


100 Cases in Surgery
ANSWER 32
The patient has chronic pancreatitis. The x-ray demonstrates pancreatic calcification (arrow in Figure 32.2).
Figure 32.2 plain x-ray of the abdomen. arrow shows pancreatic calcification.
Chronic pancreatitis is an irreversible inflammation causing pancreatic fibrosis and calcification. Patients usually present with chronic abdominal pain and normal or mildly elevated pancreatic enzyme levels. The pancreas may have lost its endocrine and exocrine function, leading to diabetes mellitus and steatorrhea.
!Causes of chronic pancreatitis
•Alcohol dependence: most common cause
•Idiopathic: approximately 30 per cent of cases
•Cholelithiasis: this is the most common cause of acute pancreatitis, but it is associated with chronic pancreatitis in less than 25 per cent of cases
•Pancreatic duct strictures
•Pancreatic trauma
•Hereditary pancreatitis: mutations in the gene for cationic trypsinogen on chromosome 7 appear to be involved in 60–75 per cent of cases of hereditary pancreatitis
•Recurrent acute pancreatitis
•Cystic fibrosis: an autosomal recessive disorder accounting for a small percentage of patients with chronic pancreatitis
•Congenital causes: pancreas divisum can cause chronic pancreatitis, although this is rare
•Autoimmune disorders: Sjögren’s syndrome, primary biliary cirrhosis, and renal tubular acidosis
•Other conditions: hyperlipidaemia, hyperparathyroidism, and uraemia can cause chronic pancreatitis
72
Upper Gastrointestinal
Diagnostic studies may be normal in the early stages of chronic pancreatitis. The inflammatory changes can only be diagnosed on histological analysis of a biopsy. The mean age of onset is 40 years, with a male preponderance of 4:1. Pancreatic calcification is observed in approximately one-third of plain x-rays of patients with chronic pancreatitis (arrow in Figure 32.2). ERCP provides an accurate visualization of the pancreatic ductal system and is useful for diagnosing chronic pancreatitis. One limitation of ERCP is that it cannot be used to evaluate the pancreatic parenchyma, and histologically proven chronic pancreatitis can be found after a normal ERCP. MRCP imaging provides information on the pancreatic parenchyma and adjacent abdominal viscera. Pancreatic function tests can provide useful information using the serum trypsin or faecal fat levels.
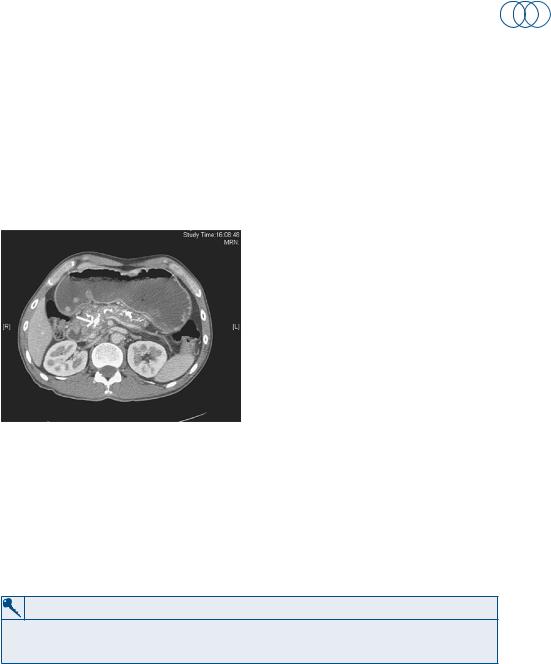
Figure 32.3 Computerized tomography showing changes consistent with chronic pancreatitis.
Treatment should primarily be a low-fat diet and abstinence from alcohol. Pancreatic enzyme supplements (creon) may reduce steatorrhoea. If conventional medical therapy is unsuccessful and the patient has severe intractable pain, coeliac ganglion blockade can be considered. Surgery is associated with significant morbidity and mortality and relieves symptoms in approximately 75 per cent of patients. It does not result in the return of normal endocrine and exocrine function. Surgery can be performed to bypass an obstructing lesion (pancreaticojejunostomy) or to remove the damaged gland (pancreaticoduodenectomy or distal pancreatectomy).
KEY POINTS
•thirty per cent of cases of chronic pancreatitis are idiopathic.
•Chronic pancreatitis increases the risk of pancreatic carcinoma.
73
This page intentionally left blank

Upper Gastrointestinal
CASE 33: abDominal pain anD jaunDiCe
history
A GP has referred a 64-year-old woman to the general surgical team on call. She has been complaining of pain in the upper part of the abdomen and generalized itching. Her daughter has also noticed a yellowish discolouration of her skin. The symptoms began about a week ago and became gradually worse. On further questioning she reports passing dark urine and pale stools for the last few days. She is usually fit and well, does not drink alcohol and denies any recent foreign travel.
examination
The patient is clinically jaundiced and tender in the right upper abdomen. The liver is not enlarged and rectal examination reveals pale stool on the glove. Her temperature is 37°C, blood pressure 130/80 mmHg and pulse rate 72/min. Bilirubin is detected on urinalysis.
INVESTIGATIONS
|
|
Normal |
haemoglobin |
12 g/dl |
11.5–16.0 g/dl |
mean cell volume |
80 fl |
76–96 fl |
White cell count |
11.5 × 109/l |
4.0–11.0 × 109/l |
platelets |
315 × 109/l |
150–400 × 109/l |
Sodium |
137 mmol/l |
135–145 mmol/l |
potassium |
4.2 mmol/l |
3.5–5.0 mmol/l |
urea |
6 mmol/l |
2.5–6.7 mmol/l |
Creatinine |
62 μmol/l |
44–80 μmol/l |
amylase |
72 iu/dl |
0–100 iu/dl |
alp |
556 iu/l |
35–110 iu/l |
aSt |
45 iu/l |
5–35 iu/l |
ggt |
127 iu/l |
11–51 iu/l |
albumin |
38 g/l |
35–50 g/l |
bilirubin |
122 mmol/l |
3–17 mmol/l |
Questions
•What do the blood results show?
•What are the causes of this condition?
•What are the options for investigation and treatment?
75