x-ray of the abdomen is performed and is shown in Figure 6.1.
Questions
• |
What is the diagnosis? |
• |
What features on the x-ray point |
|
towards the diagnosis? |
• |
How should the patient be man- |
|
aged initially? |
• |
What are the common causes of |
|
this condition? |
Figure 6.1 plain x-ray of the abdomen.
11
100 Cases in Surgery
ANSWER 6
The diagnosis is small-bowel obstruction. In this case it is most likely to be secondary to adhesions from his previous abdominal surgery, but may also be due to recurrence of his cancer. Typical features on the x-ray include dilated gas-filled loops of bowel and air-fluid levels. The small bowel is distinguished from the large bowel by its valvular conniventes (radiologically transverse the whole diameter of the bowel). The large bowel has haustral folds, which do not fully transverse the diameter of the bowel. Small-bowel loops usually lie centrally and large-bowel loops lie peripherally. If a patient develops any systemic signs of sepsis or peritonism, then strangulation of the bowel should be considered. If this occurs, the patient will require urgent resuscitation and a laparotomy. If the patient is systemically well, with a diagnosis of adhesional obstruction, then management is as below.
!Initial management
•Keep the patient nil by mouth
•in small-bowel obstruction there is substantial fluid loss and intravenous fluid resuscitation is necessary
•regular observation
•urinary catheter to monitor fluid balance
•Consider central venous line to monitor fluid balance in shocked patients
•pass a nasogastric tube and perform regular aspirates
•Consider high-dependency unit (hDu)/intensive care unit (iCu) transfer for optimization prior to surgery if required
!Aetiology of small-bowel obstruction
•adhesions – common after previous abdominal/gynaecological surgery
•incarcerated herniae, e.g. inguinal, femoral, paraumbilical, spigelian, incisional
•gallstone ileus
•inflammatory bowel disease
•radiation enteritis
•intussusception
KEY POINT
•early nasogastric tube decompression will relieve abdominal distension and prevent vomiting in small-bowel obstruction.
12