

GENERAL AND COLORECTAL
CASE 1: a lump in the groin
history
A 51-year-old woman presents to the emergency department with a painful right groin. She reports lower abdominal distension and has vomited twice on the way to the hospital. She has passed flatus but has not opened her bowels since yesterday. She is otherwise fit and well and is a non-smoker. She lives with her husband and four children.
examination
On examination she appears unwell. Her blood pressure is 106/70 mmHg and the pulse rate is 108/min. She is febrile with a temperature of 38.0°C. The abdomen is tender, particularly in the right iliac fossa, and there is marked lower abdominal distension. There is a small swelling in the right groin, which is originating below and lateral to the pubic tubercle. The lump is irreducible and no cough impulse is present. Digital rectal examination is unremarkable and bowel sounds are hyperactive.
INVESTIGATIONS
|
|
Normal |
haemoglobin |
14.1 g/dl |
11.5–16.0 g/dl |
White cell count |
18.0 × 109/l |
4.0–11.0 × 109/l |
platelets |
361 × 109/l |
150–400 × 109/l |
Sodium |
133 mmol/l |
135–145 mmol/l |
potassium |
3.3 mmol/l |
3.5–5.0 mmol/l |
urea |
6.1 mmol/l |
2.5–6.7 mmol/l |
Creatinine |
63 μmol/l |
44–80 μmol/l |
amylase |
75 iu/l |
0–99 iu/l |
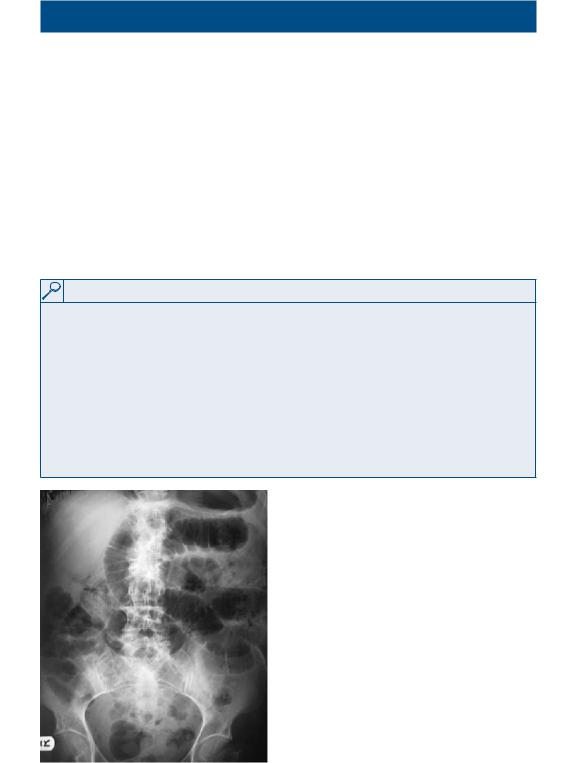
an x-ray of the abdomen is performed and is shown in Figure 1.1.
Questions
• |
What is the cause of the x-ray |
|
appearances? |
• |
What is the swelling? |
• |
What are the anatomical |
|
boundaries? |
• |
What is the initial treatment in |
|
this case? |
• |
What is the differential diagnosis |
|
for a lump in the groin region? |
Figure 1.1 plain x-ray of the abdomen.
1

100 Cases in Surgery
ANSWER 1
This woman has a right-sided femoral hernia. The neck of the femoral hernia lies below and lateral to the pubic tubercle, differentiating it from an inguinal hernia, which lies above and medial to the pubic tubercle. The x-ray shows small-bowel dilation as a result of obstruction due to trapped small bowel in the hernia sac. The high white cell count, temperature and tenderness may indicate strangulation of the hernia contents. The rigid borders of the femoral canal make strangulation more likely than in inguinal hernias.
!Relations of the femoral canal
•Anteriorly: inguinal ligament
•Posteriorly: superior ramus of the pubis and pectineus muscle
•Medially: body of pubis, pubic part of the inguinal ligament
•Laterally: femoral vein
The patient should be kept nil by mouth, and intravenous fluids and antibiotics begun. A nasogastric tube should be passed and bloods taken in preparation for theatre. Theatres should then be informed and the patient taken for urgent surgery to reduce and repair the hernia, with careful inspection of the hernial sac contents. If the bowel is infarcted, it will need to be resected.
!Differential diagnosis for a lump in the groin
•inguinal hernia
•Femoral hernia
•hydrocoele of the cord
•hydrocoele of the canal of nuck
•lipoma of the cord
•undescended testicle
•ectopic testicle
•Saphena varix
•iliofemoral aneurysm
•lymph nodes
•psoas abscess
KEY POINTS
•Femoral hernias are at high risk of strangulation.
•if strangulation is suspected, urgent surgical correction is required.
2
General and Colorectal
CASE 2: right iliaC FoSSa pain
history
A 19-year-old man presents with a 2-day history of abdominal pain. The pain started in the central abdomen and has now become constant and has shifted to the right iliac fossa. The patient has vomited twice today and is off his food. His motions were loose today, but there was no associated rectal bleeding.
examination
The patient has a temperature of 37.8°C and a pulse rate of 110/min. On examination of his abdomen, he has localized tenderness and guarding in the right iliac fossa. Urinalysis is clear.
INVESTIGATIONS
|
|
Normal |
haemoglobin |
14.2 g/dl |
11.5–16.0 g/dl |
mean cell volume |
86 fl |
76–96 fl |
White cell count |
19 × 109/l |
4.0–11.0 × 109/l |
platelets |
250 × 109/l |
150–400 × 109/l |
Sodium |
136 mmol/l |
135–145 mmol/l |
potassium |
3.5 mmol/l |
3.5–5.0 mmol/l |
urea |
5.0 mmol/l |
2.5–6.7 mmol/l |
Creatinine |
62 μmol/l |
44–80 μmol/l |
C-reactive protein (Crp) |
20 mg/l |
<5 mg/l |
Questions
•What is the likely diagnosis?
•What are the differential diagnoses for this condition?
•How would you manage this patient?
•What are the complications of any surgical intervention that may be required?
3

100 Cases in Surgery
ANSWER 2
The history and the findings on examination strongly suggest acute appendicitis.
!Differential diagnoses of acute appendicitis
•mmesenteric adenitis
•psoas abscess
•meckel’s diverticulitis
•Crohn’s ileitis
•non-specific abdominal pain
and additionally in females:
•ovarian cyst rupture
•ovarian torsion
•ectopic pregnancy (all females must have a pregnancy test)
The treatment is appendicectomy. The patient should be rehydrated with preoperative intravenous fluids, and receive analgesia. Antibiotics should be given if the diagnosis is clear and the decision for surgery has been made. Surgery should be carried out promptly in a patient who has signs of peritonitis, in order to avoid systemic toxicity. The appendix can be removed by open operation or laparoscopically.
!Complications
•Wound infection: reduced by using broad-spectrum antibiotics
•intra-abdominal collections and pelvic abscesses
•prolonged ileus
•Fistulation between the appendix stump and the wound
•Deep vein thrombosis, pulmonary embolism, pneumonia, atelectasis
•late complications: incisional hernia, adhesional obstruction
KEY POINT
•if the appendix is normal at the time of the operation, the small bowel should be inspected for the presence of a meckel’s diverticulum.
4